

43831c50f837572f4bd8a0633c447069.ppt
- Количество слайдов: 71
: Our Experience at a Tertiary Care Center Brennen Bittel, DO") Non-Convulsive Status Epilepticus (NCSE): Our Experience at a Tertiary Care Center Brennen Bittel, DO Clinical Neurophysiology Fellow
Non-Convulsive Status Epilepticus (NCSE): Our Experience at a Tertiary Care Center Brennen Bittel, DO Clinical Neurophysiology Fellow
 Overview n Background information: q q q Epidemiology Clinical features Electrographic definition n q q q EDX pitfalls Treatment Pathology Outcomes n KU Data q 2009 -2013
Overview n Background information: q q q Epidemiology Clinical features Electrographic definition n q q q EDX pitfalls Treatment Pathology Outcomes n KU Data q 2009 -2013
 Incidence/prevalence n n SE* in emergency room or intensive care units ~ 150, 000/yr NCSE: q q n n n 25 % of all SE 1. 5 – 60/100, 000/yr 34% of all SE in a tertiary care center 27% of ICU pts w/ altered mental status 8% of pts in coma Celesia 1976, Tomson 1992, Drislane 2000, Towne 2000
Incidence/prevalence n n SE* in emergency room or intensive care units ~ 150, 000/yr NCSE: q q n n n 25 % of all SE 1. 5 – 60/100, 000/yr 34% of all SE in a tertiary care center 27% of ICU pts w/ altered mental status 8% of pts in coma Celesia 1976, Tomson 1992, Drislane 2000, Towne 2000
 3.") Definition 1. Diminished level of consciousness, confusion 2. Epileptiform EEG (continuous or discrete) 3. Response to treatment? ?
Definition 1. Diminished level of consciousness, confusion 2. Epileptiform EEG (continuous or discrete) 3. Response to treatment? ?
 1. Change in mental status- Semiology n Ambulatory confused patients, mildly confused hospitalized patients n Lethargic and comatose patients in intensive care units
1. Change in mental status- Semiology n Ambulatory confused patients, mildly confused hospitalized patients n Lethargic and comatose patients in intensive care units
 Diminished Level of Consciousness, Confusion
Diminished Level of Consciousness, Confusion
 Clinical presentations
Clinical presentations
 CPSE (complex partial SE) Intermittent Continuous 20 -40% Krumholz 1999,") NCSE ASE (absence SE) CPSE (complex partial SE) Intermittent Continuous 20 -40% Krumholz 1999, Meierkord 2007 ESE (electrographic SE) 35 -40% SPSE (Simple partial SE)
NCSE ASE (absence SE) CPSE (complex partial SE) Intermittent Continuous 20 -40% Krumholz 1999, Meierkord 2007 ESE (electrographic SE) 35 -40% SPSE (Simple partial SE)
 Continuous • • • ESE (electrographic SE) CPSE (complex partial") NCSE ASE (absence SE) Continuous • • • ESE (electrographic SE) CPSE (complex partial SE) Confused Bizarre behavior Fluctuations +/- automatisms Aphasia Intermittent n n Stuporous Comatose GTC at onset Medical illness SPSE (Simple partial SE)
NCSE ASE (absence SE) Continuous • • • ESE (electrographic SE) CPSE (complex partial SE) Confused Bizarre behavior Fluctuations +/- automatisms Aphasia Intermittent n n Stuporous Comatose GTC at onset Medical illness SPSE (Simple partial SE)
 Other sxs/signs n n n n n Agitation Lethargy Mutism Disruptive behavior Staring Laughter Crying Rigidity Perseveration n n Subtle motor movements Hallucinations
Other sxs/signs n n n n n Agitation Lethargy Mutism Disruptive behavior Staring Laughter Crying Rigidity Perseveration n n Subtle motor movements Hallucinations
 DDx n n n Metabolic/toxic encephalopathy Complicated migraine/aura Prolonged post-ictal state Psychiatric disorders Substance abuse/withdrawal/intoxication q n n DTs TIA Transient global amnesia
DDx n n n Metabolic/toxic encephalopathy Complicated migraine/aura Prolonged post-ictal state Psychiatric disorders Substance abuse/withdrawal/intoxication q n n DTs TIA Transient global amnesia
 Husain 2003 n 12 in the NCSE group and 36 in the non. NCSE group q q 100% sensitivity Ocular movements n q Rhythmic blinking, deviation, nystagmus, rhythmic hippus Recent or remote risk factor for seizure n Previous stroke, tumor, previous neurosurgery, dementia, epilepsy, and meningitis
Husain 2003 n 12 in the NCSE group and 36 in the non. NCSE group q q 100% sensitivity Ocular movements n q Rhythmic blinking, deviation, nystagmus, rhythmic hippus Recent or remote risk factor for seizure n Previous stroke, tumor, previous neurosurgery, dementia, epilepsy, and meningitis
 Epileptiform EEG
Epileptiform EEG
 2. Epileptiform EEG n n Frequency Morphology Evolution Rhythmicity
2. Epileptiform EEG n n Frequency Morphology Evolution Rhythmicity
 Treiman criteria- GCSE Five characteristic stages: 1. 2. 3. 4. Discrete seizures Merging seizures Continuous seizures with brief "flat" periods on the EEG -- (usually no convulsions) 5. Prolonged flat periods with periodic discharges -- (usually no convulsions)
Treiman criteria- GCSE Five characteristic stages: 1. 2. 3. 4. Discrete seizures Merging seizures Continuous seizures with brief "flat" periods on the EEG -- (usually no convulsions) 5. Prolonged flat periods with periodic discharges -- (usually no convulsions)
 Young 1996 - NCSE n Primary Criteria 1. 2. 3. Repetitive generalized or focal spikes, sharp waves, spike-wave or sharp-slow wave complexes at >3/sec AND #4 Sequential rhythmic waves and 1 -3, +/- 4 n Secondary Criteria 1. 2. 3. 4. Incrementing onset: voltage or slowing Decrementing offset: voltage or frequency Post-discharge slowing or voltage attenuation Significant improvement in clinical state or baseline EEG after AED***
Young 1996 - NCSE n Primary Criteria 1. 2. 3. Repetitive generalized or focal spikes, sharp waves, spike-wave or sharp-slow wave complexes at >3/sec AND #4 Sequential rhythmic waves and 1 -3, +/- 4 n Secondary Criteria 1. 2. 3. 4. Incrementing onset: voltage or slowing Decrementing offset: voltage or frequency Post-discharge slowing or voltage attenuation Significant improvement in clinical state or baseline EEG after AED***
 Walker 2005 1. Frequent/continuous focal electrographic szs, with ictal patterns that wax and wane with change in amplitude, frequency, and/or spatial distribution. 2. Frequent/continuous generalized spike-wave discharges in pts without a previous history of epileptic encephalopathy or epilepsy syndrome. 3. Frequent/continuous generalized spike-wave discharges, which showed significant changes in intensity or frequency (usually a faster frequency) when compared to baseline EEG, in patients with an epileptic encephalopathy or epilepsy syndrome 4. PLEDs/ BIPEDs in patients in coma in the aftermath of a generalized tonic– clonic status epilepticus (subtle status epilepticus). 5. EEG patterns that were less easy to interpret included: Frequent/continuous EEG abnormalities (spikes, sharp-waves, rhythmic slow activity, PLEDs, BIPEDs, GPEDs, triphasic waves) in patients whose EEGs showed no previous similar abnormalities, in the context of acute cerebral damage (e. g. , anoxic brain damage, infection, trauma). 6. Frequent/continuous generalized EEG abnormalities in pts w/ epileptic encephalopathies in whom similar interictal EEG patterns were seen, but in whom clinical symptoms were suggestive of NCSE.
Walker 2005 1. Frequent/continuous focal electrographic szs, with ictal patterns that wax and wane with change in amplitude, frequency, and/or spatial distribution. 2. Frequent/continuous generalized spike-wave discharges in pts without a previous history of epileptic encephalopathy or epilepsy syndrome. 3. Frequent/continuous generalized spike-wave discharges, which showed significant changes in intensity or frequency (usually a faster frequency) when compared to baseline EEG, in patients with an epileptic encephalopathy or epilepsy syndrome 4. PLEDs/ BIPEDs in patients in coma in the aftermath of a generalized tonic– clonic status epilepticus (subtle status epilepticus). 5. EEG patterns that were less easy to interpret included: Frequent/continuous EEG abnormalities (spikes, sharp-waves, rhythmic slow activity, PLEDs, BIPEDs, GPEDs, triphasic waves) in patients whose EEGs showed no previous similar abnormalities, in the context of acute cerebral damage (e. g. , anoxic brain damage, infection, trauma). 6. Frequent/continuous generalized EEG abnormalities in pts w/ epileptic encephalopathies in whom similar interictal EEG patterns were seen, but in whom clinical symptoms were suggestive of NCSE.
 EEG Diagnosis n Inevitably subjective
EEG Diagnosis n Inevitably subjective
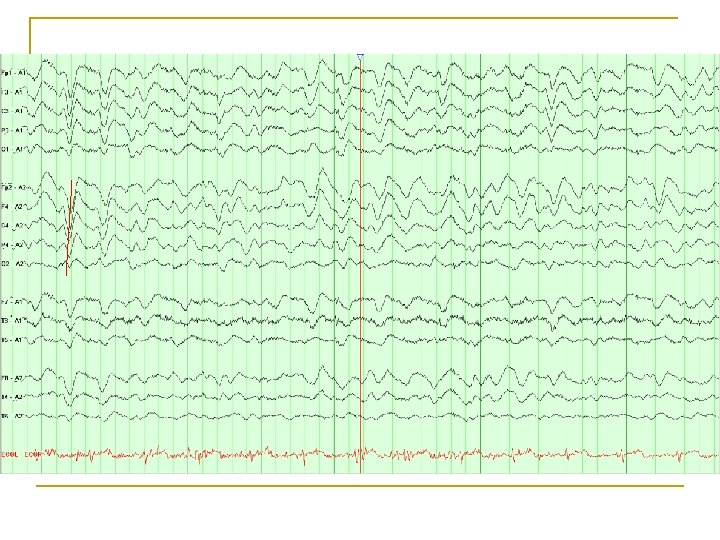
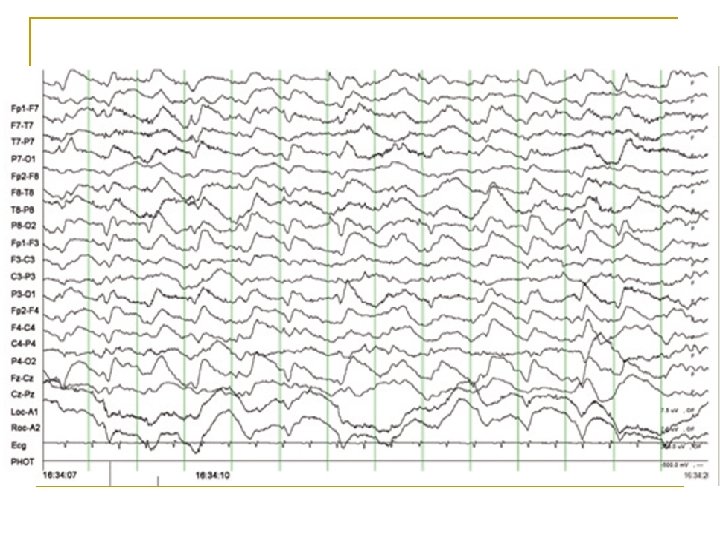
 Which tracing shows NCSE?
Which tracing shows NCSE?
 PLEDS
PLEDS
 Triphasic waves
Triphasic waves
 GPEDS
GPEDS
 L Temp/parietal CPSE
L Temp/parietal CPSE
 Diagnostic pitfalls n n PLEDs, Bi. PLEDs, GPEDs, SIRPIDs Encephalopathy Status myoclonus CJD
Diagnostic pitfalls n n PLEDs, Bi. PLEDs, GPEDs, SIRPIDs Encephalopathy Status myoclonus CJD
 PLEDs n No absolute frequency criterion can be used to distinguish PLEDs from seizures n Frequency q q n Acute, serious neurologic illness q n 1 - 4 seconds (short periodicity) >4 seconds (long periodicity) Mortality is high—up to 50% within 2 months Walsh 1987
PLEDs n No absolute frequency criterion can be used to distinguish PLEDs from seizures n Frequency q q n Acute, serious neurologic illness q n 1 - 4 seconds (short periodicity) >4 seconds (long periodicity) Mortality is high—up to 50% within 2 months Walsh 1987
 PLEDs n Associated with: • • • Stroke (the most common cause in many reports) Tumors Infections- Viral (acute and chronic) Metabolic disturbances Head injury SDH Anoxia Brain abscess Congenital lesions Tuberous sclerosis Multiple sclerosis Creutzfeld–Jakob disease
PLEDs n Associated with: • • • Stroke (the most common cause in many reports) Tumors Infections- Viral (acute and chronic) Metabolic disturbances Head injury SDH Anoxia Brain abscess Congenital lesions Tuberous sclerosis Multiple sclerosis Creutzfeld–Jakob disease
 PLEDs n 80 -90% of pts had recent clinical seizures q n 66% had some form of SE Risk for more seizures q Half patients without prior epilepsy developed subsequent epilepsy n Most PLEDs will resolve after days to weeks n Part of an ictal-interictal spectrum n Snodgrass 1989, Kaplan 2007, Chong 2005, Walsh 1987
PLEDs n 80 -90% of pts had recent clinical seizures q n 66% had some form of SE Risk for more seizures q Half patients without prior epilepsy developed subsequent epilepsy n Most PLEDs will resolve after days to weeks n Part of an ictal-interictal spectrum n Snodgrass 1989, Kaplan 2007, Chong 2005, Walsh 1987
 PLEDs
PLEDs
 PLEDs regression- 1 week later
PLEDs regression- 1 week later
 Triphasic waves n Seen commonly in metabolic encephalopathies q n n Bursts 1 -2 Hz q q n not seen in NCSE Increased with stimulation q n Blunted, low-moderate amplitude Dominant positive second phase, slow rise Phase lag q n Classically in renal or hepatic failure not seen in NCSE Sometimes suppressed with BZDs (40 -60%) q Kaplan 2006
Triphasic waves n Seen commonly in metabolic encephalopathies q n n Bursts 1 -2 Hz q q n not seen in NCSE Increased with stimulation q n Blunted, low-moderate amplitude Dominant positive second phase, slow rise Phase lag q n Classically in renal or hepatic failure not seen in NCSE Sometimes suppressed with BZDs (40 -60%) q Kaplan 2006
 Encephalopathies w/Epileptic Features n Reversible q q Usually no hx of epilepsy Medication related n n n n Irreversible q q Post-anoxic Creutzfeld-Jacob BZD withdrawal Cephalosporin Abx Ifosfamide Baclofen Psychotropics Rhythmic, semirhythmic delta Drislane 2000 n Importance of c-VEEG q Look for subtle clinical changes a/w rhythmicity
Encephalopathies w/Epileptic Features n Reversible q q Usually no hx of epilepsy Medication related n n n n Irreversible q q Post-anoxic Creutzfeld-Jacob BZD withdrawal Cephalosporin Abx Ifosfamide Baclofen Psychotropics Rhythmic, semirhythmic delta Drislane 2000 n Importance of c-VEEG q Look for subtle clinical changes a/w rhythmicity
 CJD – EEG progression
CJD – EEG progression
 Patients at risk 1. Following seizures or GCSE -- Up to 50% in NCSE after convulsions cease 2. 3. 4. 5. AMS with subtle motor signs AMS in epileptic w/ acute medical illness Post-stroke pt faring worse or recovery halted Elderly pt with AMS (post BZD withdrawal) De. Lorenzo 1998, Drislane 2000
Patients at risk 1. Following seizures or GCSE -- Up to 50% in NCSE after convulsions cease 2. 3. 4. 5. AMS with subtle motor signs AMS in epileptic w/ acute medical illness Post-stroke pt faring worse or recovery halted Elderly pt with AMS (post BZD withdrawal) De. Lorenzo 1998, Drislane 2000
 Risk factors n Mental status changes q q q q ICH SAH Large vessel CVA Meningoencephalitis CHI/TBI Tumor Post-surgical Drislane 2000
Risk factors n Mental status changes q q q q ICH SAH Large vessel CVA Meningoencephalitis CHI/TBI Tumor Post-surgical Drislane 2000
 3. Treatment Response n Treatment response less often considered diagnostic q Clinical response may be delayed hours to days q Shneker 2003
3. Treatment Response n Treatment response less often considered diagnostic q Clinical response may be delayed hours to days q Shneker 2003
 Treatment n CPSE q q q n BZDs IV AEDs Usually recurs ESE q q q 60% respond to initial BZD (clinical delay) 15% resistant to BZD Require IV AEDs n +/- Anesthesia n Granner 1994, Shneker 2003
Treatment n CPSE q q q n BZDs IV AEDs Usually recurs ESE q q q 60% respond to initial BZD (clinical delay) 15% resistant to BZD Require IV AEDs n +/- Anesthesia n Granner 1994, Shneker 2003
 Anesthesia- Claassen 2002 n 193 pts w/ refractory SE q Tx with midazolam vs propofol vs pentobarbitol n Midazolam q q n Pentobarbitol q q n n Increased breakthrough seizures Less hypotension Lowest treatment failure/recurrence More hypotension Refractory NCSE- more common with propofol and midazolam No standardized treatment regimen for use of anesthesia in SE
Anesthesia- Claassen 2002 n 193 pts w/ refractory SE q Tx with midazolam vs propofol vs pentobarbitol n Midazolam q q n Pentobarbitol q q n n Increased breakthrough seizures Less hypotension Lowest treatment failure/recurrence More hypotension Refractory NCSE- more common with propofol and midazolam No standardized treatment regimen for use of anesthesia in SE
 Anesthesia n No consensus on NCSE q More harm than good? n n n q Hypotension Sepsis/line infection DVT Ultimate effect on brain? n Outcomes…
Anesthesia n No consensus on NCSE q More harm than good? n n n q Hypotension Sepsis/line infection DVT Ultimate effect on brain? n Outcomes…
 Pathologic changes n Animal models q q q Induced GCSE, up to 5 hours, in baboons Hippocampal volume loss n ↑ with frequent, prolonged seizures n ↓ if paralytic used to abolish convulsions q Hyperpyrexia, hypotension, hypoxia, acidosis, and hypoglycemia Changes in high-frequency (10 Hz) vs low frequency (1 Hz) discharges n Bertram 1990
Pathologic changes n Animal models q q q Induced GCSE, up to 5 hours, in baboons Hippocampal volume loss n ↑ with frequent, prolonged seizures n ↓ if paralytic used to abolish convulsions q Hyperpyrexia, hypotension, hypoxia, acidosis, and hypoglycemia Changes in high-frequency (10 Hz) vs low frequency (1 Hz) discharges n Bertram 1990
 Pathologic changes n Human autopsy studies q q GCSE > epilepsy w/o SE > normal Synergistic damage n Increase in excitatory neurotransmitters Metabolic changes (lactate, pyruvate) n Earnest 1992, Kruhmholz 1995 n
Pathologic changes n Human autopsy studies q q GCSE > epilepsy w/o SE > normal Synergistic damage n Increase in excitatory neurotransmitters Metabolic changes (lactate, pyruvate) n Earnest 1992, Kruhmholz 1995 n
 Outcomes: Mortality n Vary highly based on the underlying etiology of the condition q q q n Brain tumors (30 -40%) Acute stroke (35%) Epilepsy (3%) Duration of seizures q 43 ICU pts in NCSE on VEEG n n <10 h = death in 10% >20 h = death in 85% n Age > 60 y n Rarely fatal in isolation q Young 1996, Meierkord 2007, Towne 1994
Outcomes: Mortality n Vary highly based on the underlying etiology of the condition q q q n Brain tumors (30 -40%) Acute stroke (35%) Epilepsy (3%) Duration of seizures q 43 ICU pts in NCSE on VEEG n n <10 h = death in 10% >20 h = death in 85% n Age > 60 y n Rarely fatal in isolation q Young 1996, Meierkord 2007, Towne 1994
 Outcomes: Morbidity n CPSE q No difference between continuous and intermittent electrographic sz activity n n n Return to baseline cognitive status (n=20) Cognitive decline, memory issues (n=10) ESE q q Determined by primary etiology Tend to have poorer prognosis n Drislane 1999, Cockerell 1994, Krumholz 1995
Outcomes: Morbidity n CPSE q No difference between continuous and intermittent electrographic sz activity n n n Return to baseline cognitive status (n=20) Cognitive decline, memory issues (n=10) ESE q q Determined by primary etiology Tend to have poorer prognosis n Drislane 1999, Cockerell 1994, Krumholz 1995
 Outcomes: MICU vs NICU n 168 visits over 3 yrs q 27% NICU n n n More pts w/ stroke More CPSE Avg age: 59 Alert/somnolent pts Fewer pts intubated, more tracheostomized Varelas 2013 q 73% MICU n n n More toxic/metabolic enceph More GCSE Avg age: 51 Obtunded/comatose pts Higher APACHE 2 scores
Outcomes: MICU vs NICU n 168 visits over 3 yrs q 27% NICU n n n More pts w/ stroke More CPSE Avg age: 59 Alert/somnolent pts Fewer pts intubated, more tracheostomized Varelas 2013 q 73% MICU n n n More toxic/metabolic enceph More GCSE Avg age: 51 Obtunded/comatose pts Higher APACHE 2 scores
 MICU vs NICU n No difference in outcomes q q n Length of ICU/hospital stay Functional status at discharge (m. RS) Limitations: q q Smaller NICU population Neuro illness with longer recovery period?
MICU vs NICU n No difference in outcomes q q n Length of ICU/hospital stay Functional status at discharge (m. RS) Limitations: q q Smaller NICU population Neuro illness with longer recovery period?
 KU Data
KU Data
 cases n") KU Cohort n Objective: q Review and describe non-convulsive status epilepticus (NCSE) cases n n Etiology Co-morbidities Medical treatment Clinical outcomes
KU Cohort n Objective: q Review and describe non-convulsive status epilepticus (NCSE) cases n n Etiology Co-morbidities Medical treatment Clinical outcomes
 KU Cohort n Methods: q Medical records reviewed from Jan 2009 -2013 n n n q ICD 9 for status epilepticus, at discharge CPT code for video-EEG monitoring ICU room charge during hospital stay Patients selected based on the following inclusion criteria: n n n Age: 10 - 110 years of age Diagnosis made utilizing routine or continuous video electroencephalogram Patients with hypoxic-ischemic brain injury were excluded
KU Cohort n Methods: q Medical records reviewed from Jan 2009 -2013 n n n q ICD 9 for status epilepticus, at discharge CPT code for video-EEG monitoring ICU room charge during hospital stay Patients selected based on the following inclusion criteria: n n n Age: 10 - 110 years of age Diagnosis made utilizing routine or continuous video electroencephalogram Patients with hypoxic-ischemic brain injury were excluded
 Data Demographics n 56 charts reviewed n 23 cases identified q q n M: 9 F: 14 Average age: 54 Presentation n 30% (7): q n 48% (11): q n GTC, tonic seizure(s) confusion, lethargy, somnolent 22% (5): q obtunded, stuporus, comatose
Data Demographics n 56 charts reviewed n 23 cases identified q q n M: 9 F: 14 Average age: 54 Presentation n 30% (7): q n 48% (11): q n GTC, tonic seizure(s) confusion, lethargy, somnolent 22% (5): q obtunded, stuporus, comatose
: Automatism, subtle motor mvts q q q n Head turning") Data n 35% (8): Automatism, subtle motor mvts q q q n Head turning Subtle limb, facial, tongue movements Eyelid flutter 22% (5): eye deviation
Data n 35% (8): Automatism, subtle motor mvts q q q n Head turning Subtle limb, facial, tongue movements Eyelid flutter 22% (5): eye deviation
 q q q LOS: 19. 2 d ICU: 11. 1") Data n CPSE (74%) q q q LOS: 19. 2 d ICU: 11. 1 d VEEG: 6. 1 d # AEDs: 2. 6 Anesthesia: 4. 6 d n ESE (13%) q q q LOS: 45. 7 d ICU: 20. 7 d VEEG: 8 d # AEDs: 3 Anesthesia: 7. 5 d
Data n CPSE (74%) q q q LOS: 19. 2 d ICU: 11. 1 d VEEG: 6. 1 d # AEDs: 2. 6 Anesthesia: 4. 6 d n ESE (13%) q q q LOS: 45. 7 d ICU: 20. 7 d VEEG: 8 d # AEDs: 3 Anesthesia: 7. 5 d
") Data- CPSE (17)
Data- CPSE (17)
 n Etiology q Severe sepsis n q OLT, ESRD on HD") Data- ESE (3) n Etiology q Severe sepsis n q OLT, ESRD on HD (2) CJD n n +14 -3 -3 Characteristic MRI (2)
Data- ESE (3) n Etiology q Severe sepsis n q OLT, ESRD on HD (2) CJD n n +14 -3 -3 Characteristic MRI (2)
 Increase") Data CPSE q AEDs: n n n ESE q 1 st: PHT (73%) Increase dose of AED Sedation VPA or Vimpat n n n Anesthesia: q Propofol (9/13) n n q q 2 pt + Versed Ketamine, pentobarb Versed (3/13)* Pentobarb (1/13)* AEDs: n 1 st: PHT (3) 2 nd: Keppra (3) Vimpat, PHB, topiramate (1) Anesthesia: q 1 st: Propofol (2) n Transition to Pentobarb = Versed q 1 pt: no tx
Data CPSE q AEDs: n n n ESE q 1 st: PHT (73%) Increase dose of AED Sedation VPA or Vimpat n n n Anesthesia: q Propofol (9/13) n n q q 2 pt + Versed Ketamine, pentobarb Versed (3/13)* Pentobarb (1/13)* AEDs: n 1 st: PHT (3) 2 nd: Keppra (3) Vimpat, PHB, topiramate (1) Anesthesia: q 1 st: Propofol (2) n Transition to Pentobarb = Versed q 1 pt: no tx
 q Pt#1: OLT on prograf n q Pt#2: Brain") EEG diagnosis not reported/unclear (3) q Pt#1: OLT on prograf n q Pt#2: Brain tumor n q L facial movements 3 GTC szs prolonged postictal Pt#3: Hx of epilepsy, liver failure n Poor responsiveness, eye flutter Age 56 LOS 23. 7 d ICU 10 d VEEG 6. 5 d AEDs 2 Sedation 4. 5 d
EEG diagnosis not reported/unclear (3) q Pt#1: OLT on prograf n q Pt#2: Brain tumor n q L facial movements 3 GTC szs prolonged postictal Pt#3: Hx of epilepsy, liver failure n Poor responsiveness, eye flutter Age 56 LOS 23. 7 d ICU 10 d VEEG 6. 5 d AEDs 2 Sedation 4. 5 d
 n 5/13: ≤ 15 WBCs (lymph)") Data n CSF: q n 46% abnormal (6/13) n 5/13: ≤ 15 WBCs (lymph) q q q n Meningoencephalitis (3) Inflamm WMD CJD +14 -3 -3 (1) Imaging q 22/23* n n 5 CT 17 MRI
Data n CSF: q n 46% abnormal (6/13) n 5/13: ≤ 15 WBCs (lymph) q q q n Meningoencephalitis (3) Inflamm WMD CJD +14 -3 -3 (1) Imaging q 22/23* n n 5 CT 17 MRI
 Transition to PLEDs") Data CPSE ESE n Time to resolution: q q Refractory (2) Transition to PLEDs (1)*
Data CPSE ESE n Time to resolution: q q Refractory (2) Transition to PLEDs (1)*
 Data n CPSE q Outcome: n n Death - 41% LTACH/SNF - 18% Home – 29% Rehab – 12% q One death within 30 d n ESE q Outcome: n Death or hospice – 100%
Data n CPSE q Outcome: n n Death - 41% LTACH/SNF - 18% Home – 29% Rehab – 12% q One death within 30 d n ESE q Outcome: n Death or hospice – 100%
: 51. 2 y q q n q n Epilepsy") CPSE Outcomes n Home (29%): 51. 2 y q q n q n Epilepsy (2) Remote stroke (1) Autoimmune enceph/SDH (1) Tumor (1) Rehab (12%): 57. 5 y q n Post-stroke epilepsy Autoimmune enceph LTACH/SNF (18%): 44 y q Epilepsy + illness or NC (3) Death (41%): 55. 6 y q q q Peritumoral stroke Remote stroke + sepsis Inflam WM lesions* CJD* MS + sepsis Meningoencephalitis (2)*
CPSE Outcomes n Home (29%): 51. 2 y q q n q n Epilepsy (2) Remote stroke (1) Autoimmune enceph/SDH (1) Tumor (1) Rehab (12%): 57. 5 y q n Post-stroke epilepsy Autoimmune enceph LTACH/SNF (18%): 44 y q Epilepsy + illness or NC (3) Death (41%): 55. 6 y q q q Peritumoral stroke Remote stroke + sepsis Inflam WM lesions* CJD* MS + sepsis Meningoencephalitis (2)*
: Sepsis q Death or hospice- 4 pts n n q") CPSE n 5/17 (29%): Sepsis q Death or hospice- 4 pts n n q CJD MS Peritumoral stroke Inflammatory WM lesions LTACH- 1 pt n Hx of epilepsy
CPSE n 5/17 (29%): Sepsis q Death or hospice- 4 pts n n q CJD MS Peritumoral stroke Inflammatory WM lesions LTACH- 1 pt n Hx of epilepsy
 Clinical outcome- CPSE n Follow-up in 5/10 q 2 pt: no new cognitive deficits n n q Epilepsy + NC <8 hr, <24 h 3 pt: memory impairment, assistance w/ ADLs, cognitive decline n n Tumor, AIE, menignoencephalitis <96 h, unknown (2)
Clinical outcome- CPSE n Follow-up in 5/10 q 2 pt: no new cognitive deficits n n q Epilepsy + NC <8 hr, <24 h 3 pt: memory impairment, assistance w/ ADLs, cognitive decline n n Tumor, AIE, menignoencephalitis <96 h, unknown (2)
 Limitations n Limited number of patients q n Majority from 2012, only 3 from 2009, 1 from 2010 Inclusion of patients with CJD q q 100% mortality Encephalopathy with epileptic features n Documentation, access to archived studies n Lack of clinical follow-up information n No cases of NCSE in acute stroke
Limitations n Limited number of patients q n Majority from 2012, only 3 from 2009, 1 from 2010 Inclusion of patients with CJD q q 100% mortality Encephalopathy with epileptic features n Documentation, access to archived studies n Lack of clinical follow-up information n No cases of NCSE in acute stroke
 Conclusions n Outcomes worse is ESE n Worse if underlying dx is CJD n Underlying epilepsy portends better outcome n Longer duration of uncontrolled NCSE adverse cognitive impact n Pt’s treated with Versed as initial agent, worse outcomes (2/3) death n Outcomes worse when pt diagnosed with sepsis
Conclusions n Outcomes worse is ESE n Worse if underlying dx is CJD n Underlying epilepsy portends better outcome n Longer duration of uncontrolled NCSE adverse cognitive impact n Pt’s treated with Versed as initial agent, worse outcomes (2/3) death n Outcomes worse when pt diagnosed with sepsis
 Thanks n n n Nancy Hammond, MD Utku Uysal, MD Ivan Osorio, MD William Nowack, MD Rhonda Reliford
Thanks n n n Nancy Hammond, MD Utku Uysal, MD Ivan Osorio, MD William Nowack, MD Rhonda Reliford
 References n n n Celesia CG. Modern concepts of status epilepticus. JAMA 1976: 235: 1771 -4. Tomson T, Svanbog, E, Wedlund J. E. Nonconvulsive status epilepticus: high incidence of complex partial status. Epilepsia. 1986; 27: 276 -85. Drislane F. Presentation, Evaluation, and Treatment of Nonconvulsive Status Epilepticus. Epilepsy and Behavior. 2000; 1: 301 -314. Towne AR. Prevalence of nonconvulsive status epilepticus in comatose patients. Neurology. 2000; 54(2): 340 -4. Krumholz A. Epidemiology and evidence for morbidity of nonconvulsive status epilepticus. J Clin Neurophysiology. 1999; 16(4): 314 -22. Meierkord H. The risk of epilepsy after status epilepticus in children and adults. Epilepsia. 2007; 48 suppl 8: 94 -5. Husain AM, Horn GJ, Jacobson MP. Non-convulsive status epilepticus: Usefulness of clinical features in selecting patients for urgent EEG. J. Neurol Neurosurg Psychiatry. 2003 Feb; 74(2): 189 -91. Young GB, Jordan KG, Doig GS. An assessment of nonconvulsive seizures in the intensive care unit using continuous EEG monitoring: An investigation of variables associated with mortality. Neurology. 1996 Jul; 47(1): 83 -9. Treiman DM, Walton NY, Kendrick C. A progressive sequence of electrographic changes during generalized convulsive status epilepticus. Epilepsy Res. 1990; 5: 49 -60. Walker M. Nonconvulsive status epilepticus: Epilepsy research foundation workshop reports. Epileptic Disord. 2005 Sep; 7(3): 253 -96. Walsh JM, Brenner RP. Periodic lateralized epileptiform discharges: long-term outcome in adults. Epilepsia 1987; 28: 533– 6.
References n n n Celesia CG. Modern concepts of status epilepticus. JAMA 1976: 235: 1771 -4. Tomson T, Svanbog, E, Wedlund J. E. Nonconvulsive status epilepticus: high incidence of complex partial status. Epilepsia. 1986; 27: 276 -85. Drislane F. Presentation, Evaluation, and Treatment of Nonconvulsive Status Epilepticus. Epilepsy and Behavior. 2000; 1: 301 -314. Towne AR. Prevalence of nonconvulsive status epilepticus in comatose patients. Neurology. 2000; 54(2): 340 -4. Krumholz A. Epidemiology and evidence for morbidity of nonconvulsive status epilepticus. J Clin Neurophysiology. 1999; 16(4): 314 -22. Meierkord H. The risk of epilepsy after status epilepticus in children and adults. Epilepsia. 2007; 48 suppl 8: 94 -5. Husain AM, Horn GJ, Jacobson MP. Non-convulsive status epilepticus: Usefulness of clinical features in selecting patients for urgent EEG. J. Neurol Neurosurg Psychiatry. 2003 Feb; 74(2): 189 -91. Young GB, Jordan KG, Doig GS. An assessment of nonconvulsive seizures in the intensive care unit using continuous EEG monitoring: An investigation of variables associated with mortality. Neurology. 1996 Jul; 47(1): 83 -9. Treiman DM, Walton NY, Kendrick C. A progressive sequence of electrographic changes during generalized convulsive status epilepticus. Epilepsy Res. 1990; 5: 49 -60. Walker M. Nonconvulsive status epilepticus: Epilepsy research foundation workshop reports. Epileptic Disord. 2005 Sep; 7(3): 253 -96. Walsh JM, Brenner RP. Periodic lateralized epileptiform discharges: long-term outcome in adults. Epilepsia 1987; 28: 533– 6.
 References n n n n n Snodgrass SM, Tsuburaya K, Ajmone-Marsan C. Clinical significance of periodic lateralized epileptiform discharges: Relationship with status epilepticus. J Clin Neurophysiol. 1989 Apr; 6(2): 159 -72. Kaplan PW. EEG criteria for nonconvulsive status epilepticus. Epilepsia. 2007; 48 Suppl 8: 39 -41. Chong DJ, Hirsch LJ. Which EEG patterns warrant treatment in the critically ill? Reviewing the evidence for treatment of periodic epileptiform discharges and related patterns. J Clin Neurophysiol. 2005 Apr; 22(2): 79 -91. Kaplan PW. EEG monitoring in the intensive care unit. Am J Electroneurodiagnostic Technol. 2006 Jun; 46(2): 81 -97. De. Lorenzo RJ, et al. Persistent nonconvulsive status epilepticus after the control of convulsive status epilepticus. Epilepsia. 1998 Aug; 39(8): 833 -40. Shneker BF, Fountain NB. Assessment of acute morbidity and mortality in nonconvulsive status epilepticus. Neurology. 2003 Oct 28; 61(8): 1066 -73. Granner MA, Lee SI. Nonconvulsive status epilepticus: EEG analysis in a large series. Epilepsia. 1994 Jan-Feb; 35(1): 42 -7. Claassen J, Hirsch LJ, Emerson RG, Mayer SA. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia. 2002 Feb; 43(2): 146 -53. Lothman EW, et al. Recurrent spontaneous hippocampal seizures in the rat as a chronic sequela to limbic status epilepticus. Epilepsy Res. 1990 Jul; 6(2): 110 -8.
References n n n n n Snodgrass SM, Tsuburaya K, Ajmone-Marsan C. Clinical significance of periodic lateralized epileptiform discharges: Relationship with status epilepticus. J Clin Neurophysiol. 1989 Apr; 6(2): 159 -72. Kaplan PW. EEG criteria for nonconvulsive status epilepticus. Epilepsia. 2007; 48 Suppl 8: 39 -41. Chong DJ, Hirsch LJ. Which EEG patterns warrant treatment in the critically ill? Reviewing the evidence for treatment of periodic epileptiform discharges and related patterns. J Clin Neurophysiol. 2005 Apr; 22(2): 79 -91. Kaplan PW. EEG monitoring in the intensive care unit. Am J Electroneurodiagnostic Technol. 2006 Jun; 46(2): 81 -97. De. Lorenzo RJ, et al. Persistent nonconvulsive status epilepticus after the control of convulsive status epilepticus. Epilepsia. 1998 Aug; 39(8): 833 -40. Shneker BF, Fountain NB. Assessment of acute morbidity and mortality in nonconvulsive status epilepticus. Neurology. 2003 Oct 28; 61(8): 1066 -73. Granner MA, Lee SI. Nonconvulsive status epilepticus: EEG analysis in a large series. Epilepsia. 1994 Jan-Feb; 35(1): 42 -7. Claassen J, Hirsch LJ, Emerson RG, Mayer SA. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia. 2002 Feb; 43(2): 146 -53. Lothman EW, et al. Recurrent spontaneous hippocampal seizures in the rat as a chronic sequela to limbic status epilepticus. Epilepsy Res. 1990 Jul; 6(2): 110 -8.
 References n n n Earnest MP, Thomas GE, Eden RA, Hossack KF. The sudden unexplained death syndrome in epilepsy: demographic, clinical, and postmortem features. Epilepsia. 1992 Mar -Apr; 33(2): 310 -6. Krumholz A. Complex partial status epilepticus accompanied by serious morbidity and mortality. Neurology. 1995 Aug; 45(8): 1499 -504. Drislane FW. Evidence against permanent neurologic damage from nonconvulsive status epilepticus. J Clin Neurophysiol. 1999 Jul; 16(4): 323 -31 Cockerell OC, Walker MC, Sander JW, Shorvon SD. Complex partial status epilepticus: a recurrent problem. J Neurol Neurosurg Psychiatry. 1994 Jul; 57(7): 835 -7. Varelas PN, et al. Emergent EEG: indications and diagnostic yield. Neurology. 2003 Sep 9; 61(5): 702 -4.
References n n n Earnest MP, Thomas GE, Eden RA, Hossack KF. The sudden unexplained death syndrome in epilepsy: demographic, clinical, and postmortem features. Epilepsia. 1992 Mar -Apr; 33(2): 310 -6. Krumholz A. Complex partial status epilepticus accompanied by serious morbidity and mortality. Neurology. 1995 Aug; 45(8): 1499 -504. Drislane FW. Evidence against permanent neurologic damage from nonconvulsive status epilepticus. J Clin Neurophysiol. 1999 Jul; 16(4): 323 -31 Cockerell OC, Walker MC, Sander JW, Shorvon SD. Complex partial status epilepticus: a recurrent problem. J Neurol Neurosurg Psychiatry. 1994 Jul; 57(7): 835 -7. Varelas PN, et al. Emergent EEG: indications and diagnostic yield. Neurology. 2003 Sep 9; 61(5): 702 -4.
 Thank you Questions? Comments?
Thank you Questions? Comments?