a363447919d1ab69aa90730a97c0766b.ppt
- Количество слайдов: 140


")
Neurologic Complications of Systemic Disease October 3 rd 2012 Robert Altman MD FRCP(C)

Objectives • Highlight “key points” in selected topics overlapping between neurology and internal medicine (Dx and Tx) – Neurologic complications of systemic diseases • Appreciate “common presentations” of the diseases seen in Internal Medicine / Rheumatology clinics or in consultation – Emphasis on multi-media, neuroimaging and clinical reasoning through 12 clinical vignettes. • Will not touch upon the “approach to” medicine. Nonetheless important and should related complications in neurologic patients not ignore. . . part of RC objectives; – Should have been covered in PGY 1, please refer to www. uptodate. com sick medical patient managing

“Neurological Borderlands” • Studying the impact of systemic diseases on the nervous system allows for – Consolidating knowledge of neuroanatomy, medicine, immunology and clinical examination skills. Lateral thinking. – Forming cognitive cross-links and appreciating the complexities in the diagnosis and management of the medically “sick” patient. – Having an organized ‘approach to’ very challenging cases facilitates the diagnostic process – Having a broader appreciation of neuropharmacology and systemic interactions – Understand the lack of evidence based therapies or guidelines in overlap cases because (a) rare entities (b) different specialists often involved in complex patient care; each have different approaches or association guidelines (c) No-one “takes ownership” of these cases – Educating or facilitating transfer of knowledge to colleagues in medicine, psychiatry and neurology

References Bradley Continuum x 2 Royal College notes Up to Date NEJM (Images in Clinical Medicine – videos) • Selected review papers: see last slide • • • February 2011 February 2008

Pre-Test • Neurologic manifestations of celiac disease is primarily related to specific vitamin deficiency state(s) T/F • The CNS is the second most common system involved in sarcoid (outside of pulmonary) T/F • Most sensitive biomarker for neurosarcoid is CSF ACE level T/F • Phenytoin is contraindicated in a liver failure patient T/F • Name a purported biomarker that indicates active neuropsychiatric SLE. • SS is one of the classic syndromes associated with sensory neuronopathy T/F • It is safe to use Remicade for RA in a patient with concomitant RRMS T/F

Outline 1. Neurologic Complications of Hepatic Failure – Hepatic encephalopathy, cirhosis and ALF 2. Alcohol and the nervous system 3. Neurogastroenterology – Mini-review of a few ultra-precise topics 4. Neurologic Complications of Renal Failure 5. Systemic Inflammatory Diseases – – Sarcoid Sjögren’s Syndrome RA SLE

CASE 1 Clinical Scenario 1 • Which of the following is more common in patients with hepatic encephalopathy in the setting of ALF than in patients with HE from cirrhosis? 1. 2. 3. 4. 5. Asterixis Bradykinesia Dysarthria Seizures Somnolence

CASE 1 Clinical Scenario 1 • Which of the following is more common in patients with hepatic encephalopathy in the setting of ALF than in patients with HE from cirrhosis? 1. 2. 3. 4. 5. Asterixis Bradykinesia Dysarthria Seizures Somnolence

Neurologic Manifestations of Hepatic Failure / ALF

Clinical Clues • Background knowledge of stigmata of chronic liver disease may help when diagnosis is ambiguous

Hepatic Failure • Encephalopathy – Unique • Rigidity *, tremor and hypokinesia (even if asymptomatic in initial stages) • Asterixis in UE’s or LE’s http: //www. nejm. org/doi/full/10. 1056/NEJMicm 0911157

Altered LOC in Liver Patient “Don’t do something, just stand there. . . ” • Ddx – Hypoglycemia – Sodium disturbance – Epileptic – Cerebral edema – Hypoxia (unwitnessed cardiac or pulmonary arrest) • Intoxication or OD – Wernike – ICH (coagulopathic)

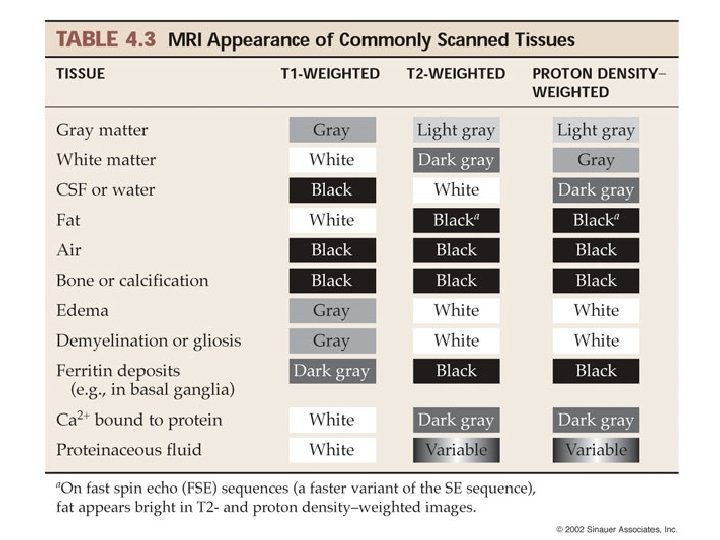
Pallidal hyperintensities on T 1 Reflects a significant portosystemic shunt, NOT hepatic encephalopathy Mn deposition (reduced excretion in bile) 90% of patients

Hypoglycemic Coma MR DWI is key sequence NB. Study excluded cardiac / respiratory arrest AJNR Am J Neuroradiology May 2012

CPM: note DWI + and location

Pathophysiology • Porto-systemic shunt with toxins normally filtered by liver gaining direct access to circulation / CNS • Main players – Ammonia • Astrocyte swelling (osmotic mechanisms) • Increased ROS – As no urea synthesis in CNS; glutamine synthesis occurs • Astrocytic swelling • Dysfunction of astrocytic and neuronal function (neurotransmission) • Increased expression of benzodiazepine receptors, augmenting GABAa receptors

Hepatic Failure / Disease Grade II • Asterixis • Brady • Rigidity • Tremor • Cerebellar dysarthria • Ataxia II

Ammonia • Elevated levels point to “potential hepatic in origin” to change in brain function • Serum levels corroborate broadly with stages of encephalopathy – Substantial overlap exists (stages) • Normal ammonia does NOT rule out HE – So check it. – And trend it. • Include it in a full metabolic panel when investigating any “encephalopathy”
 1. Look for")
Practical Point Principals of Management of Hepatic Encephalopathy (acute and chronic) 1. Look for source (occult bleed) 2. Low protein in diet 3. Lactulose PO or enema; titrate to 3+ soft BM per day 4. Antiobiotics – Target urea producing bacteria in gut (Neomycin) 5. Avoid benzodiazepines (heightened sensitivity); if necessary try Oxazepam. – May need Flumazenil. 6. ICP management. Propofol, hypertonics. 7. Consider porto-systemic shunting procedure (TIPPS) 8. Liver transplant (committee)

CASE 1. 5 36 F overdose on acetaminophen Describe the pertinent findings.
 • Encephalopathy (irritability, insomnia, concentration deficits, disorientation) + – Cerebral")
Acute Liver Failure (ALF) • Encephalopathy (irritability, insomnia, concentration deficits, disorientation) + – Cerebral edema – Seizures • Generally grades III and IV • ICP monitoring with subdural transducers can be used • Tend to occur with NH 4 > 124µmol/L • ICP management – HV, osmotics (watch-out for RF), propofol, targeted natremia (145155 mmol/L) • Seizure control – Controlled trial with prophylactic phenytoin (no survival advantage, but does decrease subclinical seizures and edema) – Appropriate sedation; barbituates, propofol careful use of benzos (midazolam)
 • Sine qua non is presence of elevated")
Practical Point “Idopathic Recurrent Stupor” (endozepine-4) • Sine qua non is presence of elevated serum (and CSF) endozepine – Physiologically regulated by neurons – Function; Modulate GABA-mediated neurotransmission • Interictally, the patients have normal EEG findings. During the attacks there is diffuse, low-amplitude, unreactive beta rhythm (13– 16 Hz). • Administration of intravenous flumazenil, 0. 5 to 2 mg or more, reverses the abnormal EEG pattern to normal, reactive alpha rhythm, and correlates with clinical improvement Ref: Metabolic Encephalopathies – Clinics 2011
, 121, 127– 133")
Brain (1998), 121, 127– 133

CASE 2 Quickie – A Neurological Classic • 33 M • Anorexia Nervosa • Otherwise no other Pm. Hx • Admitted to psychiatry with severe hypokalemia and bradycardia • Neuro consult; – “please assess” – “r/o organic brain”

CASE 2 Accompanying MR Brain

Practical Point Wernicke’s Encephalopathy • W-A-C-O – Wernike • Ataxia • Confusion / confabulation • Ophthalmoplgia • Clinical Pearls – Appreciate that it occurs outside of ETOH abuse and represents a manifestation of malnourished state – Also that all features need not be present simultaneously – Vitamin deficiency* Which? – Know the treatment for it

Practical Point Wernike’s in Pregnancy Note Ddx Molar pregnancy Hyper. T 4 Hepatitis • Generally from hyperemesis graviderum • 6 -16 weeks • Tx with thiamine IV until able to handle PO (UTD. com) – 500 mg IV TID x 2, then 500 mg daily IV/IM QD x 5 • Daily oral administration of 100 mg of thiamine should be continued after the completion of parenteral treatment and after discharge from the hospital until patients are no longer considered at risk. • Magnesium and other vitamins are replaced as well, along with other nutritional deficits if present

Neurologic Manifestations of GI Disease

CASE 3 35 F, appendicular ataxia on exam. Gets bloated and has diarrhea when eating rye or wheat. Also noted distal stocking glove polyneuropathy on exam. • Sent to see you from GI for opinion Normal comparison
 • Chronic immune-mediated systemic disease with diverse manifestations including; GI, dermatopathy,")
Gluten Enteropathy (Celiac) • Chronic immune-mediated systemic disease with diverse manifestations including; GI, dermatopathy, neurologic dysfunction – Diagnosis (in predisposed pt’s) – Serum markers + – Ig. A t. TG serology or Anti-Endomysium Ab (Ig. A EMA) or [Anti-gliadin Ig. G, ig. A [markers for spectrum of dz] ] – Small intestine bx • Earliest markers are TTG (Ig. A), anti-gliadin which can be present even before gut involved – It is said t. TG implies gut (specific) • Can get neurologic involvement without gut
 • Neurologic effects not vitamin deficiency states, rather immune mediated. –")
Gluten Enteropathy (celiac) • Neurologic effects not vitamin deficiency states, rather immune mediated. – Ig. A + TTG deposits in vessels in brainstem, cerebellum, small bowel mucosa, peripheral nerves, muscles – Cross reactivity with Purkinje cells with atrophy and gliosis • Effects entire neuraxis – Central (brain, cerebellum (gluten ataxia), cord) – Peripheral (‘gluten’ neuropathy, ‘inflammatory’ myopathy) • Treatment – Eliminate gluten (B-R-O-W) completely – ? immunosuppression if despite strict adherence to diet and dropping Ab levels neurologic dysfunction continues to progress • CONTROVERSIAL
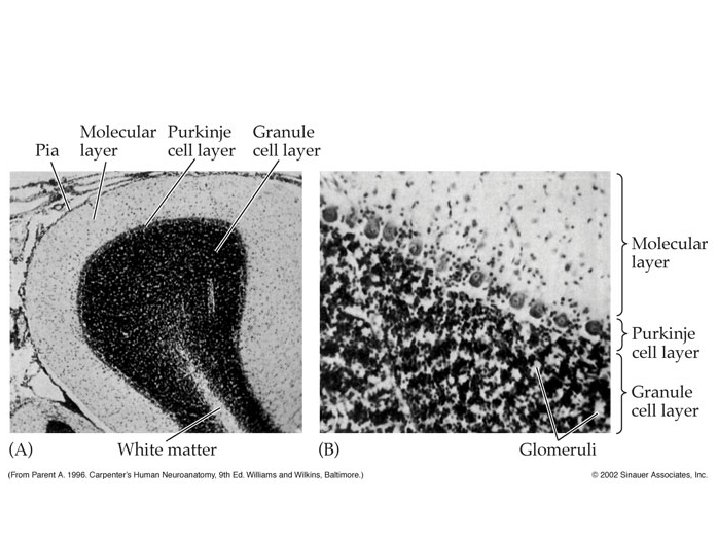

Perivascular inflammatroy infiltrate Perivascular Tg Serum from patients with gluten ataxia reacts with Purkinje cell epitopes Purkinje loss
 1.")
Practical Point Name 5 auto-immune or immune mediated diseases (systemic or nervous system) 1. 2. 3. 4. 5. MG MS / ADEM GBS Dermatomyositis / polymyositis Devic’s disease (neuromyelitis optica) 6. Neuropsychiatric lupus 7. Rhumatoid arthritis 8. Sleroderma 9. Sjogren 10. Paraneoplastic syndromes +++ (NMDA-R encephalitis, SPS) 11. Thyroid eye disease (Graves) or Hashimotos’ (SREAT) 1. 2. 3. 4. 5. Vitiligo DM 1 Psoriasis Celiac disease (ataxia, neuropathy) IBD

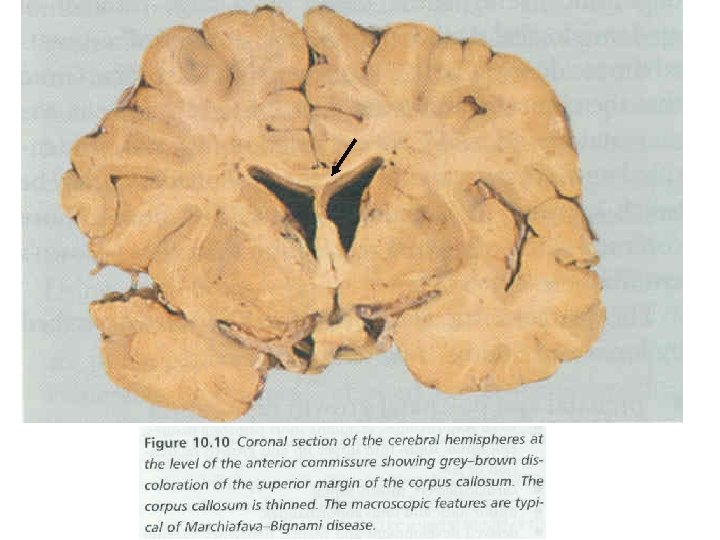
CASE 4 Mr. F, 63 M stumbles into JGH ER. “confused and ataxic” according to ED. Automatic neuro consult. • CT brain; NIL ACUTE. • ETOH level 120 mmol/L, i. e, drunk • 23: 30; Unfortunately code white called on bed 12 red A – Psych pt escaped and stabbed the security guard – Mr F has an unwitnessed ‘hallway’ MI out of fear and dies. • Brain autopsy results shown

Describe the most pertinent findings. . .

Neurologic Manifestations of ETOH Toxicity

ETOH and the nervous system
 •")
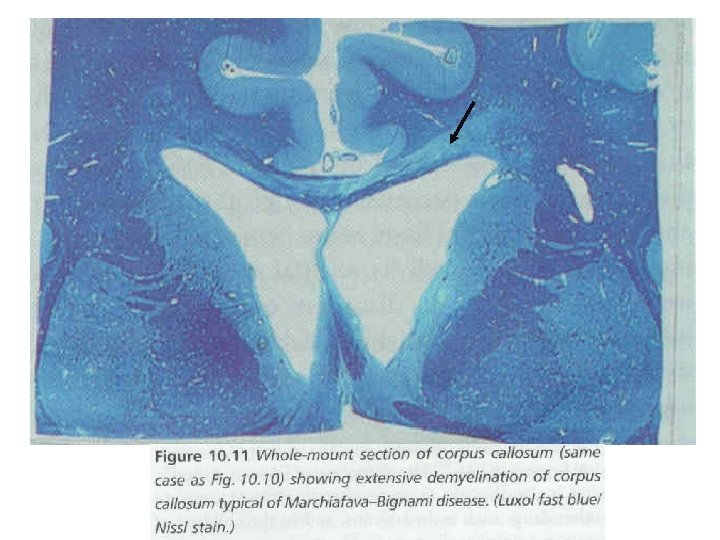
Practical Point Every Level of the Neuraxis • Acute intox (i. e, drunk) • Alcohol – Tobacco Amblyopia • Alcoholic Dementia • Cerebellar degeneration • Marchiafava Bignami or CPM (Na shifts) – “Vermian man” • Wernike-Korsakoff • Polyneuropathy (toxic and malnutrition) • Myopathy • Epileptic (withdrawal or DT’s) You may very well see all in the same patient. . .
 – Helpful in assessing compliance")
Because you asked. . . • Antigliadin antibodies (AGA) – Helpful in assessing compliance to low gluten diet (antibody to breakdown-product of gluten: gliadin), but very poor sensitivity and specificity • Ig. A AGA a sensitivity of 75– 95% and a specificity of 80– 90% • Ig. G AGA a sensitivity of 17– 100% (wide variation between studies) and a specificity of 70– 80%. • Ig. A EMA and Ig. A t. TG are based on the target antigen t. TG – Ig. A EMA had a sensitivity of 90– 97% and specificity close to 100%; – Ig. A t. TG a sensitivity of 90– 98% and specificity between 95 – 99%;

Neurologic Manifestations of Renal Disease 5 -16% incidence of ARF in hospitalized patients Mortality 20 -51%
 Progressive")
CASE 5 Clinical Example • • 52 M HTN, DB 2, CKD (CRF) Progressive lethargy, confusion, and tremors Minimal PO intake x 2 -3 days Found down by wife, with urinary incontinence and rhythmic jerking movements of the extremities

CASE 5 • On exam – 176/100 mm Hg – Bibasilar crackles on lung examination and 2+ pitting edema in the lower extremities – EO briefly to a loud voice but unable to follow complex commands. • Able to state name, and speech dysarthric. • Unable to correctly state the year or the month. • Not at his baseline according to family. – Myoclonus in arms / legs §Normal neuroimaging (not shown) – Bilateral asterixis – Labs: Creat 864 umol/L, K 5. 1, Hb 82 What is the next most important test in this patient’s management?

Important to differentiate NCS from Uremic Encephalopathy; very different treatments. . .
")
Neurologic Complications 1. Manifestations of uremic state 2. Consequence of renal replacement therapy (dialysis) • • Combination of the above CNS, PNS or both • Most complications fail to resolve fully with dialysis or transplantation (and may develop or worsen)

Disease Related • • Encephalopathy Cognitive impairment and Dementia Cerebrovascular Movement Disorders Focal mononeuropathies Polyneuropathies Uremic Myopathy Nephrogenic Systemic Sclerosis

Disease Related • Encephalopathy – ARF or CRF – Fluctuating LOC, disorientation, attention, concentration, sleep, h/a, asterixis, myoclonus, sz, UMN signs • Uremic; neurotoxins • E+ derangement; hyper. Ca, Mg; hypo. PO 4, Na • Metabolic acidosis • Wernike’s • Hypertensive; PRES • Vascular event; SDH or SAH [low threshold to image] • Rx
 • Rx • e.")
? Disease Related • Ddx Encephalopathy in renal patient (cont) • Rx • e. g. , metoclopramide, phenothiazines, AEDs including gabapentin, and opioids meperidine • Bottom Line • Before concluding encephalopathy to be a clinical feature of advanced uremia requiring renal replacement therapy, a careful search for other causes should be initiated Correction of the underlying metabolic abnormality typically leads to resolution of symptoms

Disease Related • Cognitive impairment +/- Dementia – 80% in those with CRF – Memory and executive dysfunction – Multifactorial • • • Subclinical vascular cognitive impairment (same RF’s) Inflammatory mediators Anemia and relative hypoxia-emia EPO Hyperparathyroidism (Hyper. Ca) Cognition may improve after transplant; memory, concentration, psychomotor function, EEG/EP latencies

Disease Related • Cerebrovascular – Ischemic and hemorrhagic • 4 -10 X risk compared to N controls – Ischemia • ASO, CRF share common RFs – DB, HTN, DLPD, smoking, ↑homocysteine – Anemia (independent RF for CVA) – Hemorrhage – – Plt dysfunction (poor aggregability) HTN PCKD (10 X risk for aneurysms and dolichoectasia) Antithrombotic agents used in HD to prevent fistulathrombosis (heparin)

Disease Related • Movement Disorders – Action myoclonus – Stimulus-sensitive myoclonus – “twitch convulsive syndrome” intense asterixis and myoclonus accompanied by fasciculations, muscle twitching and seizures – RLS 15 -20% • Secondary to the renal disease, anemia +/- peripheral neuropathy All improve once metabolic disturbance under control or posttransplant

Disease Related • Focal mononeuropathies – Susceptible to compression and ischemia in renal patients • Median, ulnar (UNE, UNW-from calcinosis), femoral – Vascular “steal” phenomenon after fistula insertion • Polyneuropathies – – “Uremic neurotoxins” 60% pt’s Large and small fiber (including autonomic), cranial May stabilize, even improve in dialysis (esp paresthesiae) • Uremic Myopathy – 50% of pt’s on dialysis – “uremic toxins, vitamin D metabolism dysfunction, insulin resistence, carnitine deficieny, malnutrition” all contribute] – Bx is normal or type II atrophy – Some improvement post-transplant
 Features Uremic myopathy possible Parallels decline")
Neuromuscular Complications Proportionate to GFR <25 ml/min (myopathy) Features Uremic myopathy possible Parallels decline in renal function <12 ml/min (polyneuropathy) Clinical symptoms being “myopathic” weakness; with wasting, poor endurance, and rapid fatiguing Normal EMG / Bx (type II) NCS abnormalities <6 ml/min (polyneuropathy) Clinical P&N, heat, autonmoic failure, sensory loss, areflexia Pruritus

Nephrogenic Systemic Sclerosis • ARF or CRF • Within 2 months of exposure to G+Gadolinium-based contrast agents are contraindicated in patients • Severe pain, tightening, on dialysis, and use of these agents burning of skin associated with a GFR < 30 with MRI in patients with redness and swelling. be avoided. m. L/min should – Ultimately, joint contractures and limited mobility

Treatment Related • • • Dialysis dysequilibrium syndrome Dialysis dementia EPO-related Rejection encephalopathy Anti-rejection Rx related PRES

Treatment Related • “Dialysis dysequilibrium syndrome” – Rapid clearance of BUN / other osmotically active solutes Now considered a “non-issue, ” as modern day dialysis takes rates and • Nausea, vomiting, restlessness, cramps, confusion contents of dialysate into account. – Easily avoided slowing rates of dialysis, using smaller dialysate volumes and more frequent Nonetheless, errors do occur and sessions should be cognizant of it. • “Dialysis dementia” – Aluminum accumulation of GM • Dysarthria, language disturbance, apraxia, personality, psychosis, myoclonus, seizures and dementia.
 – 1/3 pt’s get HTN and can manifest")
Treatment Related • EPO-related (for CKD) – 1/3 pt’s get HTN and can manifest with PRES – Careful monitoring of BP when initiating therapy and slow uptitration of dose • Anti-rejection Rx related – PRES and HTN // multifactorial BBB disruption, demyelination and endothelial damage • Cyclosporine, tacrolimus • Rejection encephalopathy – Within 3 months (up to 2 yrs) of transplantation – Cytokine induced (hypothesis) – Complete recovery after Tx rejection

Dialysis patient who became acutely hypertensive post dialysis Describe the findings

A note about EPO • Side effects as listed on product monograph: o >10% = HTN, headache, fever o 1 -10% = DVT, edema, thrombosis o Cardiovascular: Erythropoiesis-stimulating agents increase the risk of serious cardiovascular events, thromboembolic events, stroke, and mortality when administered to target Hgb levels >11 g/d. L (and provide no additional benefit); a rapid rise in Hgb (>1 g/d. L over 2 weeks) may also contribute to these risks. o CKD concerns; use the lowest dose sufficient to reduce the need for RBC transfusions o HTN / Cardiovascular concerns; decrease the epoetin dose if the hemoglobin increase exceeds 1 g/d. L in any 2 -week period. o Seizure concerns; increased risk in CKD, thus monitor upon initiation

Practical Point Summary Renal Neurology

Practical Point Name 2 potential etiologies for myelopathy in CRF patient? 1. Zinc (PO or IV) given thus causing a Cu deficient state 2. Acquisition of HTLV 1 via blood transfusions during HD 3. Epidural hematoma (coagulopathic) 4. SC infarct (vascular RF)

Practical Point Clinical Exam Pearl • Asterixis and myoclonus may be elicited with the hands outstretched, but may be more sensitively assessed by looking at the protruded tongue or the index finger raised with the palm placed on a firm surface

CASE 6 32 F “African American”. Febrile illness culminating in seizure. R frontal lesion identified and biopsied. Dx? • Non-necrotizing granuloma • Giant cells • -ve stains for fungus or TB
")
Neurologic Manifestations of Systemic Inflammatory Disease(s)

Fundamentals of Sarcoid • Dx of exclusion – Must r/o tuberculous, fungal, carcinomatous seeding • Defined by histologic terms, thus mandates tissue Bx – Bx shows 3 cardinal features 1. Macrophage reaction with epitheloid histiocytic differentiaion of macs, without necrosis “non-caseating” 2. Multinucleated giant cells 3. Lymphcytic of monocytic infiltration • Must go the ‘whole 9 yards’, as sarcoidosis is treatable; potentially reversible

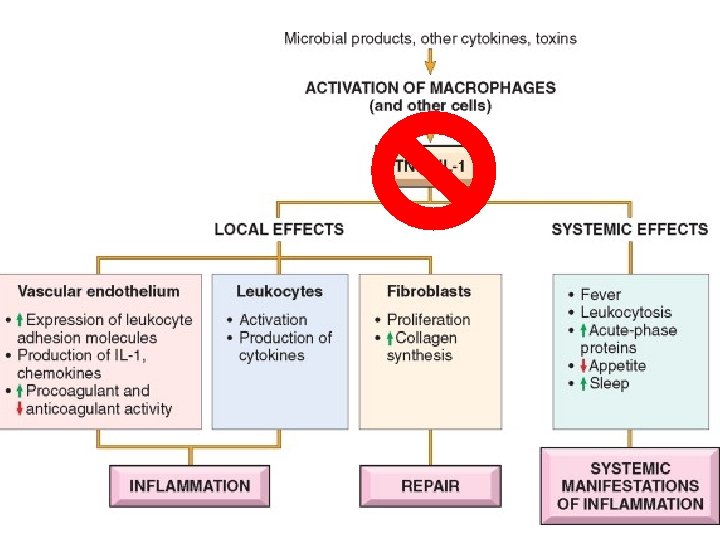
TNFα Produced by WBC and endothelia in response to inflammation Proinflammatory response Produced by macrophages as well and auto-amplifies cascade

What % of Sarcoid Patients Develop Nervous System Involvement? • Only 5% of sarcoid patients have neurologic involvement • Up to 35% of patients with NS can present with only nervous system manifestations • Isolated CNS sarcoid is exceedingly rare.
 – Arthritis –")
“Lofgren’s syndrome” • “Acute” systemic phenotype (9 - 34% of patients) – Arthritis – E. nodosum – Bilateral hilar adenopathy

Practical Point “Heerfordt’s Syndrome” Heerfordt’s Syndrome Uveoparotid syndrome • Parotid gland enlargement/Swelling • Uveitis • Facial neuropathy (CN VII) • Fever HIGHLY SUGGESTIVE OF SARCOID!

Clinical Presentation; “protean” • • • Constitutional ++ Pulmonary; fibrosis, dysnpea Ophthalmologic; uveitis, vitritis, retinal vasculitis Dermatologic; e nodosum CNS; see next slide Cardiac; arrythmias Hepatic; infiltration with variable impairment LFT MSK; neuropathy, myopathy Metabolic; hypercalcemia, calciuria

Practical Point
![Neurosarcoid Mayo Clinic Series [84 pt’s] • • • • Cranial nerve 65% Myelopathy](https://present5.com/presentation/a363447919d1ab69aa90730a97c0766b/image-76.jpg "Neurosarcoid Mayo Clinic Series [84 pt’s] • • • • Cranial nerve 65% Myelopathy")
Neurosarcoid Mayo Clinic Series [84 pt’s] • • • • Cranial nerve 65% Myelopathy 18% Cauda / Conus syndrome 3. 5% Polyradiculopathy 2. 3% Cerebellar 4. 7% Hemiparesis 2. 3% Myopathy 6% H/A 25% Encephalopathy 12% HC 8. 3% Sz 8. 3% Hypothalamic / pituitary 17% Chronic meningitis (h/a, encephalopathy, HC, sz or CN palsy with CSF pleocytosis; no parenchymal pathology) 77%
![Neurosarcoid Mayo Clinic Series [84 pt’s] • • • • Cranial nerve 65% Myelopathy](https://present5.com/presentation/a363447919d1ab69aa90730a97c0766b/image-77.jpg "Neurosarcoid Mayo Clinic Series [84 pt’s] • • • • Cranial nerve 65% Myelopathy")
Neurosarcoid Mayo Clinic Series [84 pt’s] • • • • Cranial nerve 65% Myelopathy 18% Cauda / Conus syndrome 3. 5% Polyradiculopathy 2. 3% Cerebellar 4. 7% Hemiparesis 2. 3% Myopathy 6% H/A 25% Encephalopathy 12% HC 8. 3% Sz 8. 3% Hypothalamic / pituitary 17% Chronic pachymeningitis (h/a, encephalopathy, HC, sz or CN palsy with CSF pleocytosis; no parenchymal pathology) 77%

Summary: Neurosarcoid • Chronic pachymeningitis (h/a, encephalopathy, HC, sz or CN palsy with CSF pleocytosis; no parenchymal pathology) 77% • Cranial nerve 65% – VII, VIII, II • H/A 25% • Myelopathy 18% • Hypothalamic / pituitary 17%

Practical Point Neurosarcoid; Investigation • Routine; Peripheral blood counts, Serum chemistries, including creatinine and liver enzymes • ECG • Postero-anterior chest radiograph or CT chest • PFTs, including spirometry and DLCO • Tuberculin skin test, and negative stains on Bx – Non-caseating granulomas on tissue bx • ACE level (84% PPV, 74% NPV) • Urine calcium / serum calcium • BAL (CD 4: CD 8) – reduced number of CD 8 cells, an elevated CD 4 to CD 8 ratio, and an increased amount of activated T cells, CD 4 cells, immunoglobulins, and Ig. G-secreting cells • Routine ophthalmologic examination

CSF in Neurosarcoid • Most sensitive biomarker is elevated CSF protein – I. e, normal protein argues strongly against the dx – Not specific • Low glucose (variable); 15% • Pleocytosis common; 72% – 0 -455 cells (mainly lymphs) • OCB; 18%

ACE; setting the record straight • May be helpful with routine chemistries – Secreted by sarcoidal granulomas • Approximately 60% elevated in systemic disease – Lacks sensitivity and specificity • Not useful in CSF (sensitivity 24%) – False positive also very alarming (fungal meningitis, carcinomatous) • So, do not hang your hopes of the ACE level

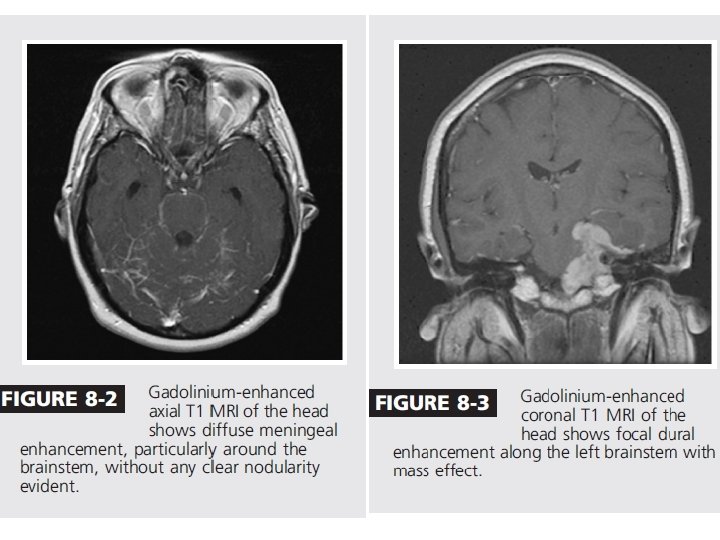
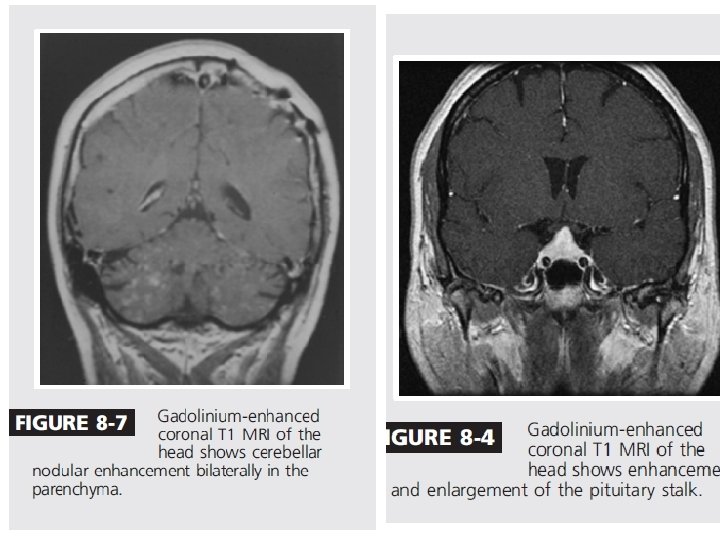
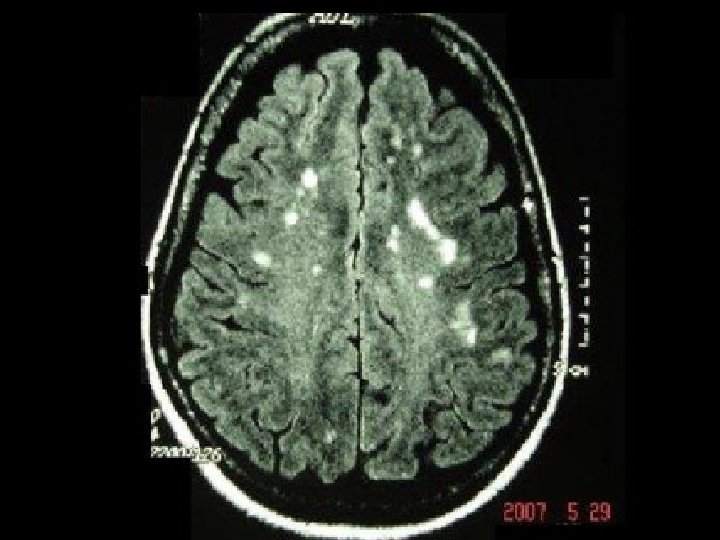
MR features of neurosarcoidosis • CNS intraparenchymal lesions of high T 2 signal and G+ enhancement • Pituitary / sella, leptomeningeal and nerve root (including cranial) with G+ enhancement • Dural enhancement • Optic nerves • Basal meningitis +/- communicating hydrocephalus
 • Most")
Neuro-Ophthalmologic Manifestations • 2 nd most common system involved (next to pulmonary) • Most frequently, the anterior segment is involved. • Chronic granulomatous uveitis, • conjunctival granulomas, scleritis, episcleritis, and interstitial keratitis. • Posterior segment • Vitritis and periphlebitis • it is sometimes the sole manifestation of ocular sarcoidosis but usually accompanies abnormalities in the anterior segment. • Severe vasculitis associated with exudates gives the appearance of candle-wax drippings.

Neuro-Ophthalmologic Manifestations • With chronic inflammation in the lacrimal system, the patient may develop keratoconjunctivitis sicca (secondary granulomas) • Ophthalmopathy; Exactly mimics thyroid eye disease – Spares the tendon

C=anterior uveitis and synechiae Enlarged nodular lacrimal gland candle-wax drippings White, mutton-fat, granulomatous keratic precipitates

Practical Point Blind Bx of What Can be used to confirm non-caseating granulomas for CNS sarcoid? • • • Lip/minor salivary gland Rectum Abdominal fat pad Duodenum Meninges Conjunctiva

Practical Point Blind Bx of What Can be used to confirm non-caseating granulomas for CNS sarcoid? • • • Lip/minor salivary gland Rectum Abdominal fat pad Duodenum Meninges Conjunctiva

Deciding on Therapy • Tissue Dx 1 st and foremost • Decide on biomarker that will be followed to tailor therapy – CSF pleocytosis – MR enhancing lesions* • May take months for G+ enhancement to disappear despite clinical response – Neurologic clinical deficits

Therapy • Cornerstone is corticosteroids – 3 induction options 1. 1 g IVMP qd x 5 d, then oral pred 60 mg / day 2. Pred 60 mg/day or 1 mg/kg 3. Pred 60 mg po q. OD from onset • Steroid sparing agents (many options) – No RTC evidence • Neurosurgery • Cranial irradiation Plan for a minimum of 6 months of therapy Relapse rate 10 -30% in successfully treated patients

Cornerstone of therapy
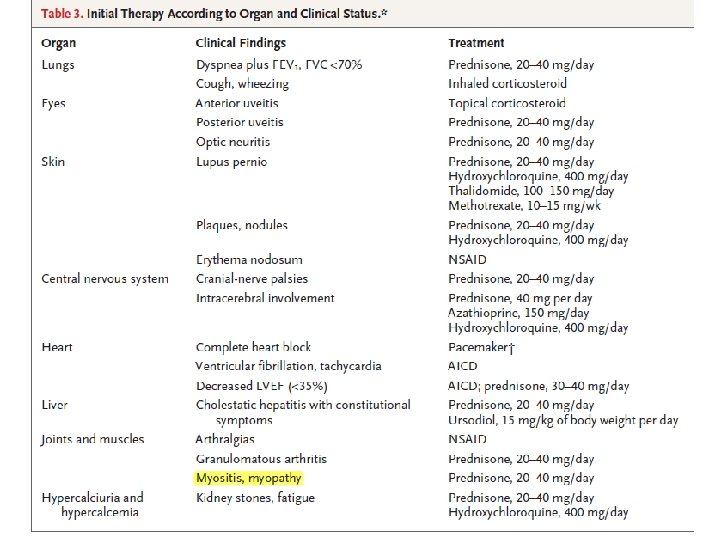

Treatment Options Immunomodulators • • • Corticosteroids Azathioprine Methotrexate Chlorambucil Cyclophosphamide Cyclosporine Hydroxychloroquine* Mycophenolate mofetil Tacrolimus TNF α blockers • • Thalidomide Pentoxyfylline Infliximab* Etanercept DO NOT FORGET • DEXA, calcium, Vit D, bisphosphanate • Septra 3 X/wk • PPI or H 2 blocker • BP and CBGM checks in collaboration with GP / Internist

CASE 9 Name this test and most likely Dx 34 F, 6 month Hx of patchy sensory phenomena over thighs, calves, forearms and nose. Systems review reveals only complaints of dry mouth and eye (sicca); no other autonomic complaints
 SS • More severe sicca")
Xeropthalmia, xerostomia, keratoconjunctivitis sicca Sjögren Syndrome • Primary (50%) SS • More severe sicca complex • Secondary (50%) SS • RA, SLE, dermatomyositis, MCTD • Milder, slower progression • Clinically; Sicca complex • Pathologically; lymphocytic infiltration of exocrine glands • Neurological manifestation(s) can sometimes be the first manifestation of the systemic disorder [1/3 present with ‘extraglandular’ manifestations] • Manifestations?

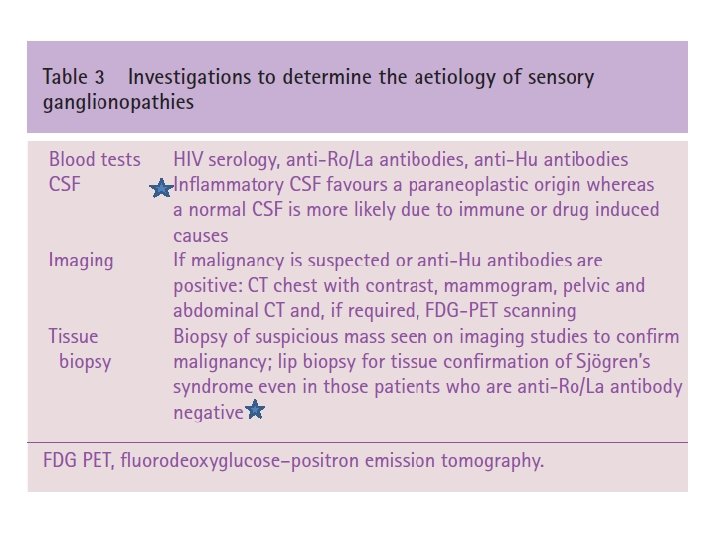
Diagnostic criteria exist • Beyond scope of this talk • Objective clinical findings with subjective sicca complaints and histopathology – Serology; anti SSA (Ro) and anti SSB (La) [60%] – Schirmer’s Test – Rose Bengal for corneal abraisons – Parotid gland salivary production (nuclear med) – Minor salivary gland (lip) biopsy Important exclusions: RTX, anti-chol Rx, HCV, AIDS, preexisting lymphoma, sarcoid, GVHD
 CN V MS mimic; clinical and paraclinical")
Sjögren’s Syndrome Primarily PNS CNS (poorly characterized) CN V MS mimic; clinical and paraclinical The optimal management of peripheral nervous system complications of SS is unclear (usual players involved IVMP, IVIG) Spontaneous improvement does occur

Practical Point Clinical Neurology • Classic case: – – – – severe loss of vibration and proprioception sensation, pseudoathetosis in her fingers, areflexia, sensory ataxic gait Romberg sign Pupillary abnormalities (see below) Autonomic neuropathy • Adie’s tonic pupils (ciliary ganglionitis) Sensory Wandering = Pseudoathetosis http: //www. nejm. org/doi/full/10. 1056/NEJMicm 0907786

For your interest only

Neuro-Sjogren’s • Sensory ataxic neuronopathy with autonomic involvement is highly suggestive of SS. • Peripheral nervous system disease often precedes the clinical diagnosis of SS. – Distal paresthesias, which may gradually spread more proximally, and loss of JPS • The MRI in patients with a sensory ataxia may show T 2 hyperintensity in the cervical spinal cord. – Ganglioneuritis may be the cause of the sensory ataxic form of neuropathy seen in SS

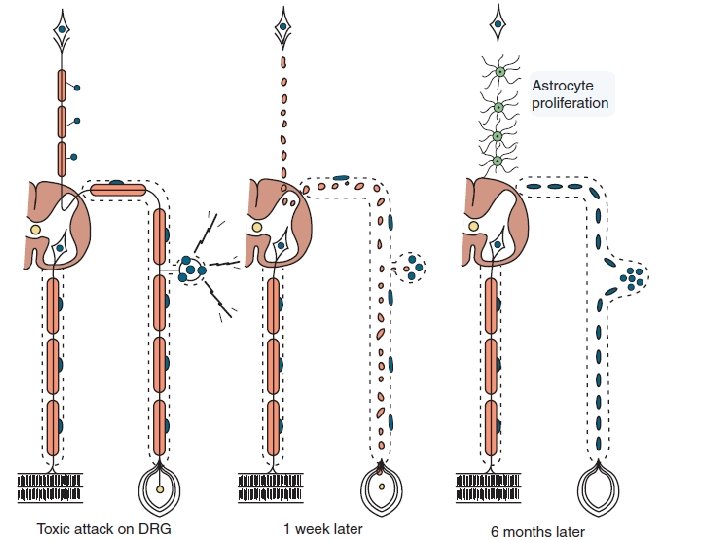
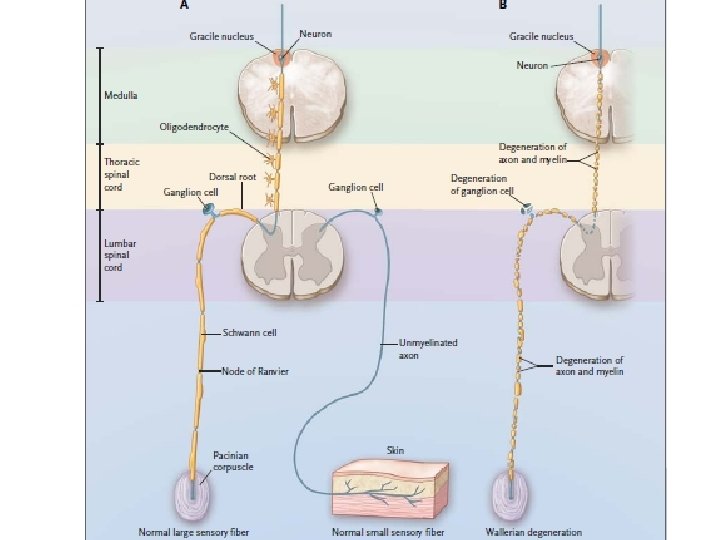
Ddx dorsal column hyperintensities • • • B 12 deficiency DRG-opathy Freidrich’s Ataxia Cu Deficiency Dorsalis Tabes HIV vacuolar myelopathy T 2 hyperintensities in the dorsal columns is the neuroradiological correlate of degeneration of large myelinated sensory fibres due to damage to the dorsal root ganglion cells (as has been confirmed in pathological studies) T 2 hyperintensities therefore possibly reflects gliosis.

Clinical Clues to Ganglionopathy Can occur to small and large fibers • It may be difficult to distinguish numbness of small fiber sensory peripheral neuropathy from that of sensory ganglionopathy based just on clinical grounds. • Aside from lower and upper extremity sensory impairment, the face may be affected (nose) • EDX: reduced or absent SNAPs and normal (or near normal) CMAPs – Normal f-waves – Abnormal H-Reflexes

Note Association b/w SS and NMO • Neuromyelitis optica can occur in association with SS – Anti-SSA (Ro) frequently found in NMO patients (with or without SS) – NMO-Ig. G prevalence same in SS pt’s without NMO • If diseases co-exist, treat NMO-spectrum disorder as if no SS – Generally involve IVMP, PLEX, azathioprine
")
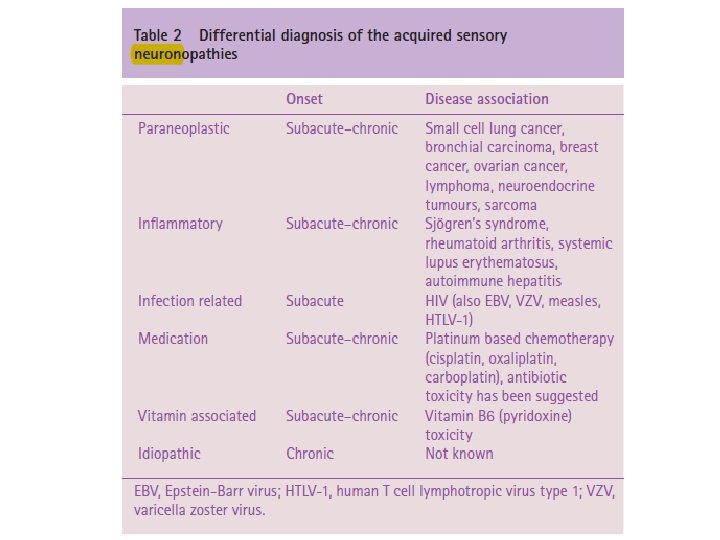
Practical Point Can you name a brief differential for selective sensory neuronopathy? (4)

Ddx primarily sensory, patchy, nonlength dependent neuropathy 1. Toxic neuronopathy (chemo = cisplatin, pyridoxine > 250500 mg /d) 2. Paraneoplastic sensory neuronopathy • SCLC; Anti-Hu Ab 3. Acute sensory neuronopathy syndrome • Post anti-biotic use [Flagyl] 4. Chronic idiopathic ataxic neuronopathy • ? unknown toxic exposure 5. Neuronopathy associated with SS 6. Primary biliary cirhhosis related ganglionopathy / neuropathy • Immune mediated 7. Sarcoidosis 8. Gluten Enteropathy
 presents with a non-compressive foot drop. •")
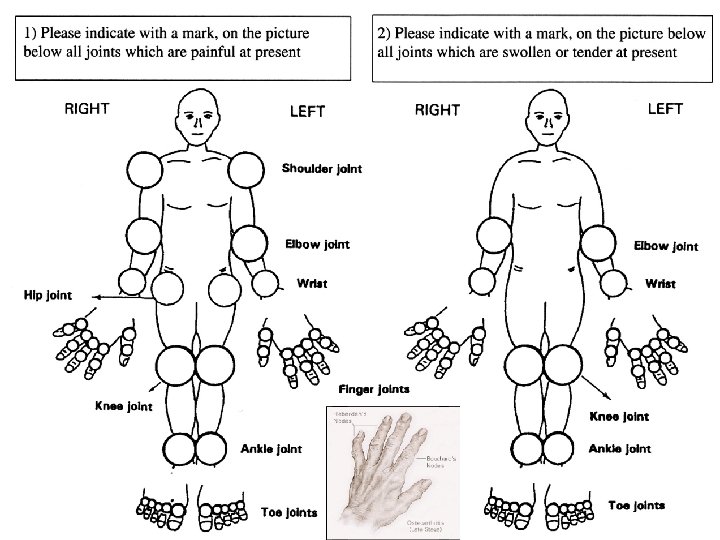
CASE 10 48 F with hands (shown) presents with a non-compressive foot drop. • What’s the most likely Dx and pathophysiology?

CASE 11 32 F with JRA presenting with acute tetraparesis after a fall, requiring ventilatory support. • What’s the most likely underlying pathophysiology?
 1. Systemic inflammatory disease characterized primarily by a polyarthritis due to")
Rhumatoid Arthritis (RA) 1. Systemic inflammatory disease characterized primarily by a polyarthritis due to chronic synovial tissue inflammation – Can progress to cartilage damage and bone erosion – Spares the spine (C-spine exception) 2. Nervous system complications related to disease process itself or therapies
 4/7 necessary 2/3; not sensitive or specific")
Not DIP (OA) 4/7 necessary 2/3; not sensitive or specific

Practical Point

Neuro-RA • CNS – Atlanto-axial instability; high cervical myelopathy with quadriparesis and respiratory failure • Asymptomatic, neck pain and paresthesias, occipital headaches from C 2 – Myelopathy may also result from compression by extradural rheumatoid nodules or by epidural lipomatosis (chronic steroid use) – VBI from damage to vertebral a. ’s – Rhumatoid meningitis (pachy or lepto) and Rhuamtoid vasculitis (rare), Sz, dementia, hemiparesis, cranial nerve palsy, blindness, hemispheric dysfunction, cerebellar ataxia, or dysphasia, “NPH”
 and C 2 (the axis)—particularly the space")
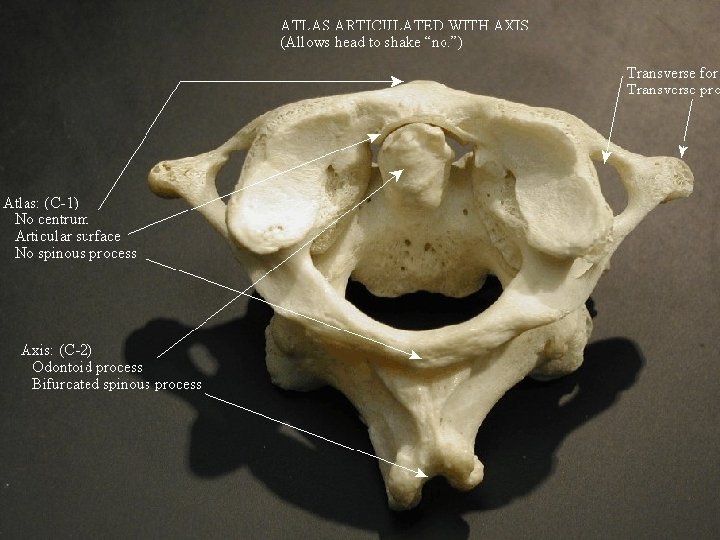
The joints between C 1 (the atlas) and C 2 (the axis)—particularly the space between the transverse atlantal ligament and the odontoid process, and the joint between the anterior atlas arch and the odontoid—are the most common sites of cervical involvement in RA

Destruction of articular facets of C 2, resulting in descent of the skull and upward migration of the odontoid

Gross destruction of the dens axis Extensive pannus formation

Stepladder phenomenon

Surgical Indications • Strong indications for surgery to reduce the subluxation and stabilize the spine include myelopathy (or brainstem compression from basilar invagination) and intractable pain or severe stenosis in conjunction with spinal instability (Kim and Hilibrand, 2005). • Note: – Caution with intubations – Office maneuvers (such as Dix Hallpike)
 • PNS")
Neuro-RA Median, post tib, une, enw, PIN (supinator and hypertrophied synovial tissue) • PNS – Entrapment neuropathies – rheumatoid tenosynovitis, nodules or joint deformities – Vasculitic Necrotizing Neuropathy (noncompressive) – Neuropathy (axonal); DSPN (sensory) – Mononeuritis multiplex Medium-sized epineurial blood vessel with fibrinoid necrosis of its wall and perivascular and transmural mononuclear cell infiltration
 • Methotrexate is now one of the most commonly used")
Practical Point (? irreversible) • Methotrexate is now one of the most commonly used DMARD in RA • Anti-malarials • Newer biologics

Practical Point Methotrexate Toxicity; know it. • Rare AE with oral, low-dose conventional Tx • Can get severe leukoencphalopathy with higher dose IV or IT; especially if concomitant RTX – Malignancy treatment (i. e, ALL; Dana Farber Protocol) • Don’t forget myelopathy

Methotrexate Leukoencephalopathy

Newer Biologics • DMARD therapy failure • TNF-α inhibitors AVOID IN PATIENTS WITH PAST HX of MS or other CNS Adverse Effects: Effects DEMYELINATING DISEASES – Infliximab (Remicade) – Etanercept (Enbrel) – Adalimumab (Humira) – increased risk for systemic infection, lymphoma – reactivation of TB CNS demyelination (R, H) Bilateral anterior toxic optic neuropathy (R) CIDP-like neuropathy (E) MMNCB (R)

Almost done. . .

56 M fever and left pronator drift. Swollen L ankle. ESR 274, CRP 300 Practical Point Name this important funduscopic finding. What immediate test(s) should you order next?

Potential Future Topics • Neuro-Lupus • Electrolytes Disturbances in Neurology • Vascular complications of systemic diseases – i. e, IE, SBE, cancer, hemoglobinopathies, APLAS and CAPS • Neuro-Hematology – B 12, TTP-HUS, ITP, homocysteine metabolism • Neurooncology • “Myelopathies in cancer patients” or “stroke in cancer patients” • CNS/PNS complications of cancer • Complications of – Rx, RTX, Surgery • The paraneoplastic wonderland • Neurologic complications of pregnancy and delivery
 Advice to R 5’s; Writing The Quiz • Keep your cool when")
Practical Point(s) Advice to R 5’s; Writing The Quiz • Keep your cool when under fire • ABC’s • Dissect the case slowly, an ‘aha’ moment will hopefully occur • CNS/PNS involvement if common pathologies, or the most talked about presentations – No zebras on RCE (for the most part) • Know your approach to hyponatremia and thrombocytopenia • Do not be afraid to consult; know your limits

Post-Test • Neurologic manifestations of celiac disease is primarily related to specific vitamin deficiency state(s) T/F • The CNS is the second most common system involved in sarcoid (outside of pulmonary) T/F • Most sensitive biomarker for neurosarcoid is CSF ACE level T/F • Phenytoin is contraindicated in a liver failure patient T/F • Name a purported biomarker that indicates active neuropsychiatric SLE. Anti-Ribosomal P (stay tuned for next talk) • SS is one of the classic syndromes associated with sensory neuronopathy T/F • It is safe to use Remicade for RA in a patient with concomitant RRMS T/F
 • Continuum; Neurologic Complications of Systemic Disease (access via VPN or AAN")
References (reviews) • Continuum; Neurologic Complications of Systemic Disease (access via VPN or AAN membership). Feb 2008, 2011 • The dorsal root ganglion under attack: the acquired sensory ganglionopathies. Pract Neurol 2010; 10: 326– 334 • Intravenous thrombolysis in Sneddon’s syndrome. Case Reports / Journal of Clinical Neuroscience 19 (2012) 326– 328 • Neurosarcoidosis: a clinical dilemma. Lancet Neurology Vol 3 July 2004 • Metabolic Encephalopathies. Neurol Clin 29 (2011) 837– 882 • Robbins Pathology – Sarcoid pathophysiology • Bradley: NICP • Uptodate. com

• Curr Opin Neurol 2012, 25: 306– 315
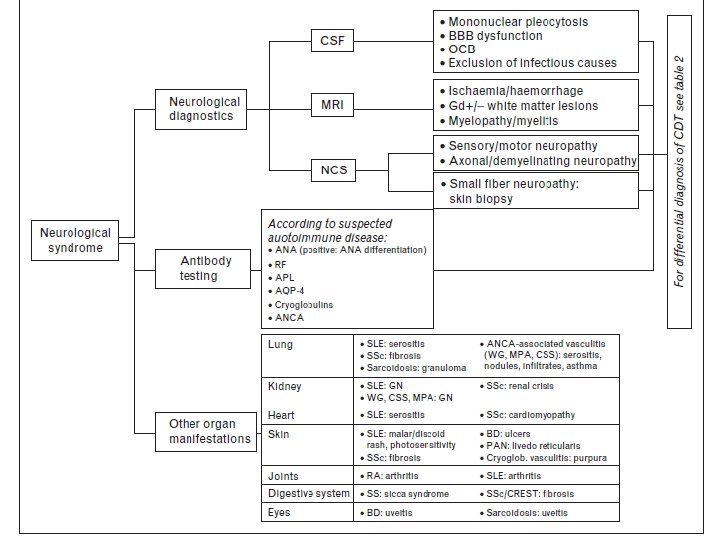

SLE SS Systemic Sclerosis RA Behcet
a363447919d1ab69aa90730a97c0766b.ppt