

e8642fd3ba9c135c522173d2f57e713a.ppt
- Количество слайдов: 81
 Neurotrauma James F. Holmes, MD, MPH Professor, Department of Emergency Medicine University of California at Davis - School of Medicine Director, EM Research Fellowship Director, Department of EM Journal Club Davis, California
Neurotrauma James F. Holmes, MD, MPH Professor, Department of Emergency Medicine University of California at Davis - School of Medicine Director, EM Research Fellowship Director, Department of EM Journal Club Davis, California
 • Diagnosis of patients") Objectives • Epidemiology • Types of traumatic brain injuries (TBI) • Diagnosis of patients with TBI • Treatment of TBI
Objectives • Epidemiology • Types of traumatic brain injuries (TBI) • Diagnosis of patients with TBI • Treatment of TBI
 Essentials of TBI • Most traumatic deaths secondary to TBI • Secondary brain injury may cause morbidity and mortality but is often preventable • Initial Resuscitation and care: – Maintain oxygenation – Appropriate ventilation – Maintain blood pressure (prevent hypotension) • Cranial CT scanning is the diagnostic test of choice
Essentials of TBI • Most traumatic deaths secondary to TBI • Secondary brain injury may cause morbidity and mortality but is often preventable • Initial Resuscitation and care: – Maintain oxygenation – Appropriate ventilation – Maintain blood pressure (prevent hypotension) • Cranial CT scanning is the diagnostic test of choice
 brain injury – Structural damage from the initial impact –") Pathophysiology • Primary (initial) brain injury – Structural damage from the initial impact – Prevention strategies to minimize the number of patients sustaining head injuries • Example: motorcycle helmets
Pathophysiology • Primary (initial) brain injury – Structural damage from the initial impact – Prevention strategies to minimize the number of patients sustaining head injuries • Example: motorcycle helmets
 Pathophysiology • Secondary brain injury – Tissue injury occurring after the initial injury • Usually in the initial 24 hours • Hypoxia • Mass effect • Limited blood flow • Infection • Hyperthermia – Treatment goal: prevent these types of insults with appropriate treatment
Pathophysiology • Secondary brain injury – Tissue injury occurring after the initial injury • Usually in the initial 24 hours • Hypoxia • Mass effect • Limited blood flow • Infection • Hyperthermia – Treatment goal: prevent these types of insults with appropriate treatment
 • Goal") Pathophysiology • CPP = MAP - ICP – Cerebral perfusion pressure (CPP) • Goal is > 70 mm. Hg – Mean Arterial Pressure (MAP) – Intracranial Pressure (ICP) • Intracranial pressure may be with: – mass effect of a bleed – generalized brain edema • Cellular dysfunction occurs with decreased perfusion to the brain cells
Pathophysiology • CPP = MAP - ICP – Cerebral perfusion pressure (CPP) • Goal is > 70 mm. Hg – Mean Arterial Pressure (MAP) – Intracranial Pressure (ICP) • Intracranial pressure may be with: – mass effect of a bleed – generalized brain edema • Cellular dysfunction occurs with decreased perfusion to the brain cells
 Types of Injuries • • Skull Fracture Concussion Contusion Intracranial hematoma – Epidural, Subdural, Epidural, Intracerebral • Diffuse axonal injury • Intraventricular and Subarrachnoid hemorrhages • Penetrating injury
Types of Injuries • • Skull Fracture Concussion Contusion Intracranial hematoma – Epidural, Subdural, Epidural, Intracerebral • Diffuse axonal injury • Intraventricular and Subarrachnoid hemorrhages • Penetrating injury
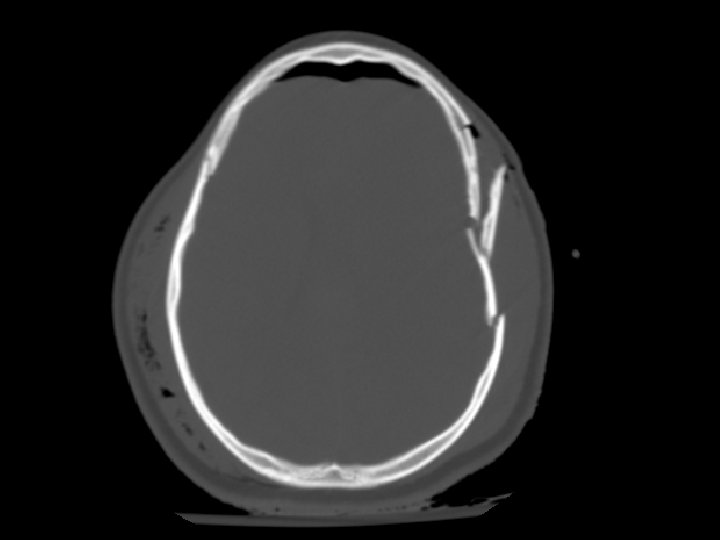
 Skull Fracture • Multiple types: – Linear, depressed, and basilar • CT must be viewed on bone windows • Most important feature is injury occurring to the brain at the site of the skull fracture • Linear skull fracture: – If closed, can simply be observed
Skull Fracture • Multiple types: – Linear, depressed, and basilar • CT must be viewed on bone windows • Most important feature is injury occurring to the brain at the site of the skull fracture • Linear skull fracture: – If closed, can simply be observed
 Skull Fracture • Basilar skull fracture: – Most often involving the temporal bone – Clinical diagnosis (CT often fails to show fracture) • Raccoon’s (Panda’s) eyes, hemotympanum, Battle’s sign (mastoid ecchymosis), CSF rhinorrhea • Depressed skull fracture: – Surgical elevation: • if greater than width of skull or • > 5 mm
Skull Fracture • Basilar skull fracture: – Most often involving the temporal bone – Clinical diagnosis (CT often fails to show fracture) • Raccoon’s (Panda’s) eyes, hemotympanum, Battle’s sign (mastoid ecchymosis), CSF rhinorrhea • Depressed skull fracture: – Surgical elevation: • if greater than width of skull or • > 5 mm


 Concussion • Brief change in brain function usually with loss of consciousness/amnesia • Head CT often normal • Post-concussive syndrome: – Headache, confusion, difficulty concentrating, memory problems, nausea – May last hours to months • Treatment – Simple observation – Limit activity that may reinjure patient’s head • Avoid “repeat concussion”
Concussion • Brief change in brain function usually with loss of consciousness/amnesia • Head CT often normal • Post-concussive syndrome: – Headache, confusion, difficulty concentrating, memory problems, nausea – May last hours to months • Treatment – Simple observation – Limit activity that may reinjure patient’s head • Avoid “repeat concussion”
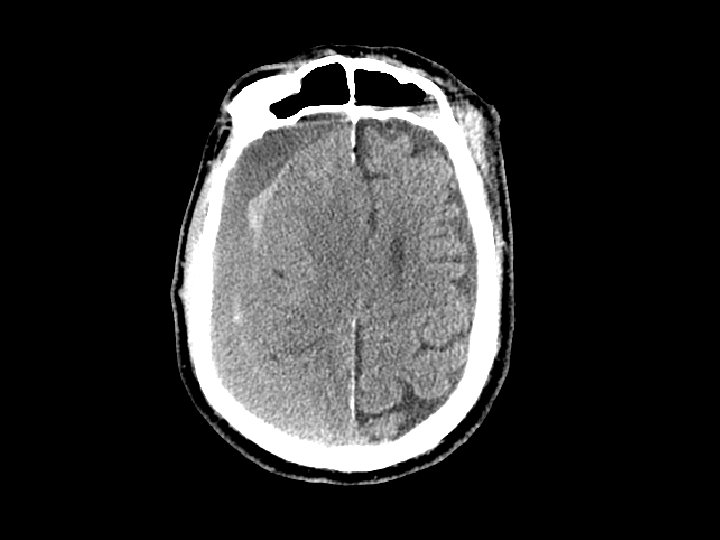
 Cerebral Contusion • Bruising to the brain • Most common traumatic finding on CT • Large contusions may have significant bleeding (hemorrhagic contusion or intracerebral hematoma), edema, or cause seizures • Location: Frontal and Temporal lobes – Due to irregularity of the skull base • Treatment: close observation
Cerebral Contusion • Bruising to the brain • Most common traumatic finding on CT • Large contusions may have significant bleeding (hemorrhagic contusion or intracerebral hematoma), edema, or cause seizures • Location: Frontal and Temporal lobes – Due to irregularity of the skull base • Treatment: close observation
 • Hemorrhage “above” the dura – Usually arterial (middle meningeal artery)") Epidural Hematoma (EDH) • Hemorrhage “above” the dura – Usually arterial (middle meningeal artery) but can also be from venous bleeding • CT: convex (lens shaped) area of blood – Bleeding restricted by the dura’s attachment to the skull • 5 -15% of patients with TBI on CT have an EDH
Epidural Hematoma (EDH) • Hemorrhage “above” the dura – Usually arterial (middle meningeal artery) but can also be from venous bleeding • CT: convex (lens shaped) area of blood – Bleeding restricted by the dura’s attachment to the skull • 5 -15% of patients with TBI on CT have an EDH


 • Potentially rapidly expanding with mass effect and uncal herniation (fixed/dilated") Epidural Hematoma (EDH) • Potentially rapidly expanding with mass effect and uncal herniation (fixed/dilated pupil) – “Awake and then die” • Most EDHs can be observed • EDHs with mass effect require surgical drainage
Epidural Hematoma (EDH) • Potentially rapidly expanding with mass effect and uncal herniation (fixed/dilated pupil) – “Awake and then die” • Most EDHs can be observed • EDHs with mass effect require surgical drainage
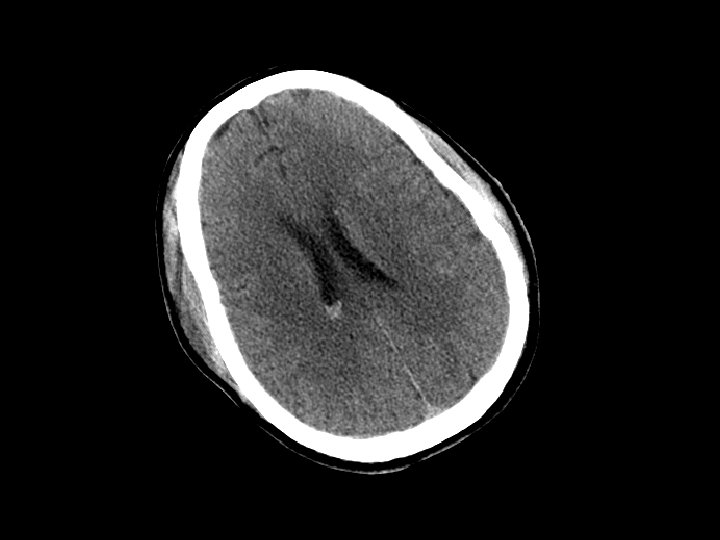
 • Hemorrhage between the dura and the brain – More common") Subdural Hematoma (SDH) • Hemorrhage between the dura and the brain – More common than EDH – 30% of patients with TBI have a SDH • CT: Crescent shaped area of blood • Can be acute, subacute or chronic – Subacute or chronic presents days/weeks after injury
Subdural Hematoma (SDH) • Hemorrhage between the dura and the brain – More common than EDH – 30% of patients with TBI have a SDH • CT: Crescent shaped area of blood • Can be acute, subacute or chronic – Subacute or chronic presents days/weeks after injury
 • Elderly at risk (less severe mechanisms) – Brain shrinks with") Subdural Hematoma (SDH) • Elderly at risk (less severe mechanisms) – Brain shrinks with age resulting in stretching of the bridging veins in the subdural space • May gradually enlarge (slower than EDH) • Surgical drainage for lesions resulting in masse effect and shift
Subdural Hematoma (SDH) • Elderly at risk (less severe mechanisms) – Brain shrinks with age resulting in stretching of the bridging veins in the subdural space • May gradually enlarge (slower than EDH) • Surgical drainage for lesions resulting in masse effect and shift


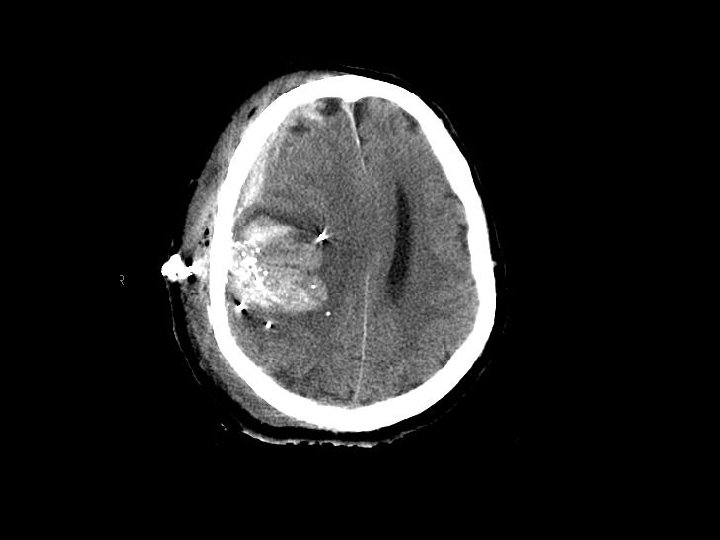
 Intracerebral Hematoma • Similar to cerebral contusions – More severe type injury – Bleeding within the brain itself • Frontal and temporal lobes • Close observation for progression of bleeding • May cause mass effect that results in herniation
Intracerebral Hematoma • Similar to cerebral contusions – More severe type injury – Bleeding within the brain itself • Frontal and temporal lobes • Close observation for progression of bleeding • May cause mass effect that results in herniation

 • Collection of blood in the ventricles • Isolated IVH usually") Intraventricular Hemorrhage (IVH) • Collection of blood in the ventricles • Isolated IVH usually not problematic and requires no specific treatment
Intraventricular Hemorrhage (IVH) • Collection of blood in the ventricles • Isolated IVH usually not problematic and requires no specific treatment
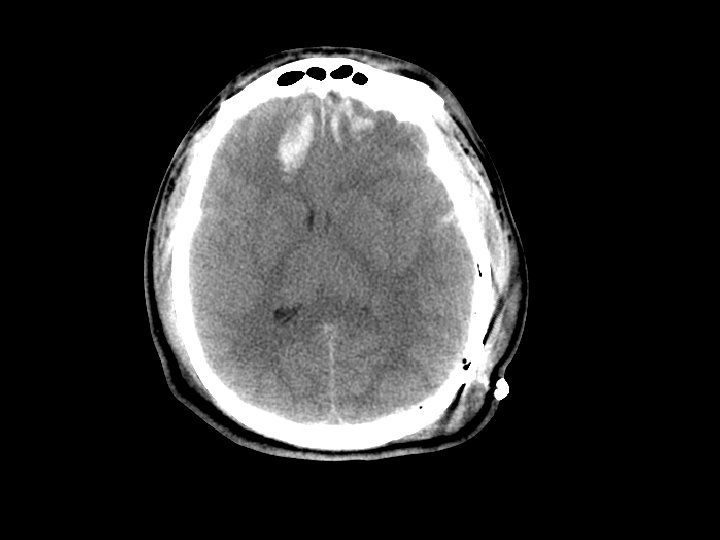
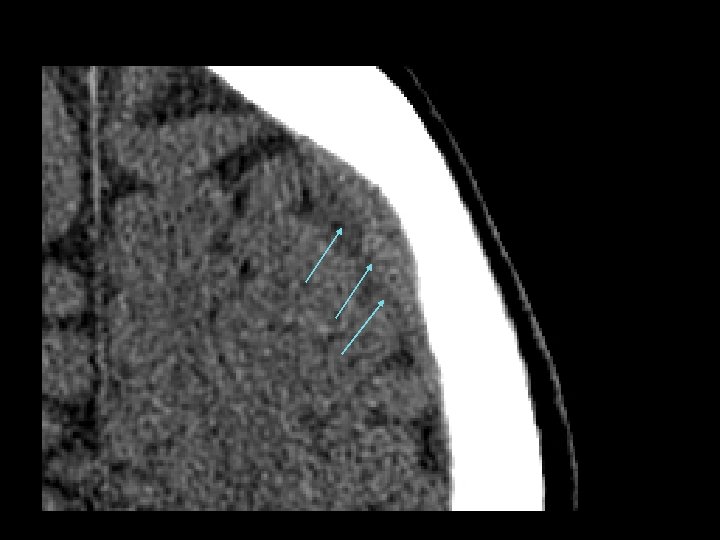
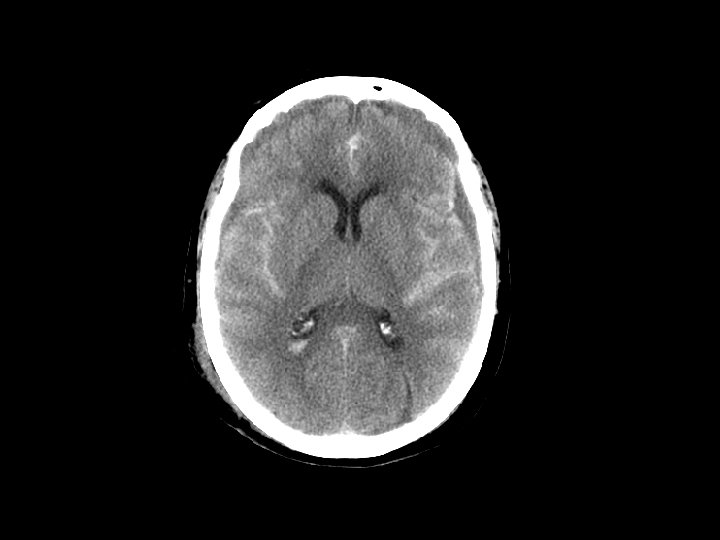
 • SAH and contusion are most common injuries on CT after") Subarrachnoid Hemorrhage (SAH) • SAH and contusion are most common injuries on CT after blunt trauma • CT: blood in the sulci and basal cisterns • Often associated with intracranial hematomas • Must consider that the SAH caused the trauma (spontaneous bleed and then fall) • Complications: – Arterial vasospasm: 2 -3 days after injury
Subarrachnoid Hemorrhage (SAH) • SAH and contusion are most common injuries on CT after blunt trauma • CT: blood in the sulci and basal cisterns • Often associated with intracranial hematomas • Must consider that the SAH caused the trauma (spontaneous bleed and then fall) • Complications: – Arterial vasospasm: 2 -3 days after injury
 • Shearing and rotational forces disrupt the axonal network •") Diffuse Axonal Injury (DAI) • Shearing and rotational forces disrupt the axonal network • Mechanism: rapid acceleration/deceleration injury • Imaging – Not well visualized by CT – MRI can better define the extent of injury • No specific therapy • Likely results in the persistent neurologic deficits in patients with normal CT scans but substantial injury
Diffuse Axonal Injury (DAI) • Shearing and rotational forces disrupt the axonal network • Mechanism: rapid acceleration/deceleration injury • Imaging – Not well visualized by CT – MRI can better define the extent of injury • No specific therapy • Likely results in the persistent neurologic deficits in patients with normal CT scans but substantial injury
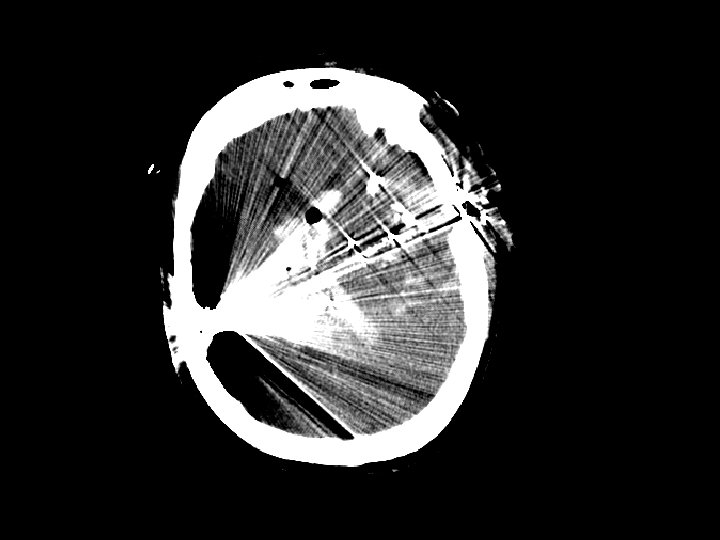
 but also from stab wounds (SWs) •") Penetrating Injury • Primarily gunshot wounds (GSWs) but also from stab wounds (SWs) • Higher rate in urban areas • Injuries that cross the midline have very poor outcomes • Periorbital/nasal region risk of infection
Penetrating Injury • Primarily gunshot wounds (GSWs) but also from stab wounds (SWs) • Higher rate in urban areas • Injuries that cross the midline have very poor outcomes • Periorbital/nasal region risk of infection
 Epidemiology of Head Injury • Varies by country, but in general: – Most common in males (ages 15 -30 years) – Highest rates of TBI on CT in: • elderly (>65 years) • young (<10 years) • Mechanisms of injury: – Motor vehicle crash (including pedestrian/bike) – Falls (especially the young and elderly) – Assaults • Alcohol frequently involved
Epidemiology of Head Injury • Varies by country, but in general: – Most common in males (ages 15 -30 years) – Highest rates of TBI on CT in: • elderly (>65 years) • young (<10 years) • Mechanisms of injury: – Motor vehicle crash (including pedestrian/bike) – Falls (especially the young and elderly) – Assaults • Alcohol frequently involved
 Classification of Neurotrauma • Multiple different classification schemes • Minimal – GCS = 15, No loss of consciousness – Normal alertness, memory and neuro exam – No evidence of skull fracture • Mild – – Brief loss of consciousness, amnesia GCS = 14 Impaired alertness, memory No evidence of skull fracture
Classification of Neurotrauma • Multiple different classification schemes • Minimal – GCS = 15, No loss of consciousness – Normal alertness, memory and neuro exam – No evidence of skull fracture • Mild – – Brief loss of consciousness, amnesia GCS = 14 Impaired alertness, memory No evidence of skull fracture
") Classification of Neurotrauma • Moderate or potentially severe – – – Prolonged (>5 minutes) loss of consciousness GCS 9 -13 Focal neurological deficit Post-traumatic seizure Intracranial lesion on CT scan Palpable depressed skull fracture • Severe: – GCS < 8 – Requires airway control
Classification of Neurotrauma • Moderate or potentially severe – – – Prolonged (>5 minutes) loss of consciousness GCS 9 -13 Focal neurological deficit Post-traumatic seizure Intracranial lesion on CT scan Palpable depressed skull fracture • Severe: – GCS < 8 – Requires airway control
 Prehospital Care • Initial GCS score • Spine immobilization • Airway management for moderate/severe head injury – Bag valve mask with oxygen to assist with ventilation – Endotracheal intubation not shown to help • Suggests harm in multiple studies
Prehospital Care • Initial GCS score • Spine immobilization • Airway management for moderate/severe head injury – Bag valve mask with oxygen to assist with ventilation – Endotracheal intubation not shown to help • Suggests harm in multiple studies
 History • Mechanism of injury – any seizure after the event? • Prehospital care – Medications given (and times) – Spine immobilization • Medical history • Allergies • Medications – Especially anticoagulant medications • Tetanus
History • Mechanism of injury – any seizure after the event? • Prehospital care – Medications given (and times) – Spine immobilization • Medical history • Allergies • Medications – Especially anticoagulant medications • Tetanus
 • Assign a GCS") Primary Survey • Standard ATLS (A, B, C, D, E) • Assign a GCS score to the patient – May use AVPU scale • Alert • Verbal stimuli • Painful stimuli • Unresponsive • Cervical spine protection • Movement in all extremities if patient to be paralyzed for airway management
Primary Survey • Standard ATLS (A, B, C, D, E) • Assign a GCS score to the patient – May use AVPU scale • Alert • Verbal stimuli • Painful stimuli • Unresponsive • Cervical spine protection • Movement in all extremities if patient to be paralyzed for airway management
 Primary Survey: Airway Managment • Most common reason for intubation in trauma • Rapid Sequence Intubation is standard in USA – Premedications • Lidocaine: 1 -2 mg/kg IV 3 -4 minutes prior, potentially protects the rise in ICP with intubation – Sedatives • Etomidate: 0. 3 mg/kg, no effects on blood pressure • Benzodiazepines/Thiopental: volume status must be normal – Paralytics • Succinylcholine: 1 -1. 5 mg/kg, paralysis for 5 minutes • Rocuronium: 1 mg/kg, paralysis for 20 -30 minutes
Primary Survey: Airway Managment • Most common reason for intubation in trauma • Rapid Sequence Intubation is standard in USA – Premedications • Lidocaine: 1 -2 mg/kg IV 3 -4 minutes prior, potentially protects the rise in ICP with intubation – Sedatives • Etomidate: 0. 3 mg/kg, no effects on blood pressure • Benzodiazepines/Thiopental: volume status must be normal – Paralytics • Succinylcholine: 1 -1. 5 mg/kg, paralysis for 5 minutes • Rocuronium: 1 mg/kg, paralysis for 20 -30 minutes
 score Standard GCS Pediatric GCS Spontaneous To Voice To Pain") Glasgow Coma Scale (GCS) score Standard GCS Pediatric GCS Spontaneous To Voice To Pain None 4 3 2 1 Verbal Response Oriented Confused Inappropriate words Incomprehensible sounds None 5 4 3 2 1 Coos/babbles Irritable/cries Cries to pain Moans None 5 4 3 2 1 Motor Response Follows commands Localizes pain Withdraws to pain Abnormal flexure posturing Abnormal extension posturing None 6 5 4 3 2 1 Spontaneous movement Withdraws to touch Withdraws to pain Abnormal flexure posturing Abnormal extension posturing None 6 5 4 3 2 1 Eye Opening
Glasgow Coma Scale (GCS) score Standard GCS Pediatric GCS Spontaneous To Voice To Pain None 4 3 2 1 Verbal Response Oriented Confused Inappropriate words Incomprehensible sounds None 5 4 3 2 1 Coos/babbles Irritable/cries Cries to pain Moans None 5 4 3 2 1 Motor Response Follows commands Localizes pain Withdraws to pain Abnormal flexure posturing Abnormal extension posturing None 6 5 4 3 2 1 Spontaneous movement Withdraws to touch Withdraws to pain Abnormal flexure posturing Abnormal extension posturing None 6 5 4 3 2 1 Eye Opening
 GCS score • Pupil examination • General neurological examination") Secondary Survey • Formal (repeat) GCS score • Pupil examination • General neurological examination – – Cranial nerves Motor exam Sensory exam Reflexes
Secondary Survey • Formal (repeat) GCS score • Pupil examination • General neurological examination – – Cranial nerves Motor exam Sensory exam Reflexes
 Secondary Survey • Head examination: – Lacerations and possible skull fracture – Evaluation for Basilar skull fracture • Hemotympanum • Raccoon’s (panda’s) eyes • Battle’s sign – mastoid ecchymosis, often takes > 12 hours to develop • CSF from the nose: – Halo test: drop of fluid onto a towel, central spot bloody with surrounding tint (CSF) – CSF contains glucose, nasal secretions do not
Secondary Survey • Head examination: – Lacerations and possible skull fracture – Evaluation for Basilar skull fracture • Hemotympanum • Raccoon’s (panda’s) eyes • Battle’s sign – mastoid ecchymosis, often takes > 12 hours to develop • CSF from the nose: – Halo test: drop of fluid onto a towel, central spot bloody with surrounding tint (CSF) – CSF contains glucose, nasal secretions do not
 Diagnostic Testing • CT scan: – – Primary screening tool Has decreased morbidity and mortality Images viewed in bone and brain windows Images rapidly obtained (<1 minute on fast CT scanners) – Exposes the patient to large amounts of radiation – Costly
Diagnostic Testing • CT scan: – – Primary screening tool Has decreased morbidity and mortality Images viewed in bone and brain windows Images rapidly obtained (<1 minute on fast CT scanners) – Exposes the patient to large amounts of radiation – Costly
 Diagnostic Testing • CT scan: – Alert patients with normal CT scans are at very low risk for neurologic deterioration • Safe to discharge home from the ED – CT limitations: • Ability to detect diffuse axonal injury • No information on blood flow to the brain
Diagnostic Testing • CT scan: – Alert patients with normal CT scans are at very low risk for neurologic deterioration • Safe to discharge home from the ED – CT limitations: • Ability to detect diffuse axonal injury • No information on blood flow to the brain
 Diagnostic Testing • Skull radiographs: – May localize a foreign body – low utility and generally not performed in those at risk for brain injury – Consider in very young children (<1 year) who appear well but only have a hematoma to head
Diagnostic Testing • Skull radiographs: – May localize a foreign body – low utility and generally not performed in those at risk for brain injury – Consider in very young children (<1 year) who appear well but only have a hematoma to head

 Diagnostic Testing • MRI: – Better than CT – May show diffuse axonal injury and injuries not identified by CT scan – Not used as a routine screening test • 30 – 45 minutes to obtain images • Very costly and not always available
Diagnostic Testing • MRI: – Better than CT – May show diffuse axonal injury and injuries not identified by CT scan – Not used as a routine screening test • 30 – 45 minutes to obtain images • Very costly and not always available
 Evaluation – Mild Head Injury • Diagnostic evaluation with cranial CT imaging when appropriate – GCS 14 -15 with LOC: • TBI on CT in 4 -15% • Neurosurgery 1 -3% • Determining appropriate indications to obtain CT is difficult – GCS = 14: patient should get a CT scan – GCS = 15: not all patients need a CT scan • Several rules to help determine when CT should be performed have been published
Evaluation – Mild Head Injury • Diagnostic evaluation with cranial CT imaging when appropriate – GCS 14 -15 with LOC: • TBI on CT in 4 -15% • Neurosurgery 1 -3% • Determining appropriate indications to obtain CT is difficult – GCS = 14: patient should get a CT scan – GCS = 15: not all patients need a CT scan • Several rules to help determine when CT should be performed have been published
 GCS = 15: Indications for CT • • Canadian Cranial CT Rule Stiell I, Lancet, 2001 New Orleans Rule Haydel, New England Journal Medicine, 2000 NEXUS Cranial CT Rule Mower W, Journal Trauma, 2005 NICE Head Injury Guidelines – http: //www. nice. org. uk/nicemedia/live/11836/36259. pdf • These rules are designed to more appropriately utilize CT in those with GCS = 15 but these rules may actually increase CT use
GCS = 15: Indications for CT • • Canadian Cranial CT Rule Stiell I, Lancet, 2001 New Orleans Rule Haydel, New England Journal Medicine, 2000 NEXUS Cranial CT Rule Mower W, Journal Trauma, 2005 NICE Head Injury Guidelines – http: //www. nice. org. uk/nicemedia/live/11836/36259. pdf • These rules are designed to more appropriately utilize CT in those with GCS = 15 but these rules may actually increase CT use
 – –") Canadian Cranial CT Rule • High Risk (to identify those needing neurosurgery) – – Failure to reach GCS=15 within 2 hours of injury Open or basilar skull fracture Vomiting more than once Age > 65 years • Moderate Risk (to identify those with brain injury on CT) – Amnesia >30 minutes before accident – High risk mechanism: auto v. ped, ejection from a motor vehicle, fall over 3 feet/5 stairs
Canadian Cranial CT Rule • High Risk (to identify those needing neurosurgery) – – Failure to reach GCS=15 within 2 hours of injury Open or basilar skull fracture Vomiting more than once Age > 65 years • Moderate Risk (to identify those with brain injury on CT) – Amnesia >30 minutes before accident – High risk mechanism: auto v. ped, ejection from a motor vehicle, fall over 3 feet/5 stairs
 New Orleans Head CT Rule • • Short-term memory deficits: 5/9 patients Intoxication: 19/176 patients Age > 60 years: 4/26 patients Seizure: 2/16 patients Headache: 4/81 patients Vomiting: 1/15 patients Above clavicle trauma: 1/197 patients
New Orleans Head CT Rule • • Short-term memory deficits: 5/9 patients Intoxication: 19/176 patients Age > 60 years: 4/26 patients Seizure: 2/16 patients Headache: 4/81 patients Vomiting: 1/15 patients Above clavicle trauma: 1/197 patients
 NEXUS Head CT Rule • Age < 65 • No evidence of skull fracture or scalp hematoma • No neurologic deficit • No abnormal alertness • No abnormal behavior • No coagulopathy • No persistent vomiting • If negative for all, then no need for CT
NEXUS Head CT Rule • Age < 65 • No evidence of skull fracture or scalp hematoma • No neurologic deficit • No abnormal alertness • No abnormal behavior • No coagulopathy • No persistent vomiting • If negative for all, then no need for CT
 NICE Head Injury Guidelines for CT • • • GCS < 13 on initial assessment GCS < 15 at 2 hours after the injury on assessment Suspected open, depressed, or basilar skull fracture Post-traumatic seizure Focal neurological deficit More than one episode of vomiting in adults Coagulopathy Amnesia for events > 30 minutes before impact Age > 65 years with loss of consciousness or amnesia Dangerous mechanism of injury (pedestrian struck by a motor vehicle, an occupant ejected from a motor vehicle or a fall from a height of greater than 1 m or five stairs) with loss of consciousness or amnesia
NICE Head Injury Guidelines for CT • • • GCS < 13 on initial assessment GCS < 15 at 2 hours after the injury on assessment Suspected open, depressed, or basilar skull fracture Post-traumatic seizure Focal neurological deficit More than one episode of vomiting in adults Coagulopathy Amnesia for events > 30 minutes before impact Age > 65 years with loss of consciousness or amnesia Dangerous mechanism of injury (pedestrian struck by a motor vehicle, an occupant ejected from a motor vehicle or a fall from a height of greater than 1 m or five stairs) with loss of consciousness or amnesia
 GCS = 15: Indications for CT • Risk factors for injury on CT from these prior studies include: – – – – Elderly: > 60 or 65 years of age Vomiting Altered Mental status/abnormal neurologic exam Skull fracture: depressed, basilar, linear LOC with symptoms (headache, nausea, etc) Post-traumatic seizure Coagulopathy (on blood thinning medications)
GCS = 15: Indications for CT • Risk factors for injury on CT from these prior studies include: – – – – Elderly: > 60 or 65 years of age Vomiting Altered Mental status/abnormal neurologic exam Skull fracture: depressed, basilar, linear LOC with symptoms (headache, nausea, etc) Post-traumatic seizure Coagulopathy (on blood thinning medications)
 GCS = 15: CT caveats • If CT is not available, consider: – Transfer to center with CT capabilities – Observation in ED or prolonged observation in hospital depending on resources
GCS = 15: CT caveats • If CT is not available, consider: – Transfer to center with CT capabilities – Observation in ED or prolonged observation in hospital depending on resources
 Pediatric: Indications for CT • Children different than adults in many aspects • Indications for cranial CT in children different than adults • Risk of radiation from the CT scan is greatest in children • Recent large pediatric study to evaluate indications for cranial CT in children – 42, 412 children with GCS = 14 -15 – Kuppermann, Lancet; 2009; 374: 1160
Pediatric: Indications for CT • Children different than adults in many aspects • Indications for cranial CT in children different than adults • Risk of radiation from the CT scan is greatest in children • Recent large pediatric study to evaluate indications for cranial CT in children – 42, 412 children with GCS = 14 -15 – Kuppermann, Lancet; 2009; 374: 1160
 Suggested CT algorithm for patients >2 years old with GCS 14 -15 after head trauma GCS = 14 or other signs of altered mental status, or Palpable skull fracture No Yes 14. 0% of population 4. 3% risk of clinically important TBI Yes History of LOC, or vomiting, or Severe mechanism of injury, or Severe Headache No 27. 7% of population 0. 9% risk of Clinically important TBI 58. 3% of population <0. 05% risk of clinically important TBI CT not recommended CT recommended Observation vs. CT: based on clinical factors including: Physician experience Multiple versus isolated findings Worsening symptoms or signs after ED observation Parental preference
Suggested CT algorithm for patients >2 years old with GCS 14 -15 after head trauma GCS = 14 or other signs of altered mental status, or Palpable skull fracture No Yes 14. 0% of population 4. 3% risk of clinically important TBI Yes History of LOC, or vomiting, or Severe mechanism of injury, or Severe Headache No 27. 7% of population 0. 9% risk of Clinically important TBI 58. 3% of population <0. 05% risk of clinically important TBI CT not recommended CT recommended Observation vs. CT: based on clinical factors including: Physician experience Multiple versus isolated findings Worsening symptoms or signs after ED observation Parental preference
 Suggested CT algorithm for patients <2 years old with GCS 14 -15 after head trauma GCS = 14 or other signs of altered mental status, or Palpable skull fracture No Yes 13. 9% of population 4. 4% risk of clinically important TBI Yes Occipital/parietal/temporal scalp hematoma, or History of LOC > 5 sec, or Severe mechanism of injury, or Not acting normally per parent No 32. 6% of population 0. 9% risk of Clinically important TBI 53. 5% of population <0. 02% risk of clinically important TBI CT not recommended CT recommended Observation vs. CT: based on clinical factors including: Physician experience Multiple versus isolated findings Worsening symptoms or signs after ED observation Age < 3 months Parental preference
Suggested CT algorithm for patients <2 years old with GCS 14 -15 after head trauma GCS = 14 or other signs of altered mental status, or Palpable skull fracture No Yes 13. 9% of population 4. 4% risk of clinically important TBI Yes Occipital/parietal/temporal scalp hematoma, or History of LOC > 5 sec, or Severe mechanism of injury, or Not acting normally per parent No 32. 6% of population 0. 9% risk of Clinically important TBI 53. 5% of population <0. 02% risk of clinically important TBI CT not recommended CT recommended Observation vs. CT: based on clinical factors including: Physician experience Multiple versus isolated findings Worsening symptoms or signs after ED observation Age < 3 months Parental preference
 Treatment of Mild Head Injury • Safe to discharge patients with normal cranial CT scans to home: – Adults (Livingston, Ann Surg 2000) • 2, 152 adults with normal CT • One patient had a craniotomy for skull fracture noted on initial CT scan • NPV for craniotomy = 99. 94% – Pediatrics (Holmes, AEM 2010) • 13, 543 children with normal CT • None underwent craniotomy • NPV for craniotomy = 100%
Treatment of Mild Head Injury • Safe to discharge patients with normal cranial CT scans to home: – Adults (Livingston, Ann Surg 2000) • 2, 152 adults with normal CT • One patient had a craniotomy for skull fracture noted on initial CT scan • NPV for craniotomy = 99. 94% – Pediatrics (Holmes, AEM 2010) • 13, 543 children with normal CT • None underwent craniotomy • NPV for craniotomy = 100%
 Treatment of Mild Head Injury • Appropriate discharge instructions • Warnings regarding concussion symptoms – Explanation of post-concussive symptoms – Exclusion from activity that may result in a repeat head injury (i. e. sports) • Headaches: paracetamol, aspirin • Nausea/Vomit: antiemetics
Treatment of Mild Head Injury • Appropriate discharge instructions • Warnings regarding concussion symptoms – Explanation of post-concussive symptoms – Exclusion from activity that may result in a repeat head injury (i. e. sports) • Headaches: paracetamol, aspirin • Nausea/Vomit: antiemetics
 Moderate/Severe Head Injury
Moderate/Severe Head Injury
 Initial Evaluation of Moderate/Severe Head Injury • A, B, C, D, E – Airway control for GCS < 8 – Prevent hypotension and Hypoxia • Hypotension: triples risk of death • Hypoxia: doubles risk of death • Movement in all extremities prior to paralysis if possible • If comatose, assess brainstem function: – Corneal reflex: lightly touch cornea will result in blinking (Cranial Nerves V and VII)
Initial Evaluation of Moderate/Severe Head Injury • A, B, C, D, E – Airway control for GCS < 8 – Prevent hypotension and Hypoxia • Hypotension: triples risk of death • Hypoxia: doubles risk of death • Movement in all extremities prior to paralysis if possible • If comatose, assess brainstem function: – Corneal reflex: lightly touch cornea will result in blinking (Cranial Nerves V and VII)
 Initial Evaluation of Moderate/Severe Head Injury • GCS ≤ 13 • Immediate CT scan (if stable) • If no CT available, then consult with neurosurgeon and transfer to site with CT • Include cervical spine imaging: CT of the cervical spine recommended the lower the GCS score is
Initial Evaluation of Moderate/Severe Head Injury • GCS ≤ 13 • Immediate CT scan (if stable) • If no CT available, then consult with neurosurgeon and transfer to site with CT • Include cervical spine imaging: CT of the cervical spine recommended the lower the GCS score is
 Treatment of Moderate/Severe Head Injury • Maintain CPP and the patient’s airway – treat hypoxia and hypotension immediately • Intracranial pressure monitoring in those with GCS < 8 – Although no evidence outcome is improved – Can be performed in the ED but normally in the operating suite by a neurosurgeon • Elevate head of bed (30 ) if no cervical spine injury
Treatment of Moderate/Severe Head Injury • Maintain CPP and the patient’s airway – treat hypoxia and hypotension immediately • Intracranial pressure monitoring in those with GCS < 8 – Although no evidence outcome is improved – Can be performed in the ED but normally in the operating suite by a neurosurgeon • Elevate head of bed (30 ) if no cervical spine injury
 Treatment of Moderate/Severe Head Injury • Mannitol – Increases mean arterial pressure and lowers ICP – Patient must be stable • Do not give if volume depleted as it may result in hypotension – Maintain volume status – Keep serum osmolarity < 320 mmol/L
Treatment of Moderate/Severe Head Injury • Mannitol – Increases mean arterial pressure and lowers ICP – Patient must be stable • Do not give if volume depleted as it may result in hypotension – Maintain volume status – Keep serum osmolarity < 320 mmol/L
 Treatment of Moderate/Severe Head Injury • Mannitol – 0. 5 – 1 gram/kg IV bolus • Repeat boluses better than drip – Indications • increased ICP: once ICP monitor placed • Give in ED: – signs of transtentorial herniation – progressive neurological deterioration
Treatment of Moderate/Severe Head Injury • Mannitol – 0. 5 – 1 gram/kg IV bolus • Repeat boluses better than drip – Indications • increased ICP: once ICP monitor placed • Give in ED: – signs of transtentorial herniation – progressive neurological deterioration
 Treatment of Moderate/Severe Head Injury • Anticonvulsants – Used for the first 7 days after injury in patients with high risk TBI: • GCS<10, CT with contusion, hematoma, or depressed skull fracture, Seizure • No evidence for anticonvulsants beyond 7 days – Phenytoin 15– 18 mg/kg IV • Carbamezapine and kepra also used – Acute seizure: • Standard therapy: – oxygen – Benzodiazepines, phenytoin, barbituates
Treatment of Moderate/Severe Head Injury • Anticonvulsants – Used for the first 7 days after injury in patients with high risk TBI: • GCS<10, CT with contusion, hematoma, or depressed skull fracture, Seizure • No evidence for anticonvulsants beyond 7 days – Phenytoin 15– 18 mg/kg IV • Carbamezapine and kepra also used – Acute seizure: • Standard therapy: – oxygen – Benzodiazepines, phenytoin, barbituates
 Treatment of Moderate/Severe Head Injury • Sedation and Pain control – Intubated patients require sedation to prevent elevation of ICP (fighting the ventilator) – Sedation must be balanced with the need for repeat neurologic examinations to determine if brain injury is worsening – Pain control: • Fentanyl ideal narcotic in TBI patients – Sedation: • Propofol: used with increasing frequency in TBI patients • Benzodiazepines: • Barbiturates: high doses in those with uncontrollable ICP
Treatment of Moderate/Severe Head Injury • Sedation and Pain control – Intubated patients require sedation to prevent elevation of ICP (fighting the ventilator) – Sedation must be balanced with the need for repeat neurologic examinations to determine if brain injury is worsening – Pain control: • Fentanyl ideal narcotic in TBI patients – Sedation: • Propofol: used with increasing frequency in TBI patients • Benzodiazepines: • Barbiturates: high doses in those with uncontrollable ICP
 Treatment of Moderate/Severe Head Injury • Surgical therapy – Craniotomy • Treatment of choice for correctable mass lesions • Better outcomes with no delays to surgery • Large hematomas (with shift), depressed skull fractures, penetrating injuries (debride the wound) – Intracranial pressure monitors/ventriculosotmy • Monitor pressure and drain CSF
Treatment of Moderate/Severe Head Injury • Surgical therapy – Craniotomy • Treatment of choice for correctable mass lesions • Better outcomes with no delays to surgery • Large hematomas (with shift), depressed skull fractures, penetrating injuries (debride the wound) – Intracranial pressure monitors/ventriculosotmy • Monitor pressure and drain CSF
 Treatment of Moderate/Severe Head Injury • Emergency Burr Hole – Indicated in patients with rapid neurologic deterioration and an expanding hematoma and unable to get to a neurosurgeon – Other measures to reduce ICP should be attempted prior to this procedure – Burr hole performed on side of dilated pupil at the temporal bone – MD must be familiar with technique prior to attempting
Treatment of Moderate/Severe Head Injury • Emergency Burr Hole – Indicated in patients with rapid neurologic deterioration and an expanding hematoma and unable to get to a neurosurgeon – Other measures to reduce ICP should be attempted prior to this procedure – Burr hole performed on side of dilated pupil at the temporal bone – MD must be familiar with technique prior to attempting
 Treatment of Moderate/Severe Head Injury • Hyperventilation – Previously a standard treatment in those with TBI – Now known to be harmful • Worse outcomes in those with prophylactic hyperventilation (Muizelaar, J Neurosurg 1991) – No prophylactic hyperventilation – Goal p. CO 2: ~ 35 mm. Hg • Do not let p. CO 2 get below 30 mm. Hg
Treatment of Moderate/Severe Head Injury • Hyperventilation – Previously a standard treatment in those with TBI – Now known to be harmful • Worse outcomes in those with prophylactic hyperventilation (Muizelaar, J Neurosurg 1991) – No prophylactic hyperventilation – Goal p. CO 2: ~ 35 mm. Hg • Do not let p. CO 2 get below 30 mm. Hg
 Treatment of Moderate/Severe Head Injury • Hyperventilation – Do not hyperventilate during initial 24 hours after injury – Hyperventilate for brief periods when there is acute neurologic deterioration – Hyperventilate for ICP that is refractory to sedation, paralysis, cerebral spinal fluid drainage, and osmotic diuretics • This is one of the last therapies
Treatment of Moderate/Severe Head Injury • Hyperventilation – Do not hyperventilate during initial 24 hours after injury – Hyperventilate for brief periods when there is acute neurologic deterioration – Hyperventilate for ICP that is refractory to sedation, paralysis, cerebral spinal fluid drainage, and osmotic diuretics • This is one of the last therapies
 Treatment of Moderate/Severe Head Injury • Antibiotics – Basilar skull fracture – no evidence that prophylactic antibiotics are beneficial – Open fractures • Controversial, little evidence to support • Antibiotics to cover skin flora
Treatment of Moderate/Severe Head Injury • Antibiotics – Basilar skull fracture – no evidence that prophylactic antibiotics are beneficial – Open fractures • Controversial, little evidence to support • Antibiotics to cover skin flora
 Treatment of Moderate/Severe Head Injury • Corticosteroids – Believed to decrease cerebral edema – CRASH trial (Roberts, Lancet 2004; 364: 1321) • 10, 008 adults in a randomized controlled trial – Increased risk of death with steroids • Relative risk = 1. 18 (95% CI 1. 09, 1. 27) – No longer recommended in patients with traumatic brain injury
Treatment of Moderate/Severe Head Injury • Corticosteroids – Believed to decrease cerebral edema – CRASH trial (Roberts, Lancet 2004; 364: 1321) • 10, 008 adults in a randomized controlled trial – Increased risk of death with steroids • Relative risk = 1. 18 (95% CI 1. 09, 1. 27) – No longer recommended in patients with traumatic brain injury
 Treatment of Moderate/Severe Head Injury • Hypertonic saline – No benefit in 2 large randomized controlled trials • Hypothermia – Experimental in those with isolated head injury – No good clinical evidence that it is useful • Albumin – Unlikely to be beneficial and generally not recommended • Progesterone – Promising in several small studies • Wright, Ann Emerg Med 2007; 49: 391 – Large trial ongoing in the USA
Treatment of Moderate/Severe Head Injury • Hypertonic saline – No benefit in 2 large randomized controlled trials • Hypothermia – Experimental in those with isolated head injury – No good clinical evidence that it is useful • Albumin – Unlikely to be beneficial and generally not recommended • Progesterone – Promising in several small studies • Wright, Ann Emerg Med 2007; 49: 391 – Large trial ongoing in the USA
 Points to remember • Avoid hypoxemia and hypotension in the TBI patient • Airway controlled if GCS ≤ 8 • Avoid hyperventilation – keep p. CO 2 from 35 -40 mm. Hg • Mannitol for evidence of brain herniation or neurologic deterioration • Anticonvulsants for those at risk of posttraumatic seizures • Avoid delays to the OR for those patients needing craniotomy
Points to remember • Avoid hypoxemia and hypotension in the TBI patient • Airway controlled if GCS ≤ 8 • Avoid hyperventilation – keep p. CO 2 from 35 -40 mm. Hg • Mannitol for evidence of brain herniation or neurologic deterioration • Anticonvulsants for those at risk of posttraumatic seizures • Avoid delays to the OR for those patients needing craniotomy
 Points to remember • Depressed mental status may be due to brain injury in the intoxicated patient • CT scanning is the screening test of choice but is not necessary in all patients with minor head injury • Patients with normal cranial CT scans are at low risk for deterioration and may be discharged from the ED if otherwise stable
Points to remember • Depressed mental status may be due to brain injury in the intoxicated patient • CT scanning is the screening test of choice but is not necessary in all patients with minor head injury • Patients with normal cranial CT scans are at low risk for deterioration and may be discharged from the ED if otherwise stable