

c650a7d8a881a9ab8284c86831fd9e06.ppt
- Количество слайдов: 36
 Not always true… Dr Aisling Loy GUM SPR
Not always true… Dr Aisling Loy GUM SPR
 Presenting history • DY 39 year old female from Israel living in Ireland 20 yrs • Referred by GP Oct 12 with several day hx of painful mouth and genital ulcers • Hx of falling downstairs 1 week prior. • Multiple bruises from fall
Presenting history • DY 39 year old female from Israel living in Ireland 20 yrs • Referred by GP Oct 12 with several day hx of painful mouth and genital ulcers • Hx of falling downstairs 1 week prior. • Multiple bruises from fall
 History • Past Medical Hx of Hidradenitis suppurativa, recurrent oral apthous ulcers x 8 years • Fam Hx-
History • Past Medical Hx of Hidradenitis suppurativa, recurrent oral apthous ulcers x 8 years • Fam Hx-
 Hx Lives with partner 25 pkyr Hx Occasional C 2 H 5 OH No children • Father has Familial Mediterranean Fever and Ankylosing spondylitis • Aunt Behcets
Hx Lives with partner 25 pkyr Hx Occasional C 2 H 5 OH No children • Father has Familial Mediterranean Fever and Ankylosing spondylitis • Aunt Behcets
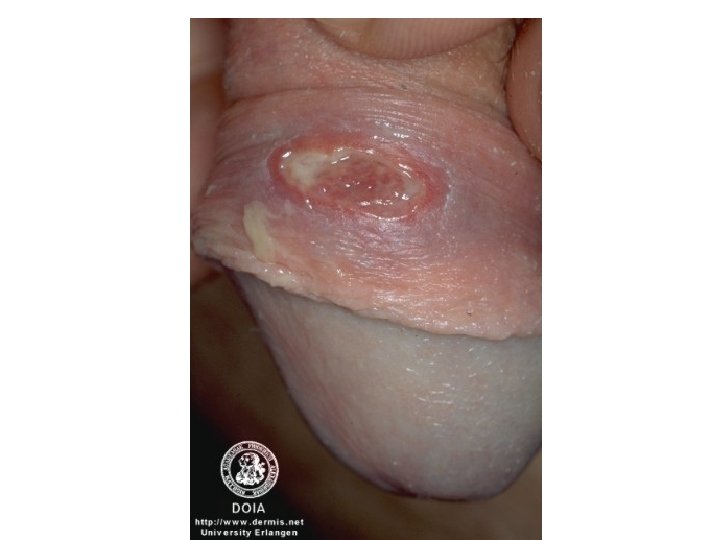
 Examination • • Normal vitals CVS/GIT/Resp/Neuro NAD Mouth- multiple ulcers, white coating GU- 2 x 2 cm ulcers on left labia majora. Indurated and tender.
Examination • • Normal vitals CVS/GIT/Resp/Neuro NAD Mouth- multiple ulcers, white coating GU- 2 x 2 cm ulcers on left labia majora. Indurated and tender.
 Laboratory • • • WCC 29. 3 Neut 25 Hb 15. 2 Plat 315 CRP 248 ESR 22 U/E NAD CXR NAD ECG NSR
Laboratory • • • WCC 29. 3 Neut 25 Hb 15. 2 Plat 315 CRP 248 ESR 22 U/E NAD CXR NAD ECG NSR
 Management plan • • Ulcer swabs taken IV Augmentin/ prophylactic clexane Tramadol/Tylex ANA/ANCA sent HIV serology HSV serology GUM and Derm consults
Management plan • • Ulcer swabs taken IV Augmentin/ prophylactic clexane Tramadol/Tylex ANA/ANCA sent HIV serology HSV serology GUM and Derm consults
 Progress • Reviewed by GUMTemp spike 38. 5 and continued to spike for next 2 days. • Blood cultures taken • STI screen • ? Behcets • Opthalmology review requested • Skin Bx taken from Vulva
Progress • Reviewed by GUMTemp spike 38. 5 and continued to spike for next 2 days. • Blood cultures taken • STI screen • ? Behcets • Opthalmology review requested • Skin Bx taken from Vulva
 Treatment • • Commenced Dermovate Topical Beclamethasone Oral Valtrex ? HSV Fluconazole
Treatment • • Commenced Dermovate Topical Beclamethasone Oral Valtrex ? HSV Fluconazole
 Skin Bx result • Skin Bx- dermal inflammation comprising of lymphocytes, histocytes and polymorphs. There are ectatic vascular spaces.
Skin Bx result • Skin Bx- dermal inflammation comprising of lymphocytes, histocytes and polymorphs. There are ectatic vascular spaces.
 Results • • Xray of SI joints NAD ANA neg ANCA neg CRP continued to improve STI screen neg HSV culture neg Hep B/C EBV Neg
Results • • Xray of SI joints NAD ANA neg ANCA neg CRP continued to improve STI screen neg HSV culture neg Hep B/C EBV Neg
 Progress • • Discharged home after 2 weeks Completed 7 days of IV/PO Augmentin CRP reduced Poor initial response to topical dermovate Changed to Colchicine 1 mg BD for 2 weeks Followed up in OPD Acute inflammation of the apocrine glands Special stains for Herpes virus, fugi, Mycobacteria and bacteris are negative.
Progress • • Discharged home after 2 weeks Completed 7 days of IV/PO Augmentin CRP reduced Poor initial response to topical dermovate Changed to Colchicine 1 mg BD for 2 weeks Followed up in OPD Acute inflammation of the apocrine glands Special stains for Herpes virus, fugi, Mycobacteria and bacteris are negative.
 2 weeks later in OPD • Sig response to colchicine, not completely healed • Returned to Isreal reviewed by Behcet specialist • Continued on 1. 5 mgs OD • For Exacerbation prednisolone 20 mgs • HLAB 51 neg
2 weeks later in OPD • Sig response to colchicine, not completely healed • Returned to Isreal reviewed by Behcet specialist • Continued on 1. 5 mgs OD • For Exacerbation prednisolone 20 mgs • HLAB 51 neg
 Dx with Behcets • What is Behcets? • Why did she develop Behcets now? • Is there a link to her family hx and her own medical Hx? • What will the future hold?
Dx with Behcets • What is Behcets? • Why did she develop Behcets now? • Is there a link to her family hx and her own medical Hx? • What will the future hold?
 • Turkish Physician • In 1937,") Hx of Behcets • Hulusi Behcet (18891948 ) • Turkish Physician • In 1937, described the classic trisymptom complex of hypopyon, iritis, and orogenital aphthosis
Hx of Behcets • Hulusi Behcet (18891948 ) • Turkish Physician • In 1937, described the classic trisymptom complex of hypopyon, iritis, and orogenital aphthosis
 • Endemic disease in") 2500 yrs ago • Hippocrates of Kos (460 -377 BC) • Endemic disease in Asia Minor characterised by “aphthous ulcerations, defluxions about the genital parts, watery ophthalmies of a chronic character. . . which destroyed the sight of many persons, large herpetic lesions. ”
2500 yrs ago • Hippocrates of Kos (460 -377 BC) • Endemic disease in Asia Minor characterised by “aphthous ulcerations, defluxions about the genital parts, watery ophthalmies of a chronic character. . . which destroyed the sight of many persons, large herpetic lesions. ”
 Spectrum of organ involvement in Behçet’s disease. Verity D H et al. Br J Ophthalmol 2003; 87: 1175 -1183 © 2003 by BMJ Publishing Group Ltd.
Spectrum of organ involvement in Behçet’s disease. Verity D H et al. Br J Ophthalmol 2003; 87: 1175 -1183 © 2003 by BMJ Publishing Group Ltd.
 Laboratory • Mild anemia and leukocytosis • The ESR, C-reactive protein may be raised. • Serum immunoglobulin levels, especially immunoglobulin A, may be elevated. • Circulating immune complexes.
Laboratory • Mild anemia and leukocytosis • The ESR, C-reactive protein may be raised. • Serum immunoglobulin levels, especially immunoglobulin A, may be elevated. • Circulating immune complexes.
 • Rheumatoid factor and antinuclear antibodies are absent.
• Rheumatoid factor and antinuclear antibodies are absent.
 Cutaneous manifestations
Cutaneous manifestations
 Joint manifestations • 50% develop signs or symptoms of synovitis, arthritis, and/or arthralgia. • The most frequent minor feature in childhoodonset BD. • Multiple-joint involvement is common.
Joint manifestations • 50% develop signs or symptoms of synovitis, arthritis, and/or arthralgia. • The most frequent minor feature in childhoodonset BD. • Multiple-joint involvement is common.
 Vascular involvement • This occurs in 7 -29% of patients, mostly men. • The 4 types of vascular lesions arterial occlusions, venous occlusions, aneurysms, and varices. • Arterial complications account for 7% of cases.
Vascular involvement • This occurs in 7 -29% of patients, mostly men. • The 4 types of vascular lesions arterial occlusions, venous occlusions, aneurysms, and varices. • Arterial complications account for 7% of cases.
 Gastrointestinal involvement • • 10% of patients with BD. Anorexia, vomiting, dyspepsia, diarrhoea, abdominal distention, abdominal pain
Gastrointestinal involvement • • 10% of patients with BD. Anorexia, vomiting, dyspepsia, diarrhoea, abdominal distention, abdominal pain
 • Neurologic involvement may present") Neurologic manifestations • Varies from 3. 2 -49%. (rare) • Neurologic involvement may present in various combinations. • Most serious complications, high fatality rate. • Occur within 5 years of disease onset • Severe headache is the most frequent.
Neurologic manifestations • Varies from 3. 2 -49%. (rare) • Neurologic involvement may present in various combinations. • Most serious complications, high fatality rate. • Occur within 5 years of disease onset • Severe headache is the most frequent.
 Behçet’s disease is associated with multiple hereditory and environmental risk factors. Verity D H et al. Br J Ophthalmol 2003; 87: 1175 -1183 © 2003 by BMJ Publishing Group Ltd.
Behçet’s disease is associated with multiple hereditory and environmental risk factors. Verity D H et al. Br J Ophthalmol 2003; 87: 1175 -1183 © 2003 by BMJ Publishing Group Ltd.
 Genetics • HLA-B 51 • Associated with Factor V Leiden deficiency • Displays genetic anticipation • More common in Isreal Arabs than Jews.
Genetics • HLA-B 51 • Associated with Factor V Leiden deficiency • Displays genetic anticipation • More common in Isreal Arabs than Jews.
 Immunological Abnormalities • Neutrophil infiltration, endothelial cell swelling, fibrinoid necrosis. • Increased levels of neutrophil priming cytokines, TNF, IL 1 B, IL 8, myeloperoxidase levels • ? genetic v primining agent v both
Immunological Abnormalities • Neutrophil infiltration, endothelial cell swelling, fibrinoid necrosis. • Increased levels of neutrophil priming cytokines, TNF, IL 1 B, IL 8, myeloperoxidase levels • ? genetic v primining agent v both
 ? Infective aetiology • Silk road promoted the spread of infection eg the black death, the plague of Athens. Behcet suspected an infectious aetiology • Monocytes show hypersensitivity to Streptococccal sanguis antigen • Higher levels of HSV 1 antibodies
? Infective aetiology • Silk road promoted the spread of infection eg the black death, the plague of Athens. Behcet suspected an infectious aetiology • Monocytes show hypersensitivity to Streptococccal sanguis antigen • Higher levels of HSV 1 antibodies
 Behçet’s disease. Verity D H et al. Br J Ophthalmol 2003; 87: 1175 -1183 © 2003 by BMJ Publishing Group Ltd.
Behçet’s disease. Verity D H et al. Br J Ophthalmol 2003; 87: 1175 -1183 © 2003 by BMJ Publishing Group Ltd.
 • 4 mutations") Link to Familial Mediterranean Fever • Gene ass’d with FMF (MEFV) • 4 mutations ass’d with Behcets • Gene codes for pyrin thought to regulate neutrophils • Similar ethnic distribution and effect on neutrophils • Thought these two are linked to same gene. • Thought to be a link with hidradenitis suppurativa
Link to Familial Mediterranean Fever • Gene ass’d with FMF (MEFV) • 4 mutations ass’d with Behcets • Gene codes for pyrin thought to regulate neutrophils • Similar ethnic distribution and effect on neutrophils • Thought these two are linked to same gene. • Thought to be a link with hidradenitis suppurativa
 Conventional Treatment
Conventional Treatment
 SYSTEMIC RX Azathiopine Interferon alpha Cyclophosphamide Cyclosporin Infliximab Etanercept Adalimumab Rituximab Anticoagulants
SYSTEMIC RX Azathiopine Interferon alpha Cyclophosphamide Cyclosporin Infliximab Etanercept Adalimumab Rituximab Anticoagulants
 Novel Treatments • • • Probiotic yoghurt Topical Tacrolimus Sublingual interferon alpha Zinc sulphate mouth wash Nigella sativa oil
Novel Treatments • • • Probiotic yoghurt Topical Tacrolimus Sublingual interferon alpha Zinc sulphate mouth wash Nigella sativa oil
 Why now? • Genetically primed plus a stress on the body starting a cytokine/neutrophilic/lymphocytic/ hyper response leading to a pathological systemic vasculitic phenonomen
Why now? • Genetically primed plus a stress on the body starting a cytokine/neutrophilic/lymphocytic/ hyper response leading to a pathological systemic vasculitic phenonomen
 Summary • Multisystem • Complex aeitology, both genetic and environmental • Varying prognosis • No specific diagnostic test • Treated with different methods of immune modulation.
Summary • Multisystem • Complex aeitology, both genetic and environmental • Varying prognosis • No specific diagnostic test • Treated with different methods of immune modulation.