f8735b00978a002b804131a57bc307c9.ppt
- Количество слайдов: 40



Nephrogenic Systemic Fibrosis: An Update Neil M. Rofsky, MD BETH ISRAEL DEACONESS MEDICAL CENTER Harvard Medical School

MR Contrast Agents: Principles • Unpaired electrons alter magnetic environment • A trait of certain metal ions • • • Indirectly affects the local H 20 Naked metal ions are toxic! Ligands for safety • (metal + ligand = chelate) Gd 3+ Gd-DTPA-BMA (Omniscan) Gd-DOTA (Dotarem)
: The Basics • Originally known as Nephrogenic Fibrosing Dermopathy (NFD)")
Nephrogenic Systemic Fibrosis (NSF): The Basics • Originally known as Nephrogenic Fibrosing Dermopathy (NFD) • Systemic proliferation of connective tissue (NSF) • “Over 215 cases reported worldwide. . ” from 1997 present • Strong epidemiologic association with Gd • Appears to be a class issue (Omniscan >>> Magnevist, Opti. MARK) • Almost all renal insufficiency at exposure (most ESRD, on dialysis) • Proinflammatory events in many 11 (e. g. , vascular surgery, sepsis, thrombosis) • Some data suggests 3 -5% incidence w/ Gd in setting of renal failure 11 • So far no co-factor identified (dialysate, ACEIs, EPO, etc. ) • Theories of pathogenesis:

Patient Safety a Decade Later… 1997 FDA issues Public Health Advisory Gd “trigger” proposed for NSF (Grobner First recognized case of “NFD” and Markmann) 2000 First description of NSF in the literature Apr 2006 May 2006 FDA revises Public Health Advisory Literature reports Gd in NSF skin biopsies 7 Jun 2006 Dec 2006 Jan 2007 Press reports FDA warning to “kidney patients” Editorial in Radiology Danish Medicines Agency reports 25 cases of Gdassociated NSF
: • MRA • Peripheral • Renal")
Uses of High Dose Gd (+/- renal insufficiency): • MRA • Peripheral • Renal • Neuro-onc (local practice patterns) • X-ray use (k-edge of Gd is inefficient) • CT • Conventional Angio
: Diagnosis • Most prominent and visible effects in the skin")
Nephrogenic Systemic Fibrosis (NSF): Diagnosis • Most prominent and visible effects in the skin • • • Discoloration & texture changes Tightening, thickening, swelling → joint immobility Burning, itching, sharp pain • Skin changes can be insidious -> confused w/ peripheral edema • Resembles scleroderma and eosinophilic fasciitis • Absent: monoclonal gammopathies 9, Raynaud phenomenon and autoantibodies 2 • Yellowish scleral plaques • Fibrotic changes can be widespread (liver, lungs, heart) • Biopsy Findings • Skin biopsy: thickened collagen bundles with surrounding clefts, mucin deposition, ↑ fibroblasts, ↑ CD 34+ dendrocytes 2
: Prognosis and Treatment • Course is chronic, progressive, variable •")
Nephrogenic Systemic Fibrosis (NSF): Prognosis and Treatment • Course is chronic, progressive, variable • May be severely debilitating • • Contractures - musculoskeletal Wheelchair requirement in some • Complications may be fatal • • Falls, fractures Immobility, pneumonia • No consistently successful treatment • Symptoms may improve if renal function improves • Limited evidence for kidney transplantation, extracorporeal photopheresis (ECP) • Also in the literature: oral steroids, plasmapheresis

What we know about Gd and NSF • Causation not established; data are suspicious, but have limitations • Retrospective studies • Info is limited (e. g. , Creatinine at time of Gd exposure, contemporaneous administration) • Markedly prolonged half-life in renal failure • All cases had renal dysfunction at time of Gd exposure • Relationship between risk and level of dysfunction • Relationship between risk and cumulative dose? • Theoretical risk with any Gd contrast agent • Risk different across agents (e. g. , due to excess chelate)? • Cases typically develop in days to few months after Gd exposure Half-life of gadodiamide (hours)4 Normal renal function 1. 3 h End-stage renal failure 34. 3 h Hemodialysis (HD) 2. 6 h Peritoneal dialysis (PD) 52. 7 h
 Opti. Mark, Gd.")
Brand Name, Chemical Name Amine backbone structure log Kst (Stability constant) Opti. Mark, Gd. DTPA-BMEA Linear 16. 8 Omniscan, Gd. DTPA-BMA Linear 16. 8 Magnevist, Gd. DTPA Linear 22. 2 Multi. Hance Gd. BOPTA Linear 22. 6 Gadovist Gd. DO 3 A-butrol Macrocyclic 21. 0 Pro. Hance, Gd. HPDO 3 A Macrocyclic 23. 8 Dotarem Gd. DOTA Macrocyclic 25. 6 Thermodynam stability
 (Optimark) Gd-DOTA (Dotarem) Gd-BT-DO 3 A (Gadovist) Gd-DTPA-BMA (Omniscan) Gd-BOPTA (Multi. HANCE)")
Gd-DTPA (Magnevist) (Optimark) Gd-DOTA (Dotarem) Gd-BT-DO 3 A (Gadovist) Gd-DTPA-BMA (Omniscan) Gd-BOPTA (Multi. HANCE) Gd-EOB-DTPA (Primovist) Gd-HP-DO 3 A (Pro. HANCE)
![ML M + L KD = [ M ] [ L ] [ ML](https://present5.com/presentation/f8735b00978a002b804131a57bc307c9/image-11.jpg "ML M + L KD = [ M ] [ L ] [ ML")
ML M + L KD = [ M ] [ L ] [ ML ] 10 -23 = x x 500 (m. M) OR, 3+ ] 5 x 10 – 21 = x 2 7 x 10 – 10 = x = [Gd
 Dissociation rate in")
Brand Name, Chemical Name Amine backbone structure log Kst (Stability constant) Dissociation rate in 0. 1 M HCl ( sec-1) Opti. Mark, Gd. DTPABMEA Linear 16. 8 >2. 2 x 10 -2 Omniscan, Gd. DTPABMA Linear 16. 8 >2 x 10 -2 Magnevist, Gd. DTPA Linear 22. 2 1. 2 x 10 -3 Multi. Hance Gd. BOPTA Linear 22. 6 -not reported- Gadovist Gd. DO 3 Abutrol Macrocyclic 21. 0 2. 8 x 10 -6 (estimated from data) Pro. Hance, Gd. HPDO 3 A Macrocyclic 23. 8 6. 4 x 10 -5 Dotarem Macrocyclic 25. 6 8. 4 x 10 -7

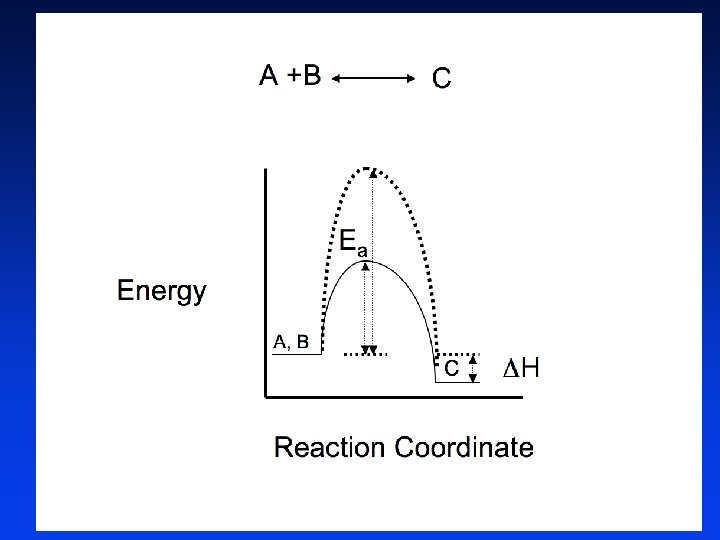
The themodynamic stability constant determines the concentrations of the Gd-chelate, free chelate, and free gadolinium at equilibrium; The rates of formation and dissociation, dictated by Ea , determine how rapidly these compounds reach equilibrium.

Relaxivity ’s in solution p. H 7. 0 Zn Gd L ↕ Gd + L 4 4 4 PO PO PO R 1 at 3 days ↓ 50% ↓ 90% ↓ 60% NO SIG Laurent S, et al. . Contrast Media Mol Imaging 4 PO PO 4 Compound Gd-DTPA-BMA Gd –BOPTA Gd-HP-DO 3 4 Pb. O

a very strong correlation between the dissociation rates of chelates in acid and the long-term deposition of Gd 3+ in rat tissues such as liver and bone (femur). Wedeking, Kumar and Tweedle

“Acid dissociation rate constants were the most accurate parameters linking in vitro and in vivo dissociation. “ “Gd(HP-D 03 A) and Gd(DOTA)-, had the lowest residual Gd 3+ in whole animals. ” “No evidence of free Gd 3+ could be detected for Gd(HP-D 03 A) using the free Gd 3+ target tissues (liver and femur) at long residence times. ” Wedeking, Kumar and Tweedle, Mag Res Imag 1992

Algorithm for Gd-Enhanced MRI Gd-MRI in last 7 days? START YES Consider delay to allow 7 days between Gd doses NO Proceeding Inpatient Outpatient / EU e. GFR w/in 3 days If worsening trend, day of exam Response to Choyke questions “NO” to all “YES” to any e. GFR within 4 weeks DIALYSIS e. GFR < 30 On PD e. GFR < 30 On HD e. GFR < 30 No dialysis Discussion w/ referrer Proceeding Obtain central venous access HD x 2 w/in 2 hrs and 24 hrs Informed consent e. GFR 30 -60 e. GFR > 60 Limit Gd to 0. 1 mmol/kg*; Consider hydration Pro. Hance™ or Multi. Hance™: No > 0. 1 mmol/kg *Except for run-offs, which are permitted up to 0. 2 mmol/kg after risk: benefit discussion w/ referrer. OK to proceed

Algorithm for Gd-Enhanced MRI START Gd-MRI in last 7 days? YES Consider delay to allow 7 days between Gd doses NO Proceeding Outpatient / EU Response to Choyke questions “NO” to all Point of service query OK to proceed

Minimizing the Risk of NSF • Risk : benefit analysis • Reduce use of Gd in renal disease • • FDA recommends avoiding for e. GFR < 30 Consider non-contrast protocols Consider alternate modality (e. g. , CT, conventional angiogram) Minimize dose if Gd is deemed imperative • Consider alternative agents • Gd-BOPTA (Multi. HANCE®) • No reports (yet…) • Can reduce dose (has higher R 1) • HOWEVER…clearance kinetics less favorable (binds protein) • Pro. HANCE • Hemodialyze patients with ESRD asap ? ? * • Gd excretory rates 78%, 96%, 99% from 1 st to 3 rd HD session 5 • When using Gd, maximize pt condition*: • Hold drugs that decrease renal function (e. g. , diuretics, NSAIDs) • Hydrate (consider bicarb – ? role of metabolic acidosis in NSF) • Informed consent *(not evidence based!!)

How do we screen for risk? • Choyke Questionnaire • Serum Creatinine • Point of Service Devices? ? • http: //www. abbottpointofcare. com/is tat/#
 l Proteinuria (OR 8.")
The Choyke Questionnaire l Pre-existing renal disease (OR 13. 6) l Proteinuria (OR 8. 7) l Prior kidney surgery (OR 8. 1) l Hypertension (OR 5. 4) l Gout (OR 4. 6) l Diabetes (OR 3. 2) Completely negative responses: Ø 450 (67%) of 673 Ø 446/450 (99%) Cr values 1. 7 mg/d. L Ø 424/450 (94%) - normal Cr values Choyke, et al. Tech Urol 1998; 4:

Algorithm for Gd-Enhanced MRI Gd-MRI in last 7 days? START YES Consider delay to allow 7 days between Gd doses NO Proceeding Inpatient Outpatient / EU e. GFR w/in 3 days If worsening trend, day of exam Response to Choyke questions “NO” to all “YES” to any e. GFR within 4 weeks DIALYSIS e. GFR < 30 On PD e. GFR < 30 On HD e. GFR < 30 No dialysis Discussion w/ referrer Proceeding Obtain central venous access HD x 2 w/in 2 hrs and 24 hrs Informed consent e. GFR 30 -60 e. GFR > 60 Limit Gd to 0. 1 mmol/kg*; Consider hydration Pro. Hance™ or Multi. Hance™: No > 0. 1 mmol/kg *Except for run-offs, which are permitted up to 0. 2 mmol/kg after risk: benefit discussion w/ referrer. OK to proceed

Algorithm for Gd-Enhanced MRI Gd-MRI in last 7 days? START YES Consider delay to allow 7 days between Gd doses NO Proceeding Inpatient Outpatient / EU e. GFR w/in 3 days If worsening trend, day of exam Response to Choyke questions “YES” to any e. GFR within 4 weeks e. GFR < 30 No dialysis Discussion w/ referrer Proceeding Informed consent e. GFR 30 -60 e. GFR > 60 Limit Gd to 0. 1 mmol/kg*; Consider hydration Pro. Hance™ or Multi. Hance™: No > 0. 1 mmol/kg *Except for run-offs, which are permitted up to 0. 2 mmol/kg after risk: benefit discussion w/ referrer. OK to proceed

Algorithm for Gd-Enhanced MRI Gd-MRI in last 7 days? START YES Consider delay to allow 7 days between Gd doses NO Proceeding Inpatient e. GFR w/in 3 days If worsening trend, day of exam DIALYSIS e. GFR < 30 On PD e. GFR < 30 On HD Discussion w/ referrer Proceeding Obtain central venous access HD x 2 w/in 2 hrs and 24 hrs Informed consent Pro. Hance™ or Multi. Hance™: No > 0. 1 mmol/kg *Except for run-offs, which are permitted up to 0. 2 mmol/kg after risk: benefit discussion w/ referrer.
 Peritoneal Dialysis Consider alternative study 2 sessions of")
For Dialysis Patients Hemo Dialysis (HD) Peritoneal Dialysis Consider alternative study 2 sessions of HD 1 st w/in 3 hrs of Gd 2 nd ~ 24 hours after Gd No functional AV Fistual Admit for temporary central venous access Functional fistula present

Hydration & HCO 3 ? ? • Oral hydration • 1 Liter of H 20 by mouth pre- and post- injection of contrast • Intravenous hydration • Contact the ordering physician or house staff for orders • Bicarb • • 150 m. Eq of Na. HCO 3 (e. g. dilute in 1 L D 5 W) Pre: 1 hr prior to contrast administration • @ 3 cc/kg/hr and for • Post: 6 hrs after contrast administration • @ 1 cc/kg/hr • Modifications possible for pts with renal failure/CHF)

Perspective – Iodinated Contrast • Risk for severe adverse reactions • 0. 147% HI-ICM • 0. 031% NI-ICM (3/10, 000) • Death • ~ 1/100, 000 either high or low osmolality. Caro AJR 1991 Apr; 156(4): 825 -32

Conclusions • Gd is associated with NSF in pts with substantial renal insufficiency • Role of acidity seems likely • Risk: Benefit assessment is vital • What is the risk of not giving CE-MRI? • Guidelines should be submitted for institutional approval • Education is essential • Keep reading, keeping conversing! • Consider using Gadoteridol in high risk situations

References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Cowper SE. Nephrogenic Fibrosing Dermopathy [NFD/NSF Website]. 2001 -2007. Available at http: //www. icnfdr. org. Accessed 01/17/2007. http: //www. icnfdr. org. Cowper SE. Nephrogenic fibrosing dermopathy: the first 6 years. Curr Opin Rheumatol 2003; 15: 785. dermopathy: Grobner T: Gadolinium – a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrology Dialysis Transplantation 21(4): 1104 -1108, April 2006. Joffe P, Thomsen HS, Meusel M: Pharmacokinetics of gadodiamide injection in patients with severe renal insufficiency and patients undergoing hemodialysis or continuous ambulatory peritoneal dialysis. Acad Radiol 5: 491 -502, 1998. Okada S et al. Safety of gadolinium contrast agent in hemodialysis patient. Acta Radiologica, 2001, Radiologica, 42(3): 339 -341. Rofsky N et al. Renal lesion characterization with gadolinium-enhanced MR imaging: Efficacy and safety in patients with renal insufficiency. Radiology, July 1991, 180: 85 -89. High WA, Ayers RA, Chandler J, Zito G, and Cowper SE. Gadolinium is detectable within the tissue of patients with nephrogenic systemic fibrosis. J Am Acad Dermatol 2007; 56(1): 21 -26. Stenver DI. Investigation of the safety of MRI contrast medium Omniscan. Danish Medicines Agency. Omniscan. http: //www. dkma. dk/1024/vis. UKLSArtikel. asp? asrtikel. ID=8931. Published May 29, 2006. Accessed http: //www. dkma. dk/1024/vis. UKLSArtikel. asp? asrtikel. ID=8931. February 6, 2007. Boyd AS, Zic JA, and Abraham JL. Gadolinium deposition in nephrogenic fibrosing dermopathy. J Am dermopathy. Acad Dermatol. January 2007. 27 -30. Dermatol. Marckmann P, Skov L, Rossen K, Dupont A, Damholt MB, Heaf JG, et al. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. J Am Soc Nephrol 2006; 17: 2359 -62. Sadowski EA, Bennett LK, Chan MR, Wentland AL, Garrett RW, et al. Nephrogenic systemic fibrosis: Risk factors and incidence estimation. Radiology 2007. http: //radiology. rsnajnls. org/cgi/content/full/2431062144 v 1. Published January 31, 2007. Accessed http: //radiology. rsnajnls. org/cgi/content/full/2431062144 v 1. February 1, 2007.
 • Gd Brightening")
Gadolinium Chelates • MR contrast agents (metal + ligand = chelate) • Gd Brightening on T 1 -WI’s • Gd is toxic! • Chelate ‘shields’ the free metal while preserving its relaxation effect. Gd Gd

Gadolinium Chelates • MR contrast agents • Brightening on T 1 -weighted images • Gd is toxic! • Chelate used to ‘shield’ the free metal while preserving its relaxation effect. Gd 3+ Gd-DTPA-BMA (Omniscan) Gd-DOTA (Dotarem)
: The Basics • Originally known as Nephrogenic Fibrosing Dermopathy (NFD)")
Nephrogenic Systemic Fibrosis (NSF): The Basics • Originally known as Nephrogenic Fibrosing Dermopathy (NFD) • Systemic proliferation of connective tissue (NSF) • ~ 215 cases reported worldwide from 1997 -2006 • Strong epidemiologic association with Gd • All FDA-reviewed cases had prior Gd exposure • Appears to be a class issue (Omniscan >>> Magnevist, Opti. MARK) • All had renal insufficiency at exposure (most ESRD, on dialysis) • Proinflammatory events in many 11 (e. g. , vascular surgery, sepsis, thrombosis) • Early data suggests 3 -5% incidence w/ Gd in setting of renal failure 11 • So far no co-factor identified (dialysate, ACEIs, EPO, etc. ) • Theories of pathogenesis: 10

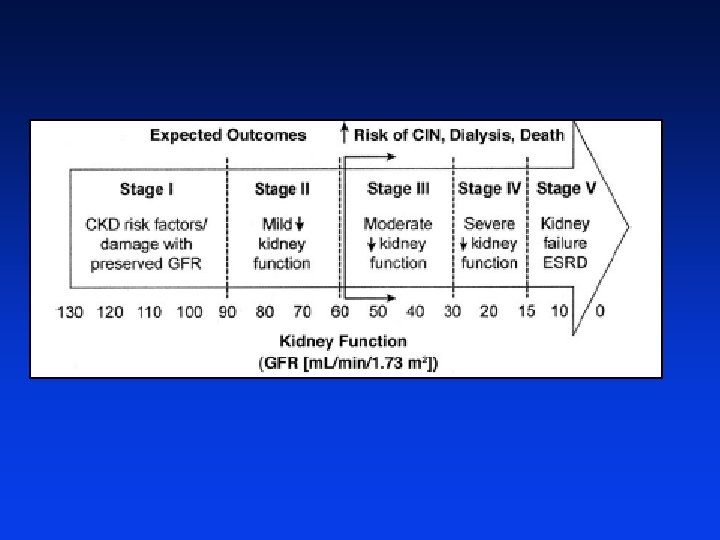
Staging of Chronic Kidney Dz Expected Outcomes Dialysis, Death ↑Risk of CIN, ↑Risk of NSF Stage 1 Stage V Stage II CKD risk factors/ damage w/ preserved GFR Mild ↓ kidney fxn 130 120 110 100 90 80 Stage III Stage IV Death ↓ Severe ↓ Moderate 70 60 kidney fxn 50 40 30 Kidney failure ESRD kidney fxn 20 15 10 0 Kidney Fxn (GFR [ml/min/1. 73 m 2]) Modified from: Am J Kidney Dis 2002; 39(suppl): S 1 -2

Algorithm for Choyke Screen; Outpt Efficacy Study Outpatient / EU Response to Choyke questions Pre- service Creat/ e. GFR “Yes” to any “NO” to all Point of service query “Yes”, “No” Point of service Creat/ e. GFR St 1 St 2 St 3 St 4 “No”, “Yes” “No”, “No” Point of service Creat/ e. GFR F/U Creat/ e. GFR; date Exam w/o Creat No F/U Creat/ e. GFR

Algorithm for Gd-Enhanced MRI Gd-MRI in last 7 days? START YES Consider delay to allow 7 days between Gd doses NO Proceeding Inpatient Outpatient / EU e. GFR w/in 3 days If worsening trend, day of exam Response to Choyke questions “YES” to any e. GFR within 4 weeks e. GFR < 30 No dialysis Discussion w/ referrer Proceeding Informed consent e. GFR 30 -60 e. GFR > 60 Limit Gd to 0. 1 mmol/kg*; Consider hydration Pro. Hance™ or Multi. Hance™: No > 0. 1 mmol/kg *Except for run-offs, which are permitted up to 0. 2 mmol/kg after risk: benefit discussion w/ referrer. OK to proceed

What we know about Gd and NSF • Causation not established; data are suspicious, but have limitations • Retrospective studies • Info is limited (e. g. , Creatinine at time of Gd exposure, contemporaneous administration) • Markedly prolonged half-life in renal failure • All cases had renal dysfunction at time of Gd exposure • Relationship between risk and level of dysfunction • Relationship between risk and cumulative dose? • Theoretical risk with any Gd contrast agent • Documented cases with Omniscan >>Magnevist, Opti. MARK • Risk different across agents (e. g. , due to excess chelate)? • Cases typically develop in days to few months after Gd exposure Half-life of gadodiamide (hours)4 Normal renal function 1. 3 h End-stage renal failure 34. 3 h Hemodialysis (HD) 2. 6 h Peritoneal dialysis (PD) 52. 7 h
f8735b00978a002b804131a57bc307c9.ppt