JAUNDICE lecture.ppt
- Количество слайдов: 62



OBSTRUCTIVE JAUNDICE DR. JAMIL SAWAKED

DEFITION OF JAUNDICE l l l YELLOW DISCOLOURATION OF SKIN AND MUCOUS MEMBRANE Clinically evident when bilirubin is more than 2. 5 mg/dl Normal bilirubin 0. 2 -1. 2 mg /dl

TYPES A PREHEPATIC POSTHEPATIC OBSTRUCTIVE OR SURGICAL HAEMOLYSIS

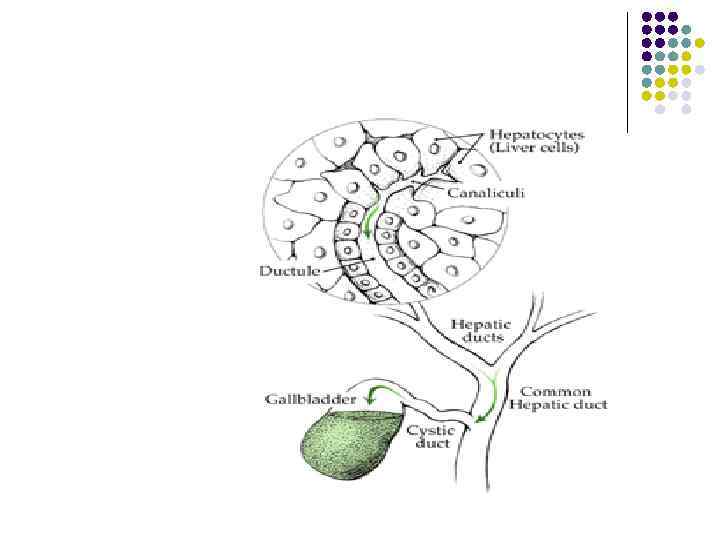
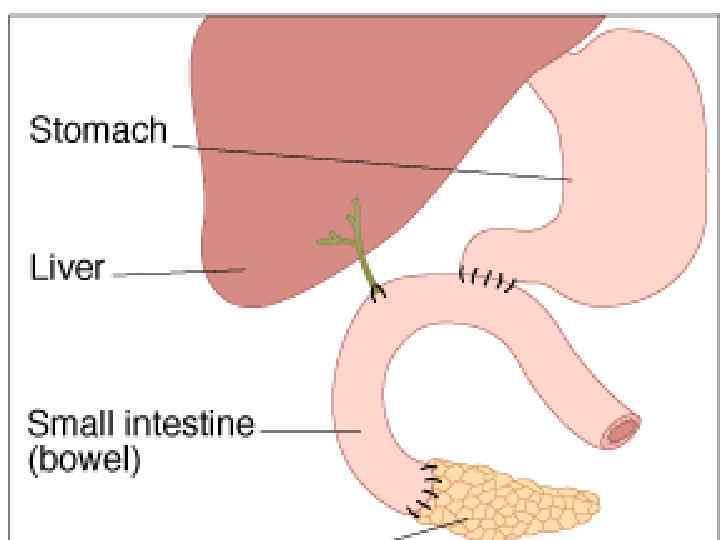
ANATOMY

ANATOMY A

BILIRUBIN CYCLE l l BROKEN DOWN RED CELLS ARE REMOVED BY R. E. S. HAEMOGLOBIN SPLITS INTO HAEM &GLOBIN & CELL WALL PROTEIN GO DOWN TO AMINOACIDS THEY ENTER THE AMINO ACID POOL
![BILIRUBIN CYCLE CONTINUE HAEM SPLITS INTO IRON BILIRUBIN [pigments] & IRON STORED AS FERRITIN](https://present5.com/presentation/79468405_187640252/image-8.jpg "BILIRUBIN CYCLE CONTINUE HAEM SPLITS INTO IRON BILIRUBIN [pigments] & IRON STORED AS FERRITIN")
BILIRUBIN CYCLE CONTINUE HAEM SPLITS INTO IRON BILIRUBIN [pigments] & IRON STORED AS FERRITIN FOR REUSE
![BILIRUBIN IS NOT REUSED [GOES TO THE LIVER] l COMBINE WITH GLUCOURINC ACID TO](https://present5.com/presentation/79468405_187640252/image-9.jpg "BILIRUBIN IS NOT REUSED [GOES TO THE LIVER] l COMBINE WITH GLUCOURINC ACID TO")
BILIRUBIN IS NOT REUSED [GOES TO THE LIVER] l COMBINE WITH GLUCOURINC ACID TO FORM THE CONJUGATED [ DIRECT ] BILIRUBIN [ WATER SOLUBLE ] l Van den Bergh reaction [DIRECT] Alcohol added after van den Gergh [INDIRECT]

HAEMOGLOBIN IRON FERRITIN TO BE REUSED +RBC WALL PROTEIN BILIRUBIN WATER INSOLUBLE GOES TO THE LIVER FOR CONGUGATION WITH GLUCOURINIC A. TO BECOME WATER SOLUBLE BLOOD URINE AMINOACIDS AMINOACID POOL

URINE IN OBSTRUCTIVE JAUNDICE TEA COLOUR

BILIRUBIN CYCLE
![DEEP JAUNDICE [OBSTRUCTIVE]](https://present5.com/presentation/79468405_187640252/image-13.jpg "DEEP JAUNDICE [OBSTRUCTIVE]")
DEEP JAUNDICE [OBSTRUCTIVE]
![S OF OBSTRUCTIVE JAUNDICE l l l l 1 -STONES 2 -STRICTURES; [BENIGN] 3](https://present5.com/presentation/79468405_187640252/image-14.jpg "S OF OBSTRUCTIVE JAUNDICE l l l l 1 -STONES 2 -STRICTURES; [BENIGN] 3")
S OF OBSTRUCTIVE JAUNDICE l l l l 1 -STONES 2 -STRICTURES; [BENIGN] 3 -CA. HEAD OF THE PANCREASE 4 -CHOLANGIOCARCINOMA 5 -PERIAMPULLARY TUMOUR 6 -PRESSURE FROM OUTSIDE; L. N. , M. SYN. 7 -CHOLEDOCHAL CYST 8 -PARASITES; FILLING THE LUMEN

CAUSES IN THE LUNEN ASCARIS CLONORCHIASIS PARASITES HYDATID PAPILLOMATOSIS CHOLANGIOCARCINOMA STONE IS THE COMMONEST

IN THE WALL: STRICTURES BENIGN STRICTURES MALIGNANT STRICTURES

OUTSIDE THE WALL L. N. Stone in cystic duct MIRIZZI SYND HARTMANN`S POUCH stone HEAD OF THE PANCREASE ANY MASS OUTSIDE

MIRRIZI`s syndrome
![BENIGN STRICTURES l l l 1 -BILIARY ATRESIA 2 -IATROGENIC BILIARY SURGERY[commonest] GASTRECTOMY HEPATIC](https://present5.com/presentation/79468405_187640252/image-19.jpg "BENIGN STRICTURES l l l 1 -BILIARY ATRESIA 2 -IATROGENIC BILIARY SURGERY[commonest] GASTRECTOMY HEPATIC")
BENIGN STRICTURES l l l 1 -BILIARY ATRESIA 2 -IATROGENIC BILIARY SURGERY[commonest] GASTRECTOMY HEPATIC RESECTION LIVER TRANSPLANT 3 -INFLAMMATORY; CHOLANGITIS , PANCREATITIS, SCLEROSINGCHOLANANGITIS. 4 -TRAUMA 5 -IDIOPATHIC 6 -RADIOTHERAPY

BILIARY ATRESIA NORMAL BILIARY ATRESIA

CAUSES

THE COMMONEST CAUSE l STONE SLIPPING INTO THE BILIARY TREE

IMPACTED STONE AT THE LOWER END OF C. B. D.

ASSENDING CHOLANGITIS WITH LIVER ABSESSES

CA. HEAD OF THE PANCREASE

ENDOSCOPIC VIEW OF PERIAMPULLARY TUMOUR ORIGIN 1 -DEUDENAL MUCOSA OR 2 -C. B. D. OR 3 -PANCREATIC DUCT

CHOLANGICARCINOMA

CHOLANGIOCARCINOMA LIVER METASTASIS

C. B. D. STRICTURE

SCLEROSING CHOLANGITIS • Associated with U. Colitis in 70% of cases • May lead to malignancy • Unknown aetiology • Symptoms of cholangitis • Treatment; Antibiotics • Or liver transplant Rosary beads ﺷﻜﻞ ﺍﻟﻤﺴﺒﺤﺔ

SYMPTOMS l l l l PAIN YELLOW DISCOLOURATION SKIN &M. M. DARK URINE [TEA COLOUR] CLAY COLOUR STOOL ﻟﻮﻥ ﺍﻟﻄﺤﻴﻨﻴﺔ ITCHING FEVER IF CHOLANGITIS SUPERVENE LOSS OF APPETITE LOSS OF WEIGHT IN MALIGNACY

SIGNS LOSS OF Wt. IN MALIGNANCY l TOXIC IN CHOLANGITIS, [CHARCOT`S TRIAD, ; PAIN, FEVER , JAUNDICE] l YELLOW DISCOLOURATION OF SKIN, M. M. l TROISIER`S SIGN. VIRCHOW`S NODE l TENDER R. U. Q. [IN CHOLANGITIS] l COURVOISIER` LAW[IN CA. HEAD OF PAN. ] l ABDOMINL MASS l ASCITES[IN MAIGNANCY] l
![DEEP JAUNDICE [GREEN] [OBSTRUCTIVE] l. VIRCHOW`S NODE OR [TROISIER`S SIGN] BRUISING VIT. K DEF.](https://present5.com/presentation/79468405_187640252/image-33.jpg "DEEP JAUNDICE [GREEN] [OBSTRUCTIVE] l. VIRCHOW`S NODE OR [TROISIER`S SIGN] BRUISING VIT. K DEF.")
DEEP JAUNDICE [GREEN] [OBSTRUCTIVE] l. VIRCHOW`S NODE OR [TROISIER`S SIGN] BRUISING VIT. K DEF. 2, 4, 7, 9, 10. DEPEND ON IT

COURVOISIER` LAW DISTENDED GALL BLADDER IN CA, HEAD OF PANCREASE

ASCITES IN ADVANCED CA. HEAD OF PANCREASE

INVESTIGATIONS l l l l C. B. C. DIFF. , ESR. L. FT. *S. ALK. P. * PROTHROMBIN TIME S. AMYLASE K. F. T. ELECTRLYTES URINE ANALSIS * BILIRUBIN * STOOL ANALYSIS, ; FAT, BLOOD.

INVESTIGATIONS l U. S. STONE
![DILATED CBD & STONE [US] Should be more than 6 mm](https://present5.com/presentation/79468405_187640252/image-38.jpg "DILATED CBD & STONE [US] Should be more than 6 mm")
DILATED CBD & STONE [US] Should be more than 6 mm

OUBLE BURRLE SIGN &DISTENDED G. PERIAMPULLARY TUMOUR

ERCP SPHINCTEROTOMY

STONE EXTRACTION BY BASKET

STONE EXTRACTION BY BALLON

ERCP C. B. D. STONE

C. B. D. BIG STONE

STENT

STONE REMOVED

C. B. D. STRICTURE

C. B. D. STENT WITH GOOD FLOW

CHOLANGICARCINOMA

CHOLANGIOCARCINOMA

E. R. C. P. FOR EXTRAHEPATIC CHOLANGIOCARCINOMA

ENDOSCOPIC VIEW OF PERIAMPULLARY TUMOUR

M. R. C. P

P. T. C. l PERCUTANOUS TRANSHEPATIC CHOLANGIOGRAM

PEROPERATIVE CHOLANGIOGRAM

T. TUBE CHOLANGIOGRAM

DRAIN CHOLANGIOGRAM

MANAGEMENT-1 l l CORRECTION OF THE DERENGED PARAMETRES ADMINISTRATION OF VITAMIN K ANTIBIOTICS MANNITOL PRE, INTRA and POSTOPERATIVELY TO PREVENT HEPATO-RENAL SHUTDOWN

MANAGEMENT-2 l l l 1. STONE-SPHINCTEROTOMY 2. STONE-EXPLORATION OF C. B. D. 3. STRICTURE-RESECTION ANASTOMOSIS FOR SHORT STRICTURES 4. STRICTURE-STENT FOR SHORT AND LONG 5. CA. HEAD OF THE PANCREASE =EARLY-WHIPPLE`S OPERATION[PANCREATICO-DUODENECTOMY. =LATE-BYPASS SURGERY[CHOLECYSTOJUJENOSTOMY

STENT FOR Ca. head of pancrease

WHIPPLE`S OPERATION Pancreatico-duodenoctomy
JAUNDICE lecture.ppt