

8822c42c4fb4ddfc8f67cccee41b7169.ppt
- Количество слайдов: 45

 “New Nasty Viruses in Travellers from Overseas” How to spot MERS – Co. V and how to use the new VHF guidelines Rebecca Sutherland Consultant in Infectious Diseases Western General Hospital
“New Nasty Viruses in Travellers from Overseas” How to spot MERS – Co. V and how to use the new VHF guidelines Rebecca Sutherland Consultant in Infectious Diseases Western General Hospital
 Case 1 -July 2008 41 year old female, The Netherlands • • • Holiday in Uganda, returned 7/7 previously Exposure to bat caves, group of tourists 3/7 fever >39, rigors, rash, conjunctivitis, diarrhoea 2 days following admission, rapid deterioration: Liver and renal failure GI haemorrhage, bruising • • Day 5: Marburg fever PCR positive Day 6: Died of cerebral oedema • • • 130 at-risk contacts identified No transmission to contacts occurred Serological screening negative in all contacts • Timen A et al. Response to imported case of Marburg hemorrhagic fever, the Netherlands. Emerg Infect Dis. 2009 Aug •
Case 1 -July 2008 41 year old female, The Netherlands • • • Holiday in Uganda, returned 7/7 previously Exposure to bat caves, group of tourists 3/7 fever >39, rigors, rash, conjunctivitis, diarrhoea 2 days following admission, rapid deterioration: Liver and renal failure GI haemorrhage, bruising • • Day 5: Marburg fever PCR positive Day 6: Died of cerebral oedema • • • 130 at-risk contacts identified No transmission to contacts occurred Serological screening negative in all contacts • Timen A et al. Response to imported case of Marburg hemorrhagic fever, the Netherlands. Emerg Infect Dis. 2009 Aug •
 Case 2 2009 • • • 20 year old male Medically evacuated from village in southern Mali to UK 10 day history fever Diagnosis locally of falciparum malaria Failure to improve despite IV quinine therapy Rapid deterioration on day of admission within six hours, with hypotension and progressive multiorgan failure Transfer to high security ID unit Died same day PCR: Lassa fever Malaria antigen, microscopy: negative
Case 2 2009 • • • 20 year old male Medically evacuated from village in southern Mali to UK 10 day history fever Diagnosis locally of falciparum malaria Failure to improve despite IV quinine therapy Rapid deterioration on day of admission within six hours, with hypotension and progressive multiorgan failure Transfer to high security ID unit Died same day PCR: Lassa fever Malaria antigen, microscopy: negative
 Case 3 - September 2008 • • • 35 year old male travel agent, living on agricultural small holding on outskirts of Lusaka, Zambia Day 1: Severe headache, malaise 4/7 later, started antivirals for suspected influenza Day 8: fever, chest pain, sore throat Commenced antiemetics, oral cephalosporin Rash, myalgia, facial swelling: presumed allergy to antibiotics
Case 3 - September 2008 • • • 35 year old male travel agent, living on agricultural small holding on outskirts of Lusaka, Zambia Day 1: Severe headache, malaise 4/7 later, started antivirals for suspected influenza Day 8: fever, chest pain, sore throat Commenced antiemetics, oral cephalosporin Rash, myalgia, facial swelling: presumed allergy to antibiotics
 Progress • • Day 12: Air ambulance evacuation to South Africa Deterioration on flight: Intubated/ventilated • • • Arrival in SA: Cerebral oedema confirmed by CT head. No pupillary reflexes ITU admission: ventilation, haemodialysis Thrombocytopenia, raised ALT • Evidence of eschar right foot: treated for suspected rickettsiosis • Day 14: died of multi-organ failure
Progress • • Day 12: Air ambulance evacuation to South Africa Deterioration on flight: Intubated/ventilated • • • Arrival in SA: Cerebral oedema confirmed by CT head. No pupillary reflexes ITU admission: ventilation, haemodialysis Thrombocytopenia, raised ALT • Evidence of eschar right foot: treated for suspected rickettsiosis • Day 14: died of multi-organ failure
 • • • Paramedic for air evacuation: headache, fever, myalgia Died 2 weeks into illness Nurse who attended index patient in S. Africa (including cleaning body): died Cleaner in hospital, cleaned cubicle where patient treated: died Nurse in hospital: fever, myalgia, recovered All patients: Confirmed novel arenavirus by viral cell culture • • • 123 contacts identified Category 3 contacts offered ribavirin No further transmission occurred • Atkin S et al. The first case of Lassa imported from Mali to the United Kingdom. Eurosurveillance 2009
• • • Paramedic for air evacuation: headache, fever, myalgia Died 2 weeks into illness Nurse who attended index patient in S. Africa (including cleaning body): died Cleaner in hospital, cleaned cubicle where patient treated: died Nurse in hospital: fever, myalgia, recovered All patients: Confirmed novel arenavirus by viral cell culture • • • 123 contacts identified Category 3 contacts offered ribavirin No further transmission occurred • Atkin S et al. The first case of Lassa imported from Mali to the United Kingdom. Eurosurveillance 2009
 VHF • Severe life threatening viral diseases • Particular public health importance because • • can spread in a hospital setting high case fatality rate difficult to recognise and detect rapidly no effective treatment • Environmental conditions in the UK do not support the natural reservoirs or vectors of any of the viruses
VHF • Severe life threatening viral diseases • Particular public health importance because • • can spread in a hospital setting high case fatality rate difficult to recognise and detect rapidly no effective treatment • Environmental conditions in the UK do not support the natural reservoirs or vectors of any of the viruses
 October 2012
October 2012
 Oct 2012 • • 38 year old male 3 week trip to Afghanistan- Kabul and Samangan Province to attend a wedding Return travel via Kabul, Dubai, Glasgow 5 day illness Myalgia, fever, diarrhoea, abdominal pain Unwell in Afghanistan since end Sep with myalgia, loose bloody stool, cramping abdo pain , cough and headache Told he had typhoid at local clinic and given antibiotics
Oct 2012 • • 38 year old male 3 week trip to Afghanistan- Kabul and Samangan Province to attend a wedding Return travel via Kabul, Dubai, Glasgow 5 day illness Myalgia, fever, diarrhoea, abdominal pain Unwell in Afghanistan since end Sep with myalgia, loose bloody stool, cramping abdo pain , cough and headache Told he had typhoid at local clinic and given antibiotics
 Progress • • • 1 st Oct flew from Kabul to Dubai then Glasgow Diarrhoea and vomiting on flight Landed Glasgow 1330 hrs, travels home in private car Greet family Further D + V Unwell so calls for ambulance • Arrives Southern General Hospital, Glasgow 1530 hrs • • Informs A and E staff might have typhoid so put in side room Referred to ID
Progress • • • 1 st Oct flew from Kabul to Dubai then Glasgow Diarrhoea and vomiting on flight Landed Glasgow 1330 hrs, travels home in private car Greet family Further D + V Unwell so calls for ambulance • Arrives Southern General Hospital, Glasgow 1530 hrs • • Informs A and E staff might have typhoid so put in side room Referred to ID
 Assessment VHF new guidelines-ACDP • Arrives Brownlee by Scottish Ambulance Service • Isolated neg pressure room • ID consultant raises possibility of CCHF • Patient denied animal contact/ tick exposure • • Platelets 10, AST 6383, ALT 2157 Differential Dengue, typhoid, rickettsia, malaria
Assessment VHF new guidelines-ACDP • Arrives Brownlee by Scottish Ambulance Service • Isolated neg pressure room • ID consultant raises possibility of CCHF • Patient denied animal contact/ tick exposure • • Platelets 10, AST 6383, ALT 2157 Differential Dengue, typhoid, rickettsia, malaria
 Assessment VHF new guidelines-ACDP • 3 rd Oct- petechial rash, spontaneous haematoma left tibia, haemoptysis over venepuncture sites, conjunctival suffusion, tender epigastrium • Mobile phone pictures
Assessment VHF new guidelines-ACDP • 3 rd Oct- petechial rash, spontaneous haematoma left tibia, haemoptysis over venepuncture sites, conjunctival suffusion, tender epigastrium • Mobile phone pictures

 Possible CCHF • Blood and urine dispatched to HPA Porton by road courier service 1000 hrs 3/10/12 • CCHF PCR positive, result telephoned 0100 4/10/12 Pt commenced on ribavarin Public Health notified • • • Medical deterioration Haemorrhage Transferred to High security Unit Royal Free by RAF • • Died on day 4 after massive haemoptysis No other cases • Atkinson B et al. Sequencing and phylogenetic characterisation of a fatal Crimean – Congo haemorrhagic fever case imported into the United Kingdom, October 2012. Eurosurveillance 2012
Possible CCHF • Blood and urine dispatched to HPA Porton by road courier service 1000 hrs 3/10/12 • CCHF PCR positive, result telephoned 0100 4/10/12 Pt commenced on ribavarin Public Health notified • • • Medical deterioration Haemorrhage Transferred to High security Unit Royal Free by RAF • • Died on day 4 after massive haemoptysis No other cases • Atkinson B et al. Sequencing and phylogenetic characterisation of a fatal Crimean – Congo haemorrhagic fever case imported into the United Kingdom, October 2012. Eurosurveillance 2012
 CCHF • Concentration of people and livestock in endemic areas • • 1944 - USSR forces drove Germans out of Crimea Farming activities paralysed by German occupation Overgrown pastureland, abundant hare population After Soviets recovered Crimea and restored agriculture, around 200 soldiers and new settlers began to fall ill • • Congo 1956 -Febrile patient in Belgian Congo Viral culture: antigenically indistinguishable from Crimean haemorrhagic fever (including Eurasian strains)
CCHF • Concentration of people and livestock in endemic areas • • 1944 - USSR forces drove Germans out of Crimea Farming activities paralysed by German occupation Overgrown pastureland, abundant hare population After Soviets recovered Crimea and restored agriculture, around 200 soldiers and new settlers began to fall ill • • Congo 1956 -Febrile patient in Belgian Congo Viral culture: antigenically indistinguishable from Crimean haemorrhagic fever (including Eurasian strains)
 CCHF • • Tick-vertebrate-tick cycle Hyalomma spp. ticks Animal reservoir: Cattle, sheep, goats, pigs, hares Nosocomial infection via blood and body fluids across mucous membranes
CCHF • • Tick-vertebrate-tick cycle Hyalomma spp. ticks Animal reservoir: Cattle, sheep, goats, pigs, hares Nosocomial infection via blood and body fluids across mucous membranes
 Fever 39") Clinical • • • Incubation: 3 -12 days (shorter with bloodborne transmission) Fever 39 -40, headache, myalgia, dizziness Diarrhoea, vomiting, nausea At 3 -5 days: petechiae, haematomas, GI bleed, menorrhagia, haemoptysis Hepatomegaly, splenomegaly 20 -40% • • • Thrombocytopenia Prolonged PT, APTT Elevated ALT, AST, LDH • DIC – mortality 3 -30%
Clinical • • • Incubation: 3 -12 days (shorter with bloodborne transmission) Fever 39 -40, headache, myalgia, dizziness Diarrhoea, vomiting, nausea At 3 -5 days: petechiae, haematomas, GI bleed, menorrhagia, haemoptysis Hepatomegaly, splenomegaly 20 -40% • • • Thrombocytopenia Prolonged PT, APTT Elevated ALT, AST, LDH • DIC – mortality 3 -30%
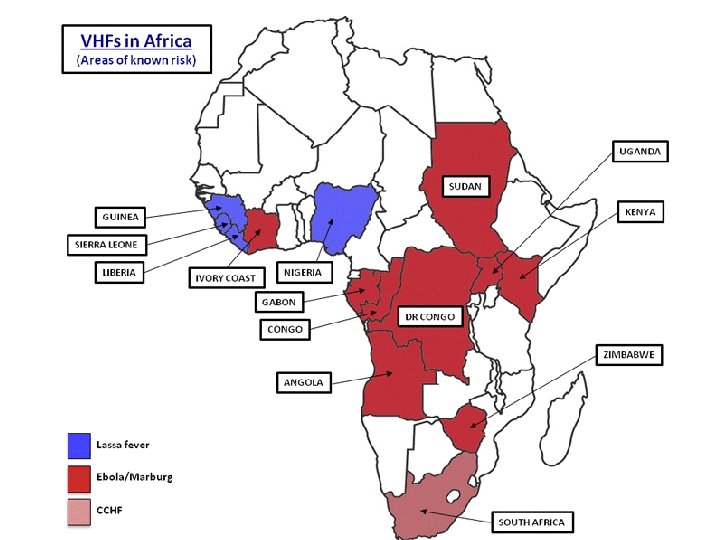
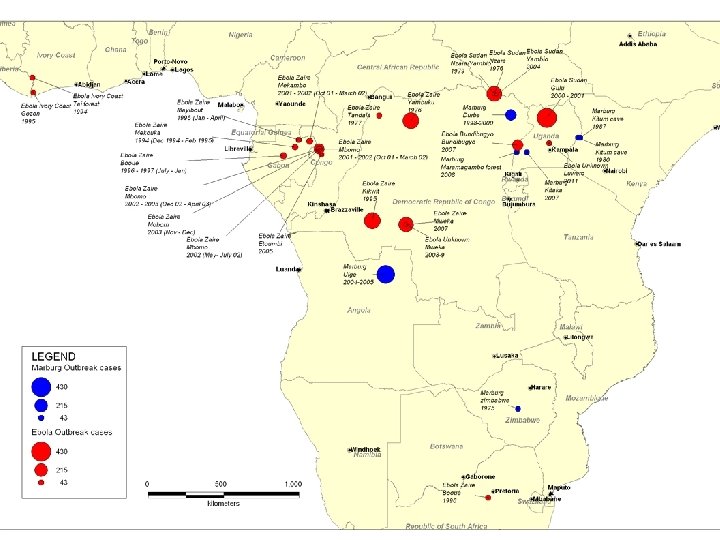
 Epidemiology
Epidemiology

 Other viral haemorrhagic fevers • Lassa: Endemic Western Africa: 12 imported cases since 1970 in UK • • • Arenavirus Rodent reservoir West Africa Human infection usually asymptomatic (80%) Incubation 5 -7 days • 2 missionary nurses died in town of Lassa, Nigeria in 1969
Other viral haemorrhagic fevers • Lassa: Endemic Western Africa: 12 imported cases since 1970 in UK • • • Arenavirus Rodent reservoir West Africa Human infection usually asymptomatic (80%) Incubation 5 -7 days • 2 missionary nurses died in town of Lassa, Nigeria in 1969
 Marburg and Ebola • • • Filovirus Fruit bats: reservoir uncertain Transmission through caves, mines, healthcare settings, laboratories Small, localised epidemics in Western and Central Africa 20 - 90% case fatality rate Incubation 3 - 16 days
Marburg and Ebola • • • Filovirus Fruit bats: reservoir uncertain Transmission through caves, mines, healthcare settings, laboratories Small, localised epidemics in Western and Central Africa 20 - 90% case fatality rate Incubation 3 - 16 days
 The RIDU protocol for suspected VHF • • • Risk assessment of the potential for infection with VHF People who satisfy the following criteria should be considered at risk 1. Patients with a fever >38 or a history of fever who have returned from a VHF endemic area within 21 days Or… 2. Fever as above who have cared for/ come into contact with body fluids/ handled a clinical specimen from a live or dead individual or animal known/ suspected to have VHF Risk assesment should then follow the Do. H guidelines
The RIDU protocol for suspected VHF • • • Risk assessment of the potential for infection with VHF People who satisfy the following criteria should be considered at risk 1. Patients with a fever >38 or a history of fever who have returned from a VHF endemic area within 21 days Or… 2. Fever as above who have cared for/ come into contact with body fluids/ handled a clinical specimen from a live or dead individual or animal known/ suspected to have VHF Risk assesment should then follow the Do. H guidelines
 Transfer of the patient with suspected VHF • Possibility of VHF- transported using category 2 removal= ambulance staff wearing overalls, gloves, masks, gowns and overshoes • High possibility of VHF- category 3 removal= removal of ambulance equipment, sealing the patient compartment, using respirators and disposable clothing and extensive disinfection following transfer. • Confirmed VHF- discuss with the High security Infectious Diseases Unit in London, transfer with use of category 4 removal- use of the SORT team (Scottish ambulance Service Special Operations Team). Transport by air likely to be required.
Transfer of the patient with suspected VHF • Possibility of VHF- transported using category 2 removal= ambulance staff wearing overalls, gloves, masks, gowns and overshoes • High possibility of VHF- category 3 removal= removal of ambulance equipment, sealing the patient compartment, using respirators and disposable clothing and extensive disinfection following transfer. • Confirmed VHF- discuss with the High security Infectious Diseases Unit in London, transfer with use of category 4 removal- use of the SORT team (Scottish ambulance Service Special Operations Team). Transport by air likely to be required.
 High possibility of VHF • One nominated Dr and member of nursing staff should care for the patient per 12 hour shift • Initial malaria film conducted at RIE • Depending on the result the assessment may be revised/ further samples sent to HPA in Porton following discussion with the fever service • The on call virologist will authorise the initiation of tests and organise transport by Category A container
High possibility of VHF • One nominated Dr and member of nursing staff should care for the patient per 12 hour shift • Initial malaria film conducted at RIE • Depending on the result the assessment may be revised/ further samples sent to HPA in Porton following discussion with the fever service • The on call virologist will authorise the initiation of tests and organise transport by Category A container
 PPE • • • Surgical cap Respirator mask Disposable visor Overshoes Surgical gown 2 pairs of gloves
PPE • • • Surgical cap Respirator mask Disposable visor Overshoes Surgical gown 2 pairs of gloves
 On balance • • Febrile patients are 1000 times more likely to have malaria than VHF No reported transmission in fellow travellers and no nosocomial transmission reported in Western healthcare settings • Imported fever • • 2000 -2009 17, 000 cases of malaria 4200 typhoid 4 cases VHF • Beeching NJ, at al. Travellers and viral haemorrhagic fevers: what are the risks? Int J Antimicrob Agents. 2010 Nov; 36 Suppl 1: S 26 -35
On balance • • Febrile patients are 1000 times more likely to have malaria than VHF No reported transmission in fellow travellers and no nosocomial transmission reported in Western healthcare settings • Imported fever • • 2000 -2009 17, 000 cases of malaria 4200 typhoid 4 cases VHF • Beeching NJ, at al. Travellers and viral haemorrhagic fevers: what are the risks? Int J Antimicrob Agents. 2010 Nov; 36 Suppl 1: S 26 -35
 But we should be prepared • Case not far from here • • • ACDP flow chart is usable- disseminate to key areas Updated our protocol Alerting new staff to consider this diagnosis in differential Audit- 11 possible cases only 1 d/w ID on admission ID and virology then deal with the probabilities Isolate until proven otherwise
But we should be prepared • Case not far from here • • • ACDP flow chart is usable- disseminate to key areas Updated our protocol Alerting new staff to consider this diagnosis in differential Audit- 11 possible cases only 1 d/w ID on admission ID and virology then deal with the probabilities Isolate until proven otherwise
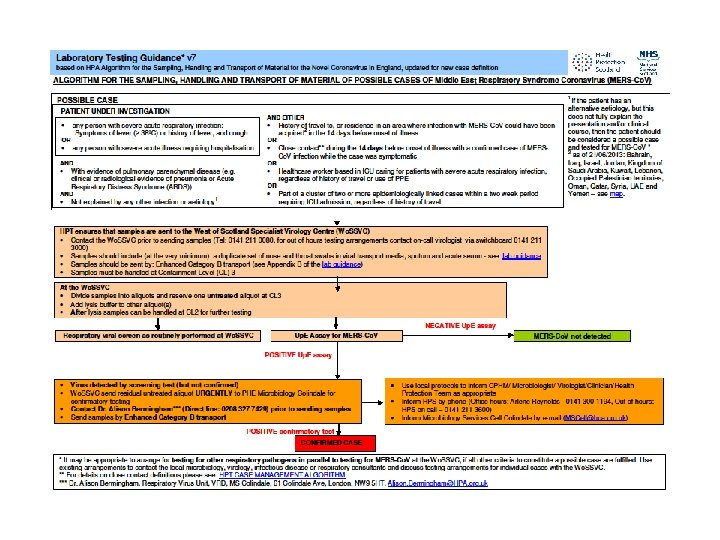
 Mers Co. V Middle East respiratory syndrome coronavirus
Mers Co. V Middle East respiratory syndrome coronavirus
 Middle East respiratory syndrome coronavirus • • • First reported in Sep 2012 in Saudi Arabiasevere pneumonia and AKI Few days later similar presentation with an almost identical virus in patient from Saudi Arabia who sought care in the UK Report on Pro. Med Mail • Beta coronavirus, different from other human betacoronaviruses (severe acute respiratory syndrome coronavirus) • • CD 26, present on human non ciliated bronchial epithelial cells is a functional receptor for the virus Broad tissue tropism- lower respiratory, kidney, intestinal and liver cells Evolutionary rate virus- emerged July 2011 • 130 laboratory cases to date •
Middle East respiratory syndrome coronavirus • • • First reported in Sep 2012 in Saudi Arabiasevere pneumonia and AKI Few days later similar presentation with an almost identical virus in patient from Saudi Arabia who sought care in the UK Report on Pro. Med Mail • Beta coronavirus, different from other human betacoronaviruses (severe acute respiratory syndrome coronavirus) • • CD 26, present on human non ciliated bronchial epithelial cells is a functional receptor for the virus Broad tissue tropism- lower respiratory, kidney, intestinal and liver cells Evolutionary rate virus- emerged July 2011 • 130 laboratory cases to date •
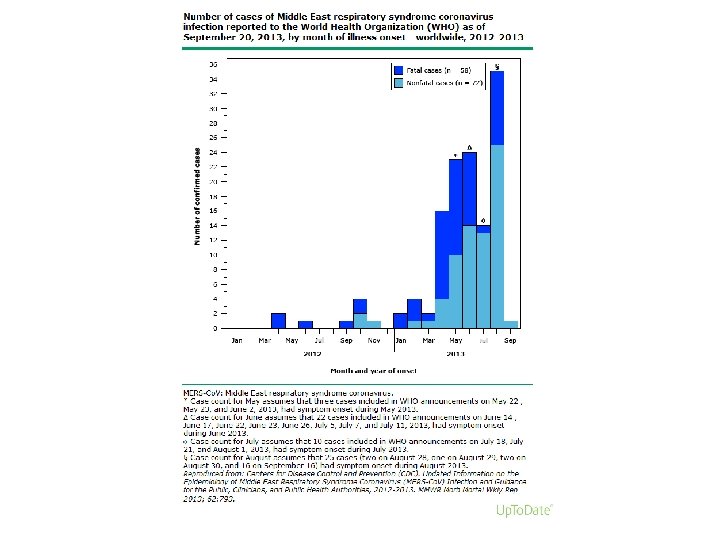
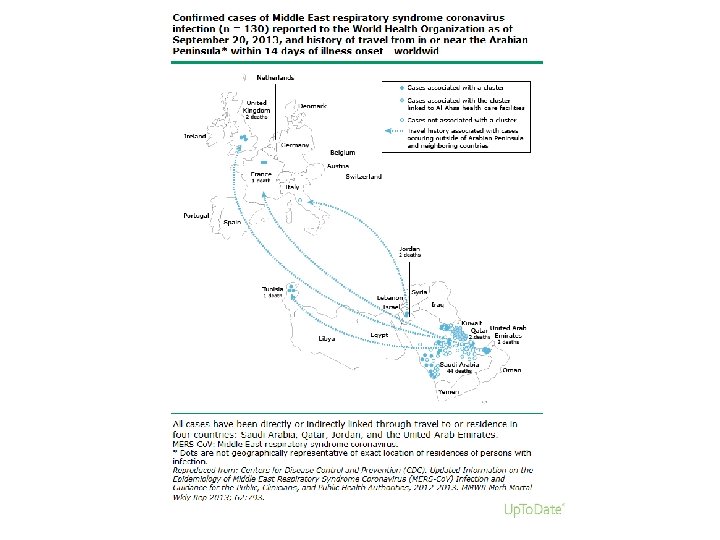
 Cases and clusters • Began with 3 separate cases • Oct and nov 2012 four men in one family in Riyadh, 2 cases fatal. None of 24 family members nor 124 healthcare workers became ill • 2 further cases in cluster 11 pneumonia cases. Pneumonia and DIC, pneumonia and pericarditiis. • Jan 2013 resident UK visited Saudi Arabia, died of severe respiratory illness (MERS- Co. V and H 1 N 1 influenza A detected). Feb 2013 son (underlying medical condition) died from MERS Co. V infection after close contact – 2 further milder cases in family • April 2013 23 cluster cases in Saudia Arabia, direct person- person exposure, most in haemodialysis. 2 healthcare workers and 3 family members • May 2013 5 cases eastern Saudi, all had co morbidities • May 2013 pt in France dev MERS Co. V after holiday in UAE, second patient diagnosed having shared room with first patient. First pt dies, second pt on ECMO. Both had co morbidities • ….
Cases and clusters • Began with 3 separate cases • Oct and nov 2012 four men in one family in Riyadh, 2 cases fatal. None of 24 family members nor 124 healthcare workers became ill • 2 further cases in cluster 11 pneumonia cases. Pneumonia and DIC, pneumonia and pericarditiis. • Jan 2013 resident UK visited Saudi Arabia, died of severe respiratory illness (MERS- Co. V and H 1 N 1 influenza A detected). Feb 2013 son (underlying medical condition) died from MERS Co. V infection after close contact – 2 further milder cases in family • April 2013 23 cluster cases in Saudia Arabia, direct person- person exposure, most in haemodialysis. 2 healthcare workers and 3 family members • May 2013 5 cases eastern Saudi, all had co morbidities • May 2013 pt in France dev MERS Co. V after holiday in UAE, second patient diagnosed having shared room with first patient. First pt dies, second pt on ECMO. Both had co morbidities • ….
 Possible sources and modes of transmission • • • Thought to be of animal origin Related to several bat coronaviruses Case clusters suggest human- human transmission • Closely related sequences in bat faecal samples with one identical sequence near the home of an infected patient • Probable reservoir because human contact uncommon Intermediate host ? Camel 100% dromedary camels in Oman have spec Ig. G against subunit protein MERSCo. V vs 15% those in Canary Islands • • • But no cases in Oman and only serology so may be cross reaction
Possible sources and modes of transmission • • • Thought to be of animal origin Related to several bat coronaviruses Case clusters suggest human- human transmission • Closely related sequences in bat faecal samples with one identical sequence near the home of an infected patient • Probable reservoir because human contact uncommon Intermediate host ? Camel 100% dromedary camels in Oman have spec Ig. G against subunit protein MERSCo. V vs 15% those in Canary Islands • • • But no cases in Oman and only serology so may be cross reaction
 The new SARS? • • • Probable droplet and contact transmission The effective reproduction number (R 0; defined as the average number of infections caused by one individual in a fully susceptible population) = 0. 69 If R 0<1 then unlikely to have pandemic potential • SARS estimated R 0 2. 2 to 3. 7, swine flu 1. 4 • Similar virologically but different mechanisms to infect human airways • Not adapting to human infection as rapidly as SARS • Enhanced surveillance, active contact tracing, vigorous searches for animal hosts • Proposed that SARS could have been controlled earlier when it was still confined to SE Asia
The new SARS? • • • Probable droplet and contact transmission The effective reproduction number (R 0; defined as the average number of infections caused by one individual in a fully susceptible population) = 0. 69 If R 0<1 then unlikely to have pandemic potential • SARS estimated R 0 2. 2 to 3. 7, swine flu 1. 4 • Similar virologically but different mechanisms to infect human airways • Not adapting to human infection as rapidly as SARS • Enhanced surveillance, active contact tracing, vigorous searches for animal hosts • Proposed that SARS could have been controlled earlier when it was still confined to SE Asia
 Clinical Findings and Test Results in Two Patients in Saudi Arabia and Four Patients in the Family Cluster with Confirmed or Probable MERS-Co. V Infection, as Compared with Patients with SARSCo. V Infection. Memish ZA et al. N Engl J Med 2013; 368: 2487 -2494.
Clinical Findings and Test Results in Two Patients in Saudi Arabia and Four Patients in the Family Cluster with Confirmed or Probable MERS-Co. V Infection, as Compared with Patients with SARSCo. V Infection. Memish ZA et al. N Engl J Med 2013; 368: 2487 -2494.
 •") Clinical manifestations • Incubation period: 5 days (although french cases 9 -12 days) • Consider in pts returning from Arabian peninsula or neighbouring countries within the past 14 days • Clinical features: Pneumonia, ARDS, AKI • Other symptoms: anorexia, nausea, vomiting, abdo pain, diarrhoea, pericarditis, DIC • Study of 47 pts with MERS-Co. V in Saudi Arabia 96% had underlying co morbidities -68% DM, hypertension (34%) chronic cardiac disease (28%), chronic kidney disease (49%)
Clinical manifestations • Incubation period: 5 days (although french cases 9 -12 days) • Consider in pts returning from Arabian peninsula or neighbouring countries within the past 14 days • Clinical features: Pneumonia, ARDS, AKI • Other symptoms: anorexia, nausea, vomiting, abdo pain, diarrhoea, pericarditis, DIC • Study of 47 pts with MERS-Co. V in Saudi Arabia 96% had underlying co morbidities -68% DM, hypertension (34%) chronic cardiac disease (28%), chronic kidney disease (49%)
 •") Clinical manifestations • Incubation period: 5 days (although french cases 9 -12 days) • Consider in pts returning from Arabian peninsula or neighbouring countries= • Bahrain, Iraq, Iran, Israel, Jordan, Kuwait, Lebanon, Oman, Palestinian territories, Qatar, Saudi Arabia, Syria, the United Arab Emrites and Yemen.
Clinical manifestations • Incubation period: 5 days (although french cases 9 -12 days) • Consider in pts returning from Arabian peninsula or neighbouring countries= • Bahrain, Iraq, Iran, Israel, Jordan, Kuwait, Lebanon, Oman, Palestinian territories, Qatar, Saudi Arabia, Syria, the United Arab Emrites and Yemen.
 • • Person with acute respiratory infection who") Who to test (WHO and CDC) • • Person with acute respiratory infection who requires admission to hospital and any of the following • The disease occurs in a cluster of respiratory illness that occurs within a 14 day period (2 or more persons associated with a specific setting eg classroom, workplace, barracks), unless another aetiology has been established. Occurs in a healthcare worker who has cared for pts with acute r/s infections Travel to Middle East within 14 days before the onset of the illness Person has an unusual or unexpected clinical course without regard to above • • •
Who to test (WHO and CDC) • • Person with acute respiratory infection who requires admission to hospital and any of the following • The disease occurs in a cluster of respiratory illness that occurs within a 14 day period (2 or more persons associated with a specific setting eg classroom, workplace, barracks), unless another aetiology has been established. Occurs in a healthcare worker who has cared for pts with acute r/s infections Travel to Middle East within 14 days before the onset of the illness Person has an unusual or unexpected clinical course without regard to above • • •
 Travel recommendations • Ministry Health Saudi Arabia recommends following postpone their trip to Mecca • • >65 yrs old Individuals with chronic diseases Individuals with immunodeficiency Patients with malignancy Patients with a terminal illness Pregnant women Children (<12 yrs) • • •
Travel recommendations • Ministry Health Saudi Arabia recommends following postpone their trip to Mecca • • >65 yrs old Individuals with chronic diseases Individuals with immunodeficiency Patients with malignancy Patients with a terminal illness Pregnant women Children (<12 yrs) • • •
 Isolation and Treatment • Standard, contact and airborne precautions • No antivirals currently recommended • In cell culture and animal experiments IFN alpha 2 b and ribavarin appears promising • • • Isolation: x rooms in RIDU with negative pressure facility Occupied with MDR TB Face masks- FFP 3 Fit testing HSE report
Isolation and Treatment • Standard, contact and airborne precautions • No antivirals currently recommended • In cell culture and animal experiments IFN alpha 2 b and ribavarin appears promising • • • Isolation: x rooms in RIDU with negative pressure facility Occupied with MDR TB Face masks- FFP 3 Fit testing HSE report
 Thank you
Thank you