

46ff6207a22f3be1e477300a27e15967.ppt
- Количество слайдов: 41
 Pain in Cancer, AIDS, and NCDs, with a Focus on Opioid Analgesics James Cleary, MD Pain and Policy Studies Group
Pain in Cancer, AIDS, and NCDs, with a Focus on Opioid Analgesics James Cleary, MD Pain and Policy Studies Group
 Uganda as a model! • Uganda serves as a brilliant model, like Wisconsin and Catalonia, for the importance of an integrated government and community non-governmental approach. Each one by themselves in isolation, will not achieve much. Oxford Textbook of Palliative Medicine, 3 rd Edition
Uganda as a model! • Uganda serves as a brilliant model, like Wisconsin and Catalonia, for the importance of an integrated government and community non-governmental approach. Each one by themselves in isolation, will not achieve much. Oxford Textbook of Palliative Medicine, 3 rd Edition
 • US based:") Wisconsin Cancer Pain Initiative • Dahl & Joranson (WI Pharmacy Board) • US based: 1986 – WHO Demonstration Project. – Role Model Initiative. – Education • Wisconsin Pain Initiative – Alliance of State Pain Initiatives.
Wisconsin Cancer Pain Initiative • Dahl & Joranson (WI Pharmacy Board) • US based: 1986 – WHO Demonstration Project. – Role Model Initiative. – Education • Wisconsin Pain Initiative – Alliance of State Pain Initiatives.
 Pain and Policy Study Group • 1996: Pain and Policy Study Group – National – International • WHO Collaborating Center – Cancer Control – Access to Controlled Medications Program • INCB Workshop Estimates; Dec 2009 • Close Ties with INCB – Opioid Consumption Data – Model Laws – Estimates Process
Pain and Policy Study Group • 1996: Pain and Policy Study Group – National – International • WHO Collaborating Center – Cancer Control – Access to Controlled Medications Program • INCB Workshop Estimates; Dec 2009 • Close Ties with INCB – Opioid Consumption Data – Model Laws – Estimates Process
 Establishes a Framework to: 1. Prevent abuse and diversion, and 2. Ensure the availability of drugs for medical purposes
Establishes a Framework to: 1. Prevent abuse and diversion, and 2. Ensure the availability of drugs for medical purposes
 Global Trend 1980 - 2008 Source: International Narcotics Control Board By: Pain & Policy Studies Group, University of Wisconsin/WHO Collaborating Center, 2010
Global Trend 1980 - 2008 Source: International Narcotics Control Board By: Pain & Policy Studies Group, University of Wisconsin/WHO Collaborating Center, 2010
 Total ME: High Income vs. Low and Middle Income Countries Source: International Narcotics Control Board By: Pain & Policy Studies Group, University of Wisconsin/WHO Collaborating Center, 2010
Total ME: High Income vs. Low and Middle Income Countries Source: International Narcotics Control Board By: Pain & Policy Studies Group, University of Wisconsin/WHO Collaborating Center, 2010
 2006 International Pain Policy Fellowship Dr. Simbo Daisy Amanor-Boadu Dr. Henry Ddungu Uganda/APCA Nigeria Prof. Snežana Bošnjak Dr. Jorge Eisenchlas Serbia Argentina Prof. Rosa Buitrago Dr. Marta Ximena León Republic of Panama Colombia Mrs. Nguyen Thi Phuong Cham Vietnam Pain & Policy Studies Group Supported by the University of Wisconsin Open Society Institute October 2006 Madison, Wisconsin Mr. Gabriel Madiye Sierra Leone
2006 International Pain Policy Fellowship Dr. Simbo Daisy Amanor-Boadu Dr. Henry Ddungu Uganda/APCA Nigeria Prof. Snežana Bošnjak Dr. Jorge Eisenchlas Serbia Argentina Prof. Rosa Buitrago Dr. Marta Ximena León Republic of Panama Colombia Mrs. Nguyen Thi Phuong Cham Vietnam Pain & Policy Studies Group Supported by the University of Wisconsin Open Society Institute October 2006 Madison, Wisconsin Mr. Gabriel Madiye Sierra Leone
 2008 International Pain Policy Fellowship Dr. Dingle Spence Mrs. Verna Walker. Edwards Dr. Hrant Karapetyan Dr. Irina Kazaryan Armenia Jamaica Dr. Pati Dzotsenidze Mr. Mikheil Pavliashvili Dr. Zippy Ali Dr. Jacinta Wasike Georgia Kenya Dr. Eva Rossina Duarte Juárez Lic. Ana Lucía Arango Espigares Dr. Adrian Belîi Republic of Moldova Guatemala Dr. Bishnu Dutta Paudel Mr. Radha Raman Prasad Teli Nepal Pain & Policy Studies Group Supported by the University of Wisconsin Open Society Institute October 2006 Madison, Wisconsin
2008 International Pain Policy Fellowship Dr. Dingle Spence Mrs. Verna Walker. Edwards Dr. Hrant Karapetyan Dr. Irina Kazaryan Armenia Jamaica Dr. Pati Dzotsenidze Mr. Mikheil Pavliashvili Dr. Zippy Ali Dr. Jacinta Wasike Georgia Kenya Dr. Eva Rossina Duarte Juárez Lic. Ana Lucía Arango Espigares Dr. Adrian Belîi Republic of Moldova Guatemala Dr. Bishnu Dutta Paudel Mr. Radha Raman Prasad Teli Nepal Pain & Policy Studies Group Supported by the University of Wisconsin Open Society Institute October 2006 Madison, Wisconsin
 WHO Palliative Care Public Health Model Drug Availability Education Policy
WHO Palliative Care Public Health Model Drug Availability Education Policy
 “the medical use of narcotic drugs continues to be indispensable for the relief of pain and suffering… adequate provision must be made to ensure the availability of narcotic drugs for such purposes. ” (Preamble, p. 13)
“the medical use of narcotic drugs continues to be indispensable for the relief of pain and suffering… adequate provision must be made to ensure the availability of narcotic drugs for such purposes. ” (Preamble, p. 13)
") • • • Measurement Sustainable delivery systems Tobacco, obesity, alcohol Vaccination (HBV, HPV) Dispel myths about cancer Screening & early detection Effective pain control Training opportunities Reduce health emigration Improve cancer survival for all. 2020 Targets
• • • Measurement Sustainable delivery systems Tobacco, obesity, alcohol Vaccination (HBV, HPV) Dispel myths about cancer Screening & early detection Effective pain control Training opportunities Reduce health emigration Improve cancer survival for all. 2020 Targets
 • 7: Improve Access to Diagnosis, Treatment, Rehabilitation and Palliative Care Access to accurate cancer diagnosis, appropriate cancer treatments, supportive care, rehabilitation services and palliative care will have improved for all patients worldwide. • 8: Effective pain control measures will be available universally to all cancer patients in pain
• 7: Improve Access to Diagnosis, Treatment, Rehabilitation and Palliative Care Access to accurate cancer diagnosis, appropriate cancer treatments, supportive care, rehabilitation services and palliative care will have improved for all patients worldwide. • 8: Effective pain control measures will be available universally to all cancer patients in pain
 1274 27. 5
1274 27. 5
 Deaths from HIV & Cancer
Deaths from HIV & Cancer
 Noncommunicable diseases: Infectious diseases: HIV/AIDS 4. 9%") Deaths by cause in the world (2005) Noncommunicable diseases: Infectious diseases: HIV/AIDS 4. 9% Tuberculosis 2. 4% Heart disease 30. 2% Malaria 1. 5% Total: 58. 2 M Cancer 15. 7% Diabetes 1. 9% Other chronic diseases 15. 7% (WHO, Chronic Disease Report, 2005) Other Infectious Diseases 20. 9% Injuries 9. 3%
Deaths by cause in the world (2005) Noncommunicable diseases: Infectious diseases: HIV/AIDS 4. 9% Tuberculosis 2. 4% Heart disease 30. 2% Malaria 1. 5% Total: 58. 2 M Cancer 15. 7% Diabetes 1. 9% Other chronic diseases 15. 7% (WHO, Chronic Disease Report, 2005) Other Infectious Diseases 20. 9% Injuries 9. 3%
 • Responsible for up to 60% of all deaths, • 80%") Noncommunicable Diseases (NCDs) • Responsible for up to 60% of all deaths, • 80% are in low- and middle-income countries • Major non-communicable diseases: – Cardiovascular disease Diabetes – Cancer – Chronic Respiratory disease Cardiovascular Disease – Diabetes • Shared preventable risk factors: – Tobacco use – Unhealthy diet – Physical inactivity – Harmful use of alcohol Cancer Other NCDs Physical inactivity Obesity Chronic Respiratory Diseases Unhealthy diets Smoking Harmful use of alcohol
Noncommunicable Diseases (NCDs) • Responsible for up to 60% of all deaths, • 80% are in low- and middle-income countries • Major non-communicable diseases: – Cardiovascular disease Diabetes – Cancer – Chronic Respiratory disease Cardiovascular Disease – Diabetes • Shared preventable risk factors: – Tobacco use – Unhealthy diet – Physical inactivity – Harmful use of alcohol Cancer Other NCDs Physical inactivity Obesity Chronic Respiratory Diseases Unhealthy diets Smoking Harmful use of alcohol
 2005 Geographical regions (WHO classification) 2006 -2015 (cumulative) Total deaths") Noncommunicable diseases (2006 -2015) 2005 Geographical regions (WHO classification) 2006 -2015 (cumulative) Total deaths (millions) NCD deaths (millions) Trend: Death from infectious disease Trend: Death from NCD Africa 10. 8 2. 5 28 +6% +27% Americas 6. 2 4. 8 53 -8% +17% Eastern Mediterranean 4. 3 2. 2 25 -10% +25% Europe 9. 8 8. 5 88 +7% +4% South-East Asia 14. 7 8. 0 89 -16% +21% Western Pacific 12. 4 9. 7 105 +1 +20% Total 58. 2 35. 7 388 -3% +17% WHO projects that over the next 10 years, the largest increase in deaths from cardiovascular disease, cancer, respiratory disease and diabetes will occur in low- and middle-income countries. (WHO, Chronic Disease Report, 2005)
Noncommunicable diseases (2006 -2015) 2005 Geographical regions (WHO classification) 2006 -2015 (cumulative) Total deaths (millions) NCD deaths (millions) Trend: Death from infectious disease Trend: Death from NCD Africa 10. 8 2. 5 28 +6% +27% Americas 6. 2 4. 8 53 -8% +17% Eastern Mediterranean 4. 3 2. 2 25 -10% +25% Europe 9. 8 8. 5 88 +7% +4% South-East Asia 14. 7 8. 0 89 -16% +21% Western Pacific 12. 4 9. 7 105 +1 +20% Total 58. 2 35. 7 388 -3% +17% WHO projects that over the next 10 years, the largest increase in deaths from cardiovascular disease, cancer, respiratory disease and diabetes will occur in low- and middle-income countries. (WHO, Chronic Disease Report, 2005)
 • For the first time ever,") United Nations general assembly on non-communicable diseases (NCD) • For the first time ever, the United Nations General Assembly held a Non-communicable Disease (NCD) Summit involving Heads of State, in September 2011, to address the threat posed by NCDs to low- & middleincome countries (LMICs). • • World Heart Federation International Diabetes Federation (IDF) International Union Against Cancer (UICC) the International Union Against Tuberculosis and Lung Disease • Where was PAIN? ? ?
United Nations general assembly on non-communicable diseases (NCD) • For the first time ever, the United Nations General Assembly held a Non-communicable Disease (NCD) Summit involving Heads of State, in September 2011, to address the threat posed by NCDs to low- & middleincome countries (LMICs). • • World Heart Federation International Diabetes Federation (IDF) International Union Against Cancer (UICC) the International Union Against Tuberculosis and Lung Disease • Where was PAIN? ? ?
 World Health Organization
World Health Organization
 2010 WHO Model List 2. ANALGESICS, ANTIPYRETICS, NON-STEROIDAL") Essential Medicines 16 th edition (updated) 2010 WHO Model List 2. ANALGESICS, ANTIPYRETICS, NON-STEROIDAL ANTI-INFLAMMATORY MEDICINES (NSAIMs), MEDICINES USED TO TREAT GOUT AND DISEASE MODIFYING AGENTS IN RHEUMATOID DISORDERS (DMARDs) 2. 1 Non-opioids and non-steroidal anti-inflammatory medicines (NSAIMs) acetylsalicylic acid Suppository: 50 mg to 150 mg. Tablet: 100 mg to 500 mg. Ibuprofen Tablet: 200 mg; 400 mg. >3 months. paracetamol* Oral liquid: 125 mg/5 ml. Suppository: 100 mg. Tablet: 100 mg to 500 mg. * Not recommended for anti‐inflammatory use due to lack of proven benefit to that effect. 2. 2 Opioid analgesics Codeine Morphine Tablet: 15 mg (phosphate); 30 mg (phosphate). Injection: 10 mg (morphine hydrochloride or morphine sulfate) in 1‐ml ampoule. Oral liquid: 10 mg (morphine hydrochloride or morphine sulfate)/5 ml. Tablet: 10 mg (morphine sulfate). Tablet (prolonged release): 10 mg; 30 mg; 60 mg (morphine sulfate)
Essential Medicines 16 th edition (updated) 2010 WHO Model List 2. ANALGESICS, ANTIPYRETICS, NON-STEROIDAL ANTI-INFLAMMATORY MEDICINES (NSAIMs), MEDICINES USED TO TREAT GOUT AND DISEASE MODIFYING AGENTS IN RHEUMATOID DISORDERS (DMARDs) 2. 1 Non-opioids and non-steroidal anti-inflammatory medicines (NSAIMs) acetylsalicylic acid Suppository: 50 mg to 150 mg. Tablet: 100 mg to 500 mg. Ibuprofen Tablet: 200 mg; 400 mg. >3 months. paracetamol* Oral liquid: 125 mg/5 ml. Suppository: 100 mg. Tablet: 100 mg to 500 mg. * Not recommended for anti‐inflammatory use due to lack of proven benefit to that effect. 2. 2 Opioid analgesics Codeine Morphine Tablet: 15 mg (phosphate); 30 mg (phosphate). Injection: 10 mg (morphine hydrochloride or morphine sulfate) in 1‐ml ampoule. Oral liquid: 10 mg (morphine hydrochloride or morphine sulfate)/5 ml. Tablet: 10 mg (morphine sulfate). Tablet (prolonged release): 10 mg; 30 mg; 60 mg (morphine sulfate)
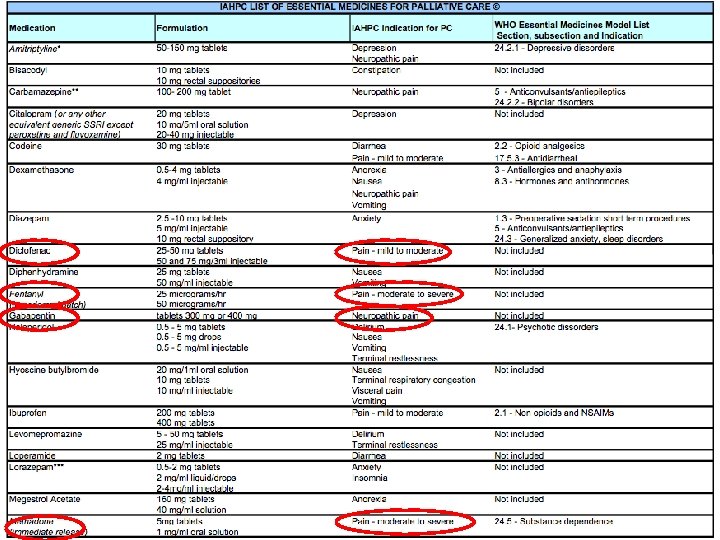
 International Association of Hospice and Palliative Care List of Essential Medicines for Palliative Care (http: //www. hospicecare. com/resources/pdf-docs/iahpc-list-em. pdf) ü Codeine, ü Fentanyl, ü Methadone, ü Morphine (immediate and sustained release), ü Oxycodone, ü Tramadol NOTE: NO GOVERNMENT SHOULD APPROVE MODIFIED RELEASE MORPHINE, FENTANYL OR OXYCODONE WITHOUT ALSO GUARANTEEING WIDELY AVAILABLE NORMAL RELEASE ORAL MORPHINE.
International Association of Hospice and Palliative Care List of Essential Medicines for Palliative Care (http: //www. hospicecare. com/resources/pdf-docs/iahpc-list-em. pdf) ü Codeine, ü Fentanyl, ü Methadone, ü Morphine (immediate and sustained release), ü Oxycodone, ü Tramadol NOTE: NO GOVERNMENT SHOULD APPROVE MODIFIED RELEASE MORPHINE, FENTANYL OR OXYCODONE WITHOUT ALSO GUARANTEEING WIDELY AVAILABLE NORMAL RELEASE ORAL MORPHINE.

 WHO supports global effort to relieve chronic pain • The WHO co-sponsors the first Global Day Against Pain, which seeks to draw global attention to the urgent need for better pain relief for sufferers from diseases such as cancer and AIDS. • The campaign, organised by the International Association on the Study of Pain (IASP) & the European Federation of the IASP Chapters (EFIC), asks for recognition that pain relief is integral to the right to the highest attainable level of physical and mental health…
WHO supports global effort to relieve chronic pain • The WHO co-sponsors the first Global Day Against Pain, which seeks to draw global attention to the urgent need for better pain relief for sufferers from diseases such as cancer and AIDS. • The campaign, organised by the International Association on the Study of Pain (IASP) & the European Federation of the IASP Chapters (EFIC), asks for recognition that pain relief is integral to the right to the highest attainable level of physical and mental health…
 Report on AVAILABILITY “The low levels of consumption of opioid analgesics for the treatment of pain in many countries, in particular in developing countries, continue to be a matter of serious concern to the Board. The Board again urges all Governments concerned to identify the impediments in their countries to adequate use of opioid analgesics for the treatment of pain and to take steps to improve the availability of those narcotic drugs for medical purposes…” (paragraph 97) INCB, 2007 report
Report on AVAILABILITY “The low levels of consumption of opioid analgesics for the treatment of pain in many countries, in particular in developing countries, continue to be a matter of serious concern to the Board. The Board again urges all Governments concerned to identify the impediments in their countries to adequate use of opioid analgesics for the treatment of pain and to take steps to improve the availability of those narcotic drugs for medical purposes…” (paragraph 97) INCB, 2007 report
 Opioid availability and cost: West Europe Codeine Propox HC/DHC Bupr. PO Bupr. TD Mo. IR Mo. CR Mo. Inj Oc. IR Oc. CR Methad. Fent. TD Fent. TM Hm. IR Hm. CR Peth. Inj Finland France Norway Austria Portugal Italy Denmark Israel Netherlands Cyprus Greece Germany Luxemburg Spain Switzerland UK Belgium Iceland Turkey Free <25% Cost 25 -50% Cost 50 -75% Cost 100% cost
Opioid availability and cost: West Europe Codeine Propox HC/DHC Bupr. PO Bupr. TD Mo. IR Mo. CR Mo. Inj Oc. IR Oc. CR Methad. Fent. TD Fent. TM Hm. IR Hm. CR Peth. Inj Finland France Norway Austria Portugal Italy Denmark Israel Netherlands Cyprus Greece Germany Luxemburg Spain Switzerland UK Belgium Iceland Turkey Free <25% Cost 25 -50% Cost 50 -75% Cost 100% cost
 Opioid availability and cost: Eastern Europe Czech R. Croatia Latvia Rumania Slovak R. Hungary Estonia Serbia Bulgaria Moldova Poland Russia Monten. Maced. Bosnia-H Lithuania Belarus Albania Georgia Ukraine Codeine Propox HC/DHC Bupr. PO Bupr. TD Mo. IR Mo. CR Mo. Inj Oc. IR Oc. CR Methad. Fent. TD Fent. TM Hm. IR Hm. CR Peth. Inj Free <25% Cost 25 -50% Cost 50 -75% cost 100% cost
Opioid availability and cost: Eastern Europe Czech R. Croatia Latvia Rumania Slovak R. Hungary Estonia Serbia Bulgaria Moldova Poland Russia Monten. Maced. Bosnia-H Lithuania Belarus Albania Georgia Ukraine Codeine Propox HC/DHC Bupr. PO Bupr. TD Mo. IR Mo. CR Mo. Inj Oc. IR Oc. CR Methad. Fent. TD Fent. TM Hm. IR Hm. CR Peth. Inj Free <25% Cost 25 -50% Cost 50 -75% cost 100% cost
 Global Consumption of Morphine High-Income vs. Low - and Middle - Income Countries, 2008 Percent total 91% 83% 17% 9% Source: International Narcotics Control Board; United Nations Population Data, 2007; World Bank Income Classification, 2008. By: Pain & Policy Studies Group, University of Wisconsin /WHO Collaborating Center, 2010.
Global Consumption of Morphine High-Income vs. Low - and Middle - Income Countries, 2008 Percent total 91% 83% 17% 9% Source: International Narcotics Control Board; United Nations Population Data, 2007; World Bank Income Classification, 2008. By: Pain & Policy Studies Group, University of Wisconsin /WHO Collaborating Center, 2010.
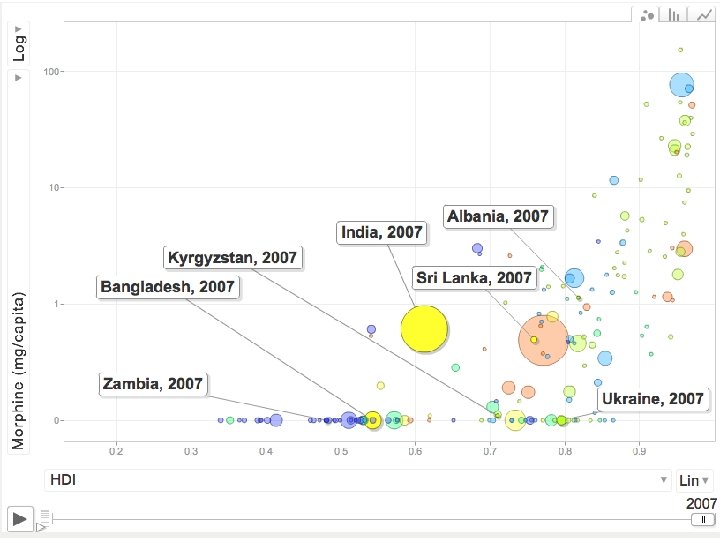
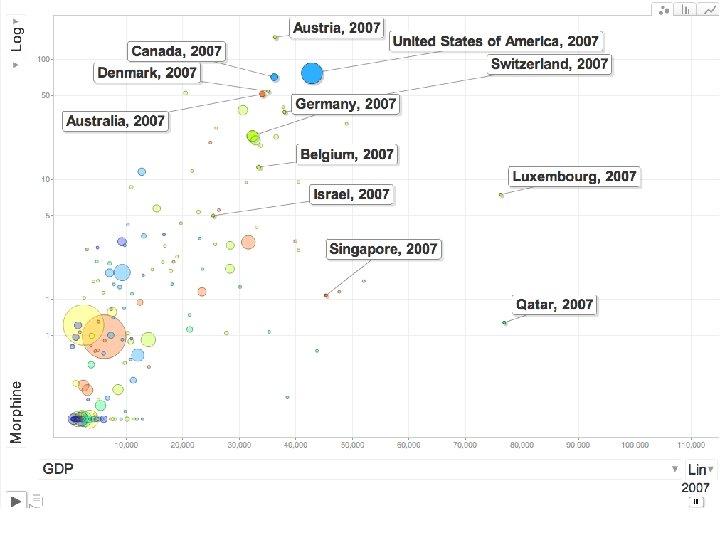
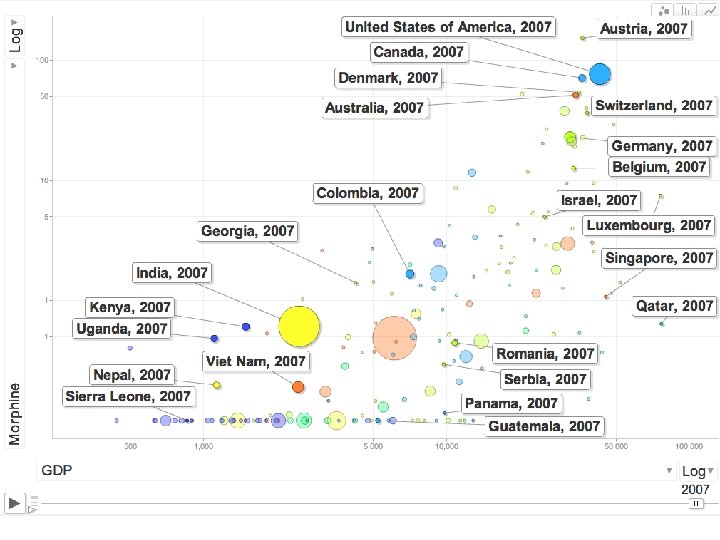
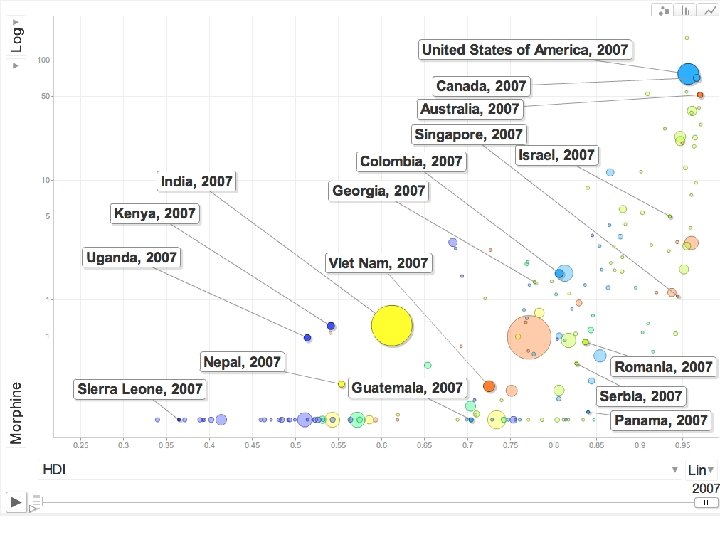
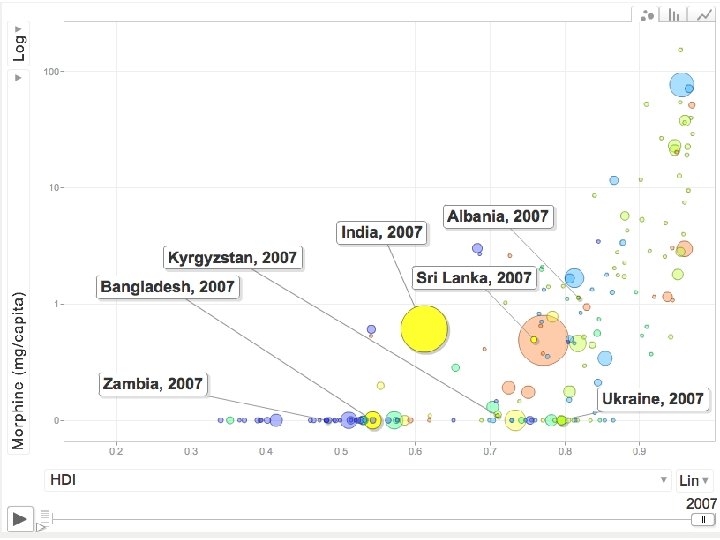
 Global Consumption of Morphine, 2008 Mg/capita Global mean 0. 6945 mg Georgia Uses morphine for substitution treatment 5. 9847 mg Armenia Austria (166. 9070 mg) 1. 338 mg Guatemala 0. 3561 mg Jamaica 1. 3652 mg Kenya 0. 1292 mg Nepal 0. 0349 mg Colombia 1. 2390 mg Panama U. S. A (66. 5682 mg) Sierra Leone Global Mean N/A Serbia Italy (3. 4816 mg) 0. 6659 Vietnam (6. 005 mg) Poland (6. 4746 mg) South Africa (10. 3011 mg) 0. 5170 0. 2193 Guatemala Georgia Armenia Serbia Kenya Vietnam Jamaica Colombia Nepal Panama (158 Countries) Source: International Narcotics Control Board; United Nations population data By: Pain & Policy Studies Group, University of Wisconsin/WHO Collaborating Center, 2010 The means are calculated by adding the individual mg/capita statistics for all countries and then dividing by the number of countries; data does not Include information for countries from which the INCB did not receive a report
Global Consumption of Morphine, 2008 Mg/capita Global mean 0. 6945 mg Georgia Uses morphine for substitution treatment 5. 9847 mg Armenia Austria (166. 9070 mg) 1. 338 mg Guatemala 0. 3561 mg Jamaica 1. 3652 mg Kenya 0. 1292 mg Nepal 0. 0349 mg Colombia 1. 2390 mg Panama U. S. A (66. 5682 mg) Sierra Leone Global Mean N/A Serbia Italy (3. 4816 mg) 0. 6659 Vietnam (6. 005 mg) Poland (6. 4746 mg) South Africa (10. 3011 mg) 0. 5170 0. 2193 Guatemala Georgia Armenia Serbia Kenya Vietnam Jamaica Colombia Nepal Panama (158 Countries) Source: International Narcotics Control Board; United Nations population data By: Pain & Policy Studies Group, University of Wisconsin/WHO Collaborating Center, 2010 The means are calculated by adding the individual mg/capita statistics for all countries and then dividing by the number of countries; data does not Include information for countries from which the INCB did not receive a report

 "We must not only stop the harm caused by drugs: let's unleash the capacity of drugs to do good. You think this is a radical idea? Look back to the origins of drug control. The Preamble of the Single Convention recognizes that … the medical use of narcotic drugs continues to be indispensable for the relief of pain… This is hardly the language of a prohibitionist regime. Indeed, this noble goal of UN drug policy, the freedom from physical pain, demonstrates our over-riding commitment to health. " Antonio Costa, Exec Director, UN Office on Drugs and Crime (UNODC) March 2010
"We must not only stop the harm caused by drugs: let's unleash the capacity of drugs to do good. You think this is a radical idea? Look back to the origins of drug control. The Preamble of the Single Convention recognizes that … the medical use of narcotic drugs continues to be indispensable for the relief of pain… This is hardly the language of a prohibitionist regime. Indeed, this noble goal of UN drug policy, the freedom from physical pain, demonstrates our over-riding commitment to health. " Antonio Costa, Exec Director, UN Office on Drugs and Crime (UNODC) March 2010