

ebee1d4fea448976868115063d493d6a.ppt
- Количество слайдов: 29
 NYC School Health Automated Student Health Record Oxiris Barbot, M. D. Medical Director December 6, 2006
NYC School Health Automated Student Health Record Oxiris Barbot, M. D. Medical Director December 6, 2006
 Mission Promote the physical, emotional, social and environmental health of the 1. 2 million public school children of New York City.
Mission Promote the physical, emotional, social and environmental health of the 1. 2 million public school children of New York City.
 Office of School Health Structure • Department of Health and Mental Hygiene – – HPDP Division ~800 nurses 54 doctors ~ 150 public health advisers • Department of Education – Office of Youth Development and School. Community Services – ~300 nurses – 5 Health Content Experts
Office of School Health Structure • Department of Health and Mental Hygiene – – HPDP Division ~800 nurses 54 doctors ~ 150 public health advisers • Department of Education – Office of Youth Development and School. Community Services – ~300 nurses – 5 Health Content Experts
 Program Responsibilities Health Services • Physician of Last Resort • Students with IEP and Section 504 Needs – Nursing, OT, PT • • New Entrant and Other Exams Vision and Hearing Screening Coordinate response to communicable diseases Immunization and other mandates compliance
Program Responsibilities Health Services • Physician of Last Resort • Students with IEP and Section 504 Needs – Nursing, OT, PT • • New Entrant and Other Exams Vision and Hearing Screening Coordinate response to communicable diseases Immunization and other mandates compliance

 ASHR Goals • Computerize student health-related data • Easily accessible, yet secure • Improve the way health related information is maintained, tracked and retrieved • For the purpose of providing medical services, tracking mandated activities and providing follow up on identified health needs (case management). • Supply real-time data to Syndromic Surveillance
ASHR Goals • Computerize student health-related data • Easily accessible, yet secure • Improve the way health related information is maintained, tracked and retrieved • For the purpose of providing medical services, tracking mandated activities and providing follow up on identified health needs (case management). • Supply real-time data to Syndromic Surveillance
 • Web-based ‘EHR’ • In house ASHR 1. 0") Automated Student Health Record (ASHR) • Web-based ‘EHR’ • In house ASHR 1. 0 development Spring 2003 • Limited pilot September 2003 • Complete roll out of 811 sites June 2006 • Phase in ASHR 2. 0 September 2006
Automated Student Health Record (ASHR) • Web-based ‘EHR’ • In house ASHR 1. 0 development Spring 2003 • Limited pilot September 2003 • Complete roll out of 811 sites June 2006 • Phase in ASHR 2. 0 September 2006
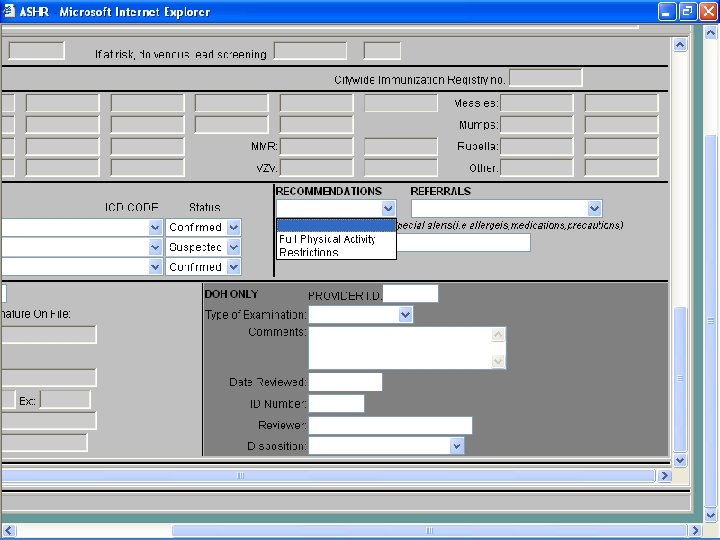
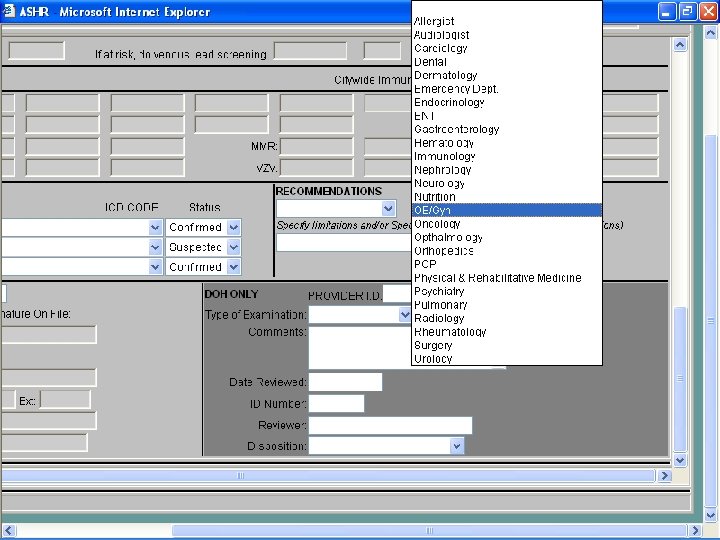
 • PMD & specialist contact info") ASHR Content • Student demographics (imported from DOE) • PMD & specialist contact info • Immunizations (imported from DOE) • Chronic Diagnoses • Allergies • Activities Restrictions • Vision and Hearing • Medication orders • Individual health plans • New Admission Exam • Asthma profile • Walk-in (exports to Syndromic Surveillance) • Diabetes module (under construction)
ASHR Content • Student demographics (imported from DOE) • PMD & specialist contact info • Immunizations (imported from DOE) • Chronic Diagnoses • Allergies • Activities Restrictions • Vision and Hearing • Medication orders • Individual health plans • New Admission Exam • Asthma profile • Walk-in (exports to Syndromic Surveillance) • Diabetes module (under construction)
 Use Case • State and City mandate that every newly entering student is required to submit a new admission examination (NAE aka 211 S)
Use Case • State and City mandate that every newly entering student is required to submit a new admission examination (NAE aka 211 S)
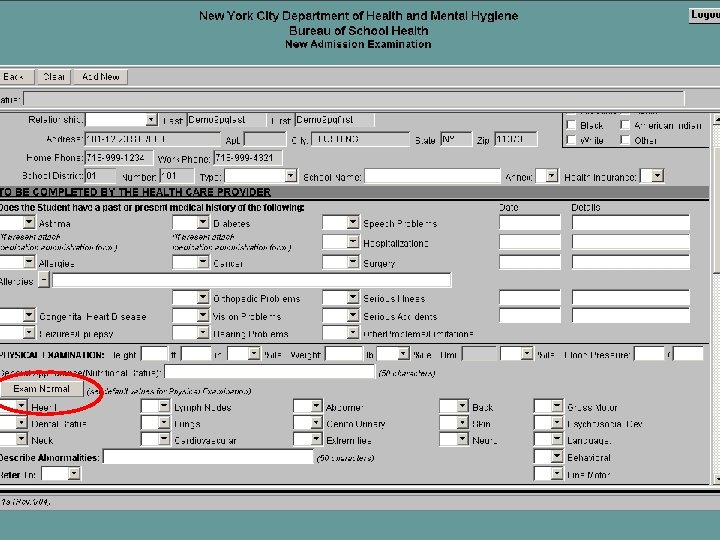
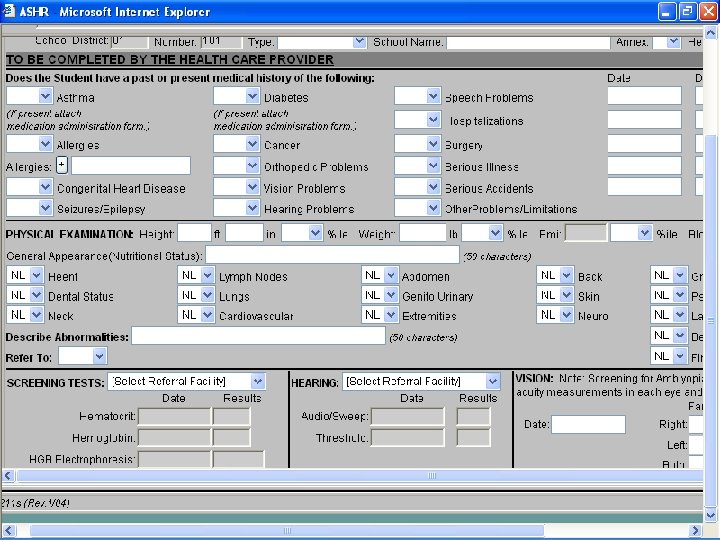
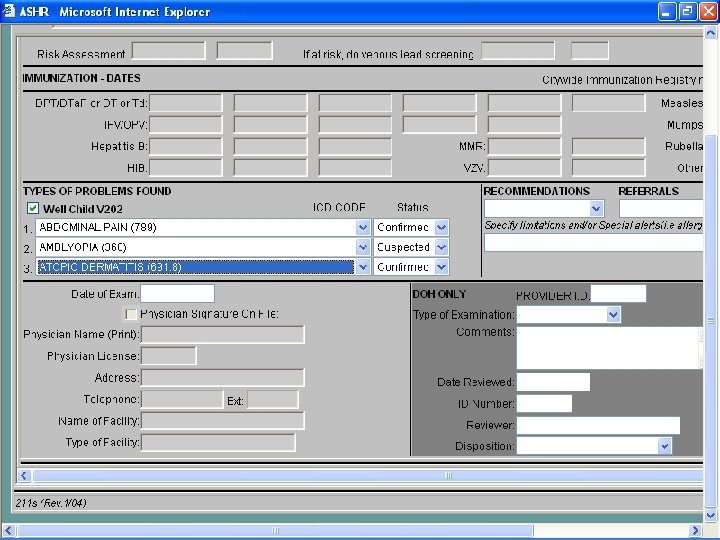
 • Form may change from year to year") New Admission Exam Form (211 S) • Form may change from year to year • Some fields are age dependant e. g. lead • Some fields are grade dependant e. g. TST • Some fields are historically poorly complied with e. g. complete vision screening to rule out amblyopia
New Admission Exam Form (211 S) • Form may change from year to year • Some fields are age dependant e. g. lead • Some fields are grade dependant e. g. TST • Some fields are historically poorly complied with e. g. complete vision screening to rule out amblyopia
 Current Work and Data Flow Model Child with parent visits provider Provider completes 211 S Patient Record Parent deliver 211 S to school 211 S Form School nurse enter 211 S data into ASHR 211 S Form Reports DOHMH maintains ASHR 211 S Form ASHR School DB EHR CHC EHRS Reports
Current Work and Data Flow Model Child with parent visits provider Provider completes 211 S Patient Record Parent deliver 211 S to school 211 S Form School nurse enter 211 S data into ASHR 211 S Form Reports DOHMH maintains ASHR 211 S Form ASHR School DB EHR CHC EHRS Reports
 Goal: Electronic Data Exchange EHR CHC-I EHRS EHR CHC-II EHRS EHR CHC-N EHRS School Forms 211 S Form Consent Form RES MUM Form Automated Student Health Record (ASHR) System School-I System School Forms School-II System School Forms School-N System
Goal: Electronic Data Exchange EHR CHC-I EHRS EHR CHC-II EHRS EHR CHC-N EHRS School Forms 211 S Form Consent Form RES MUM Form Automated Student Health Record (ASHR) System School-I System School Forms School-II System School Forms School-N System
 Benefits and Challenges: OSH • Benefits – Improve case management and initiation of related services – Increase number of students with mandated exams – Reduce paper that could potentially get lost – Reduce redundancy – Reallocate staff time to other school health activities • Challenges – – Identity management of outside providers “Wet signatures” “Communicating” with numerous EHRs Administering system for tracking consents
Benefits and Challenges: OSH • Benefits – Improve case management and initiation of related services – Increase number of students with mandated exams – Reduce paper that could potentially get lost – Reduce redundancy – Reallocate staff time to other school health activities • Challenges – – Identity management of outside providers “Wet signatures” “Communicating” with numerous EHRs Administering system for tracking consents
 Benefits and Challenges: Providers • Benefits – Improve care coordination with schools – Improve productivity • Time to complete forms • Redoing work already done • Challenges – Determining which diagnoses to transmit and which not to – “Keeping parents in the loop” – Administering consent system
Benefits and Challenges: Providers • Benefits – Improve care coordination with schools – Improve productivity • Time to complete forms • Redoing work already done • Challenges – Determining which diagnoses to transmit and which not to – “Keeping parents in the loop” – Administering consent system
 Benefits and Challenges: Parents • Benefits – Compliance with school requirements – Less missed school and work days – Improved care coordination between PCP and school system • Challenges – Knowing what is being transmitted to schools
Benefits and Challenges: Parents • Benefits – Compliance with school requirements – Less missed school and work days – Improved care coordination between PCP and school system • Challenges – Knowing what is being transmitted to schools
 Overall Goals for NAE Electronic Transmission • Traditional school health – ensure full participation in school activities – Students are free of communicable diseases – Students’ academic needs accommodated – Delivery of direct services • Public Health Oriented School Health – Population-based chronic disease management (chronic disease reporting) – Resource allocation – PH equivalent of clinical decision support
Overall Goals for NAE Electronic Transmission • Traditional school health – ensure full participation in school activities – Students are free of communicable diseases – Students’ academic needs accommodated – Delivery of direct services • Public Health Oriented School Health – Population-based chronic disease management (chronic disease reporting) – Resource allocation – PH equivalent of clinical decision support
 Benefits of Bi-directionality: Parents • Minimize unnecessary go-between activities • Updates on child’s status – e. g. # of visits to medical room • Reports on when and what type of information was transmitted
Benefits of Bi-directionality: Parents • Minimize unnecessary go-between activities • Updates on child’s status – e. g. # of visits to medical room • Reports on when and what type of information was transmitted
 Benefits of Bi-directionality: Provider • List of patients and schools they attend with nurse contact info – Medication services – Related services – e. g. PT/OT/ST – Accommodations – e. g. barrier-free schools • Updates on patient status – e. g. # of visits to medical room • Profile as compared to other providers
Benefits of Bi-directionality: Provider • List of patients and schools they attend with nurse contact info – Medication services – Related services – e. g. PT/OT/ST – Accommodations – e. g. barrier-free schools • Updates on patient status – e. g. # of visits to medical room • Profile as compared to other providers
 Benefits of Bi-directionality: OSH • Improve communications with providers • Expand from NAE to “doctor’s notes”
Benefits of Bi-directionality: OSH • Improve communications with providers • Expand from NAE to “doctor’s notes”
 Data transfer to Syndromic Surveillance • Began March 1, 2005 • Data fields transferred – – – Student Age ATS School DBN Official Class Complaint Description Record Last Update - Walk-In Time In - Grade Level - Zip - Comments • Process – Nightly Data transfer Service (DTS) of de-identified student walk-in data by school
Data transfer to Syndromic Surveillance • Began March 1, 2005 • Data fields transferred – – – Student Age ATS School DBN Official Class Complaint Description Record Last Update - Walk-In Time In - Grade Level - Zip - Comments • Process – Nightly Data transfer Service (DTS) of de-identified student walk-in data by school
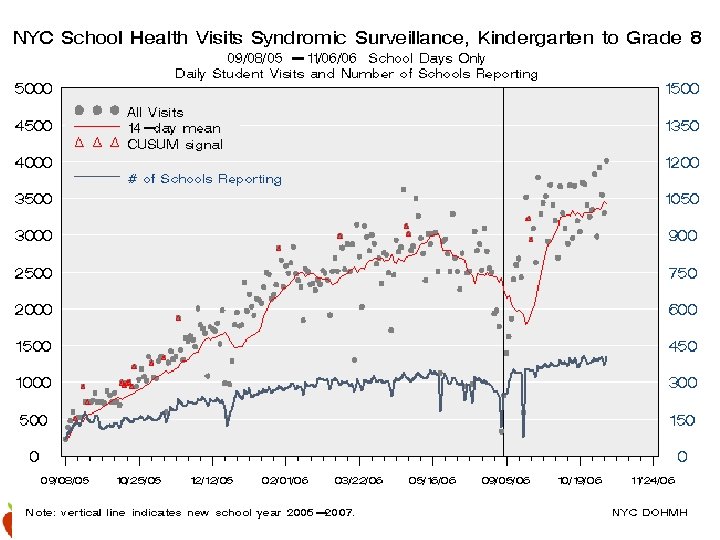
 Syndromic Surveillance Potential • Syndromes tracked – Allergy – Diarrhea – Injury – Rash - Asthma. Resp - Fever. Flu - Neuro - Vomiting • Once a week email now; daily once system fully functional • Potential for tracking to citywide, but too early to determine overall utility
Syndromic Surveillance Potential • Syndromes tracked – Allergy – Diarrhea – Injury – Rash - Asthma. Resp - Fever. Flu - Neuro - Vomiting • Once a week email now; daily once system fully functional • Potential for tracking to citywide, but too early to determine overall utility
 Flu signals correspond to city-wide signals
Flu signals correspond to city-wide signals