f98ec7a7447fddd5c50546f529b88eb3.ppt
- Количество слайдов: 32



Novel non-HLA antibodies and rejection Duska Dragun Nephrology, Charité Campus Mitte, Humboldt University Berlin

Antibody mediated acute rejection • The issue is not trivial, humoral rejection causes 30% of acute rejections and 10% of graft failures Pathogenesis • donor-specific antibodies against HLA class I and class antigens (C 4 d+) • „non-HLA“ antibodies against unknown targets

Subpopulation of patients with „unclear“ rejection • severe pathology: endarteritis or fibrinoid necrosis • 16/16 cases negative for HLA class I and class II DSA • no hereditary or autoimmune thrombophilia • negative serology for autoimmune disorders

Inferior survival in patients with non-HLA antibody rejection Dragun, D. et al. N Engl J Med 2005; 352: 558 -569

Demographic data HLA DSA- HLA DSA+ n 16 13 Living donor 7/16 5/13 Male 8/16 4/13 First kidney graft 7/16 5/13 Cold ischemia [h] 10. 3 (1. 6 – 13. 3) 13. 2 (1. 8 – 16. 2) HLA-mismatches 3 (0 – 5) 3 (2 – 6) Age at transplantation [years] 34. 8 (27. 9 -48. 4) 43. 6 (20. 1 -59. 8) Time transplantation to rejection [days] 4 (2 -1217) ( 9 (3 -680)

Clinical manifestations and biopsies HLA DSA- HLA DSA+ Severe hypertension 16/16 0/13 Histology: C 4 d positive 5/16 13/13

Our index case 50 -years old female recipient of the first, zero mismatch “full-house” kidney transplant with primary graft function (creatinine 1. 0 mg/dl at postoperative day 3) develops refractory vascular rejection with BP 240/160 mm Hg. Autoimmune serology is negative; CMV negative No hereditary thrombophilia. Why is this patient rejecting? Interesting detail from patients´medical history: „During my pregnancy, 25 years ago, I also had very high blood pressure and I almost lost my baby. “

J Clin Invest 103: 945 -952, 1999
 agonistic antibodies Patients´Ig. G")
Bioassay for Ang II Typ 1–Rezeptor (AT 1 R) agonistic antibodies Patients´Ig. G
 activity C 4 d+")
Bioassay results for Ang II type 1–receptor (AT 1 R) activity C 4 d+ HLA neg (before Tx) HLA neg (rejection) HLA pos (before Tx) HLA pos (rejection)

Ig. G activate Angiotensin II Type 1 Receptor Increase in BPM 30 20 10 0 Ang II AT 1 R-AA +Losartan +PD 123319

AT 1 R agonistic activity in transplant nephrectomies Increase in BPM 30 20 10 0 AT 1 R-AA Serum + Losartan AT 1 R-AA + Losartan Niere

Losartan + PPH improve graft survival in AT 1 R-AA+ patients Dragun, D. et al. N Engl J Med 2005; 352: 558 -569

Influence of losartan + PPH on AT 1 R activity Dragun, D. et al. N Engl J Med 2005; 352: 558 -569

AT 1 R Ig. G subclass activity Increase in beat number/min 30 20 10 0 Ig. G 1 Ig. G 2 Ig. G 3 Ig. G 4

Binding sites of AT 1 R activating Ig. G 1 and Ig. G 3 Ang II type 1 receptor Ingelfinger, J. R. N Engl J Med 2005; 352: 617 -619

Incidence of AT 1 R-AA positive rejection 279 kidney transplantations in 4. 5 years (Jan 1 st 2000 – July 31 st 2004) 119 rejection episodes in 83 patients 23 refractory to steroids (19. 3% of all rejections)

Incidence of AT 1 R-AA positive rejection 23 refractory to steroids (19. 3% of all rejections) 9 episodes HLA-DSA pos episodes 39. 1% of refract. rejections 10 episodes AT 1 R-AA pos episodes 43. 5% of refract. rejections 4 HLA-DSA neg/ AT 1 R-AA neg 7. 6% of all rejections 8. 4% of all rejections

Interdisciplinary „bedside to bench“ approach ECs, VSMCs

ERK ½ phosphorylation coronary endothelial cells coronary VSMC

NF-k. B
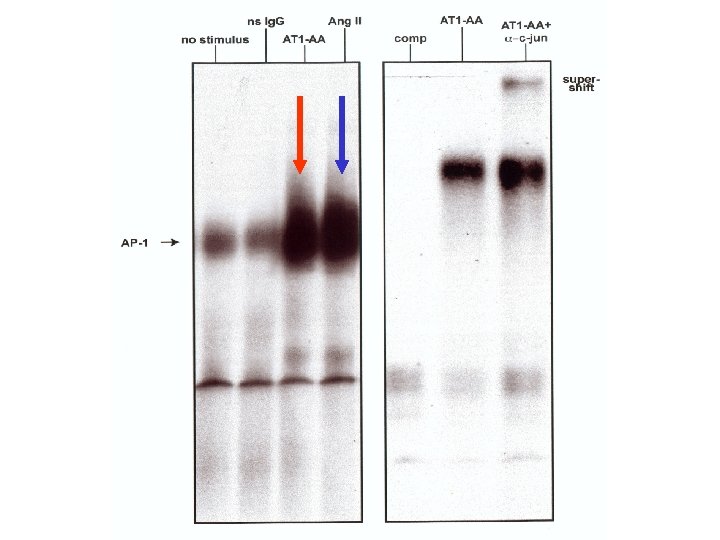

Cell promoter transfection experiments Tissue factor is a target of NF-k. B and AP-1 C 4 d+ AT 1 R-AA+ Mutant promoter

Tissue Factor expression in patients´ biopsies TF vor PPH + Losartan TF nach PPH + Losartan

Kochs´postulate study to investigate pathogenic role of AT 1 R-AA in transplant vascular pathology passive transfer of human Ig. G with AT 1 R agonistic activity

Orthotopic life-supporting functional NTx rat model Control Ig. G Lew recipient F 344 donor AT 1 -AA 7 d. pre NTx c telemetry device implant. 7 d. post NTx, osmotic mini-pump allograft morphology Telemetry follow-up

AT 1 R-AA induce vascular rejection AT 1 R-AA+ human Ig. G AT 1 R-AA- human Ig. G
 with AT 1 R human Ig.")
Colocalization of AT 1 R-AA (human Ig. G) with AT 1 R human Ig. G AT 1 R-AA+ human Ig. G AT 1 R-AA- human Ig. G

AT 1 R-AA induce hypertension Dragun, D. et al. N Engl J Med 2005; 352: 558 -569
 should")
Do AT 1 R-AA fulfill Koch´s postulates? 1. The agent (AT 1 -AA) should be present in all cases but not in controls 2. The agent (AT 1 -AA) must be isolated from the cases and studied in cells 3. The agent (AT 1 -AA) transferred into a healthy laboratory animal, should cause the disease 4. The agent should be re-isolated from the experimental disease

Putative mechanism of action of AT 1 R-AA Apoptosis? Mø CTL Permeability? AT 1 R-AA AT 1 R ECs AT 1 R MAPKs (Erk 1/2) AT 1 R-AA AT 1 R VSMCs AT 1 R MCP-1 TF AT 1 R-AA MAPKs (Erk 1/2) AT 1 R-AA AT 1 R TF RANTES NF-k. B, AP-1 Thrombotic Angiopathy! Effector cell infiltration!

AT 1 R-AA collaborators Max-Delbrück-Centre Berlin Gerd Wallukat Nephrology, Charité Campus Buch Ralf Dechend Dominik N. Müller Ralph Plehm Jan Hinrich Bräsen Friedrich C. Luft Pharmacology, Charité Campus Mitte Ulrich Kintscher Thomas Unger Nephrology, Charité Campus Mitte Diana Eckert Melina Nieminen-Kelhä Lutz Fritsche Klemens Budde Hans-H. Neumayer HLA Laboratory Charité Constanze Schönemann Pathology, Charité Campus Mitte Birgit Rudolph CNRS, Strasbourg Johan Hoebeke
f98ec7a7447fddd5c50546f529b88eb3.ppt