

edcd12dc841e7cd16648ee5b8c6fa060.ppt
- Количество слайдов: 46
 Neonatal Intensive Care Outcomes Research and Evaluation Dr. B. P. Murphy Cork University Maternity Hospital
Neonatal Intensive Care Outcomes Research and Evaluation Dr. B. P. Murphy Cork University Maternity Hospital
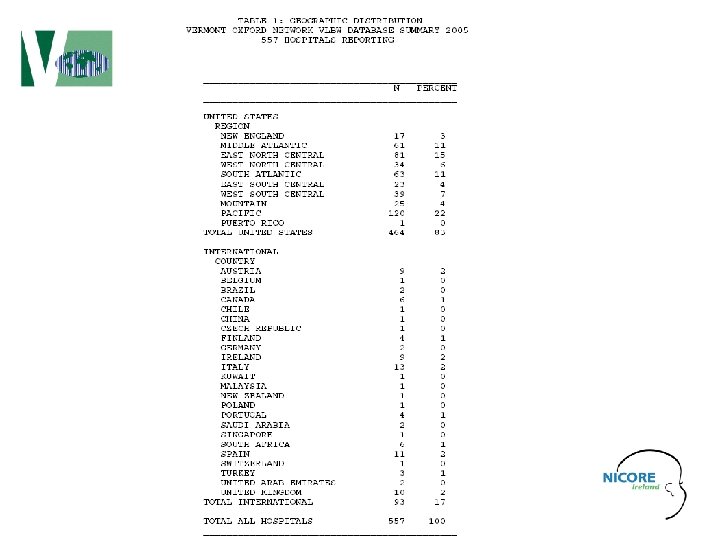
 Vermont Oxford Network improving care for infants and their families • The Vermont Oxford Network maintains one of the world's largest Databases including information about the care and outcomes for high-risk infants treated in neonatal intensive care units around the world. • The Database is used to provide participating members with feedback concerning their performance. Network reports using information from the Database are designed for use in quality improvement, internal audit, and peer review. • Participating members receive detailed, confidential reports documenting patient characteristics, treatment practices, morbidity, mortality, and length of stay at their institution. • The reports track performance over time, and compare an individual institution's performance with that of the Network as a whole and with subgroups of institutions similar to their own. • These reports assist the members in identifying opportunities for improvement and in monitoring the effects of their local quality improvement interventions.
Vermont Oxford Network improving care for infants and their families • The Vermont Oxford Network maintains one of the world's largest Databases including information about the care and outcomes for high-risk infants treated in neonatal intensive care units around the world. • The Database is used to provide participating members with feedback concerning their performance. Network reports using information from the Database are designed for use in quality improvement, internal audit, and peer review. • Participating members receive detailed, confidential reports documenting patient characteristics, treatment practices, morbidity, mortality, and length of stay at their institution. • The reports track performance over time, and compare an individual institution's performance with that of the Network as a whole and with subgroups of institutions similar to their own. • These reports assist the members in identifying opportunities for improvement and in monitoring the effects of their local quality improvement interventions.
 NICORE & VON VLBW DATABASE 1990 TO 2005
NICORE & VON VLBW DATABASE 1990 TO 2005
 9 Participating Units in South • National Maternity Hospital, Dublin • Coombe Women’s Hospital, Dublin • Rotunda Hospital, Dublin • Cork University Maternity Hospital, Cork • Our Lady of Lourdes Hospital, Drogheda • Waterford Regional Hospital • St. Munchin’s Hospital, Limerick • University College Hospital, Galway • Sligo General Hospital
9 Participating Units in South • National Maternity Hospital, Dublin • Coombe Women’s Hospital, Dublin • Rotunda Hospital, Dublin • Cork University Maternity Hospital, Cork • Our Lady of Lourdes Hospital, Drogheda • Waterford Regional Hospital • St. Munchin’s Hospital, Limerick • University College Hospital, Galway • Sligo General Hospital
 5 Participating Units in North • • • Royal Maternity Hospital, Belfast Ulster Hospital, Dundonald, Belfast Altnagelvin Hospital, Derry Antrim Hospital, Antrim Craigavon Area Hospital, Portadown
5 Participating Units in North • • • Royal Maternity Hospital, Belfast Ulster Hospital, Dundonald, Belfast Altnagelvin Hospital, Derry Antrim Hospital, Antrim Craigavon Area Hospital, Portadown
 Project details • Secure submission of anonymised data from each unit • Individual comparisons provided to each participating unit • Publication of All-Ireland annual report
Project details • Secure submission of anonymised data from each unit • Individual comparisons provided to each participating unit • Publication of All-Ireland annual report
 Project Aims • Comprehensive database for all neonatal intensive care episodes for a geographically defined population • Centralisation of data for research and clinical governance activities • Benchmarking neonatal intensive care services with defined professional standards nationally and internationally • Informed decision making regarding intensive care services in Ireland
Project Aims • Comprehensive database for all neonatal intensive care episodes for a geographically defined population • Centralisation of data for research and clinical governance activities • Benchmarking neonatal intensive care services with defined professional standards nationally and internationally • Informed decision making regarding intensive care services in Ireland
 Project aims • Encourage each unit to introduce a programme of continuing quality improvement • Provision of support (e. g. newsletter, visits, toolkits, web site) • Regular meetings of steering group representing all participating units
Project aims • Encourage each unit to introduce a programme of continuing quality improvement • Provision of support (e. g. newsletter, visits, toolkits, web site) • Regular meetings of steering group representing all participating units
 Quality Improvement • • • Transfers Antenatal steroids Admission temperature Timing of surfactant administration Screening for Retinopathy of Prematurity • Nosocomial infection
Quality Improvement • • • Transfers Antenatal steroids Admission temperature Timing of surfactant administration Screening for Retinopathy of Prematurity • Nosocomial infection
 Dissemination of results • Presentation of results to each unit and wider neonatal community through annual report, presentation and publication • Development of intervention strategy to introduce ongoing collaborative quality improvement in each unit • Linkages with Vermont Oxford Neonatal Network and Euro. Neo. Stat Network
Dissemination of results • Presentation of results to each unit and wider neonatal community through annual report, presentation and publication • Development of intervention strategy to introduce ongoing collaborative quality improvement in each unit • Linkages with Vermont Oxford Neonatal Network and Euro. Neo. Stat Network
 Vermont Oxford Network 4 Key Habits Habit for Change Habit for Evidence Based Practice BETTER PRACTICES Clinical Organizational Operational Habit for Collaborative Learning Habit for Systems Thinking
Vermont Oxford Network 4 Key Habits Habit for Change Habit for Evidence Based Practice BETTER PRACTICES Clinical Organizational Operational Habit for Collaborative Learning Habit for Systems Thinking
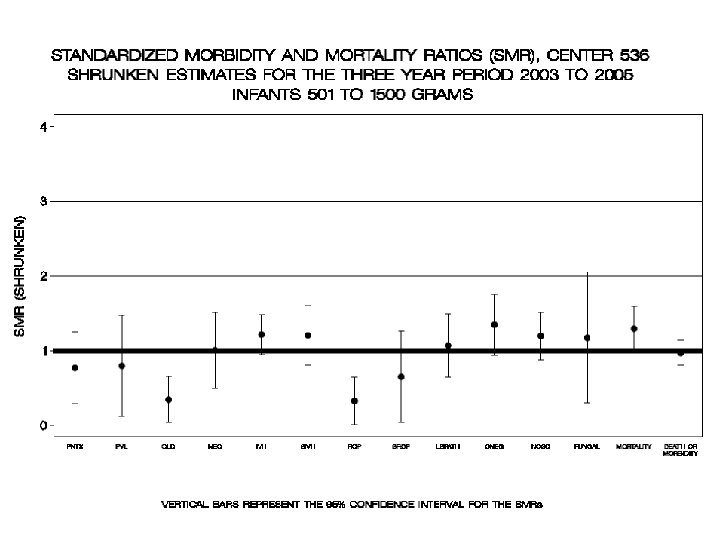
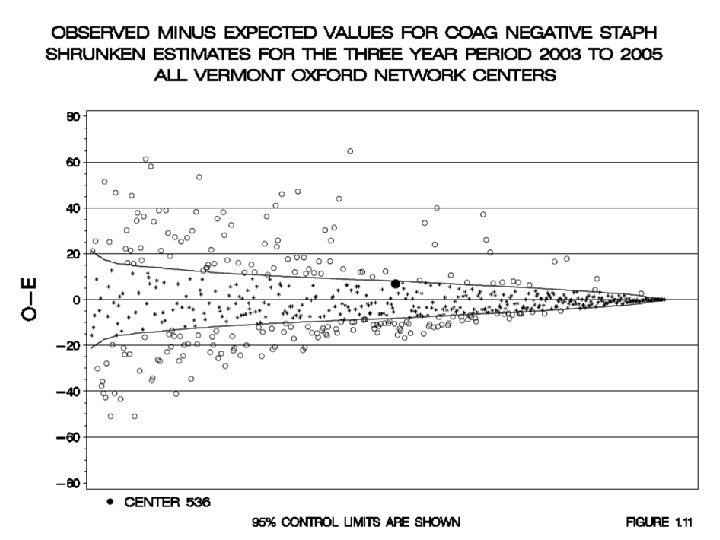
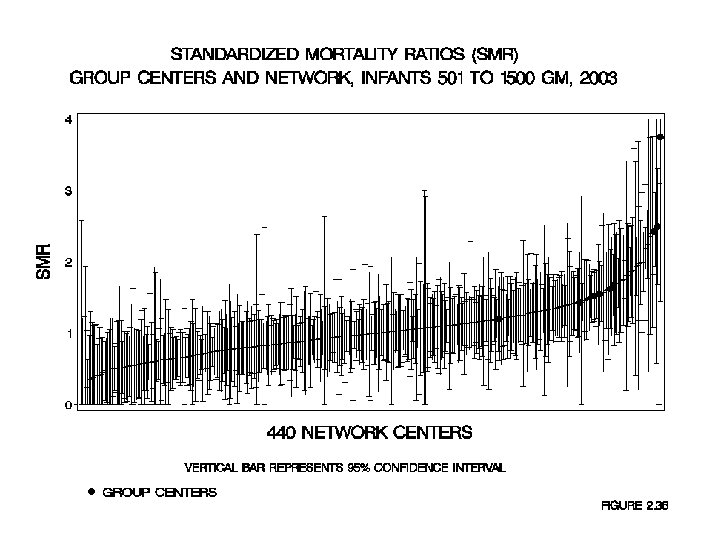
 • The SMR is the ratio of the number of") Standardised Mortality/Morbidity Ratio (SMR) • The SMR is the ratio of the number of observed cases (O) to the number of expected cases (E), where the number of expected cases is based on a multivariable risk adjustment model. • Each of the SMRs and confidence intervals have been corrected or “shrunken” using methods which recognize that some of the observed variation is random “noise”, particularly for small hospitals. The shrunken values are more stable estimates because they are adjusted for imprecise estimates (small N’s) and filter random variation.
Standardised Mortality/Morbidity Ratio (SMR) • The SMR is the ratio of the number of observed cases (O) to the number of expected cases (E), where the number of expected cases is based on a multivariable risk adjustment model. • Each of the SMRs and confidence intervals have been corrected or “shrunken” using methods which recognize that some of the observed variation is random “noise”, particularly for small hospitals. The shrunken values are more stable estimates because they are adjusted for imprecise estimates (small N’s) and filter random variation.
 Standardised Ratios • PREDICTED RATE – is calculated using a multivariable logistic regression model developed by analyzing infants from all Network centres. • Infant characteristics used as variables in the regression equation to calculate predicted values include: – – – – GESTATIONAL AGE (completed weeks) and its squared term, SMALL FOR GESTATIONAL AGE, MULTIPLE BIRTH, 1 MINUTE APGAR SCORE, SEX, RACE, LOCATION OF BIRTH (inborn or outborn) MODE OF DELIVERY (vaginal or c-section) CONGENITAL MALFORMATION • ordered categories from most life threatening to least life threatening.
Standardised Ratios • PREDICTED RATE – is calculated using a multivariable logistic regression model developed by analyzing infants from all Network centres. • Infant characteristics used as variables in the regression equation to calculate predicted values include: – – – – GESTATIONAL AGE (completed weeks) and its squared term, SMALL FOR GESTATIONAL AGE, MULTIPLE BIRTH, 1 MINUTE APGAR SCORE, SEX, RACE, LOCATION OF BIRTH (inborn or outborn) MODE OF DELIVERY (vaginal or c-section) CONGENITAL MALFORMATION • ordered categories from most life threatening to least life threatening.
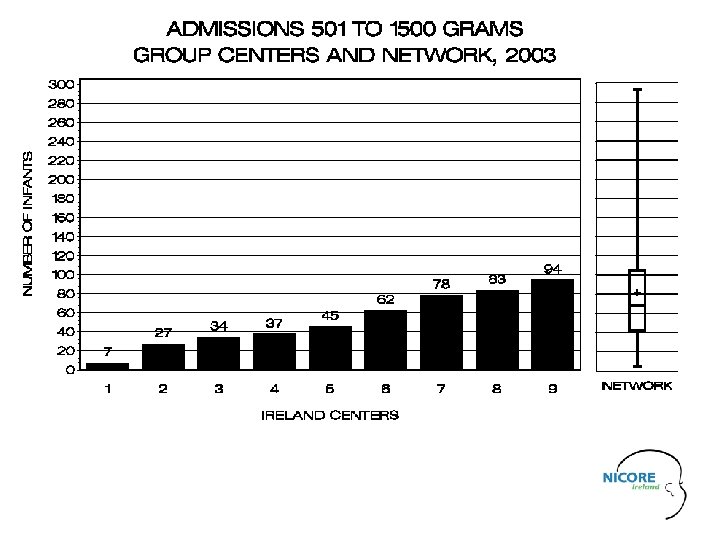
 VLBW Admissions Ireland 2004
VLBW Admissions Ireland 2004
 VLBW Admissions Ireland 2005
VLBW Admissions Ireland 2005
 A B C D E") Standardised Mortality Ratios 2003 CENTER (95% C. I. ) A B C D E F G H I 2. 5 1. 2 2. 4 1. 6 1. 7 1. 5 1. 6 3. 8 1. 4 (1. 7, 3. 3) (0. 6, 1. 8) (1. 8, 3. 0) (1. 1, 2. 2) (1. 2, 2. 1)) (1. 2, 1. 9) (1. 1, 2. 0) (1. 4, 6. 1) (0. 7, 2. 1)
Standardised Mortality Ratios 2003 CENTER (95% C. I. ) A B C D E F G H I 2. 5 1. 2 2. 4 1. 6 1. 7 1. 5 1. 6 3. 8 1. 4 (1. 7, 3. 3) (0. 6, 1. 8) (1. 8, 3. 0) (1. 1, 2. 2) (1. 2, 2. 1)) (1. 2, 1. 9) (1. 1, 2. 0) (1. 4, 6. 1) (0. 7, 2. 1)
 Standardised Mortality Ratios Ireland 2004
Standardised Mortality Ratios Ireland 2004
 Standardised Mortality Ratios Ireland 2005
Standardised Mortality Ratios Ireland 2005
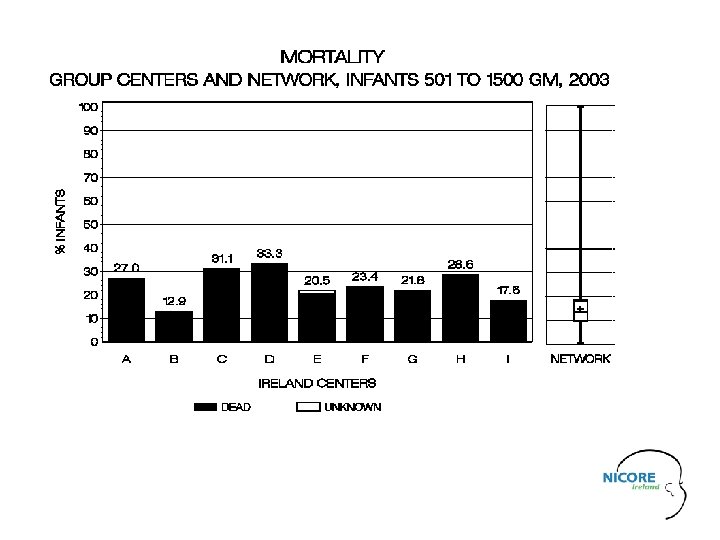
 Mortality 2004
Mortality 2004
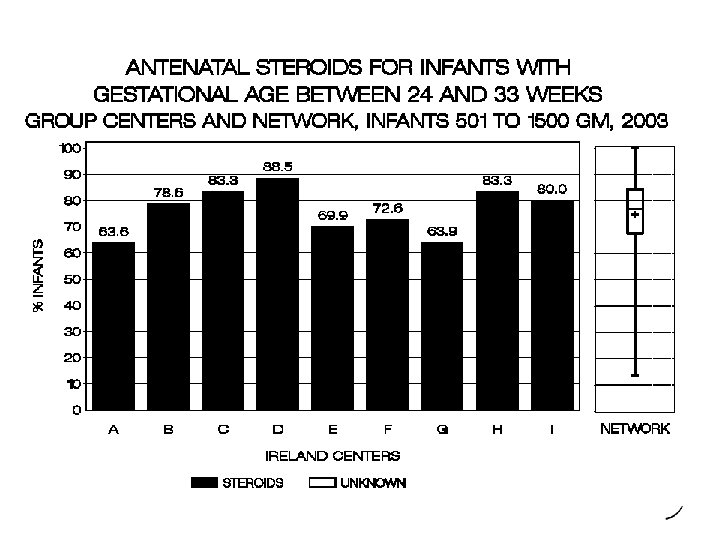
 Antenatal Corticosteroids 2004
Antenatal Corticosteroids 2004
 Antenatal Corticosteroids 2005
Antenatal Corticosteroids 2005
 SURVIVAL WITH NO KNOWN MORBIDITY AND MORBIDITY AMONG SURVIVORS 2003 Ireland n=9 N=467 % Survival with no known morbidity 77 Morbidities CLD SEVERE IVH PVL NEC PNEUMOTHORAX ANY LATE INFECTION ONE OR MORE MORBIDITY VON n= 442 N=35, 165 %(quartiles) 85 (81, 90) 43 11 4 2 6 3 25 44 47 (40, 55) 27 (15, 33) 6 (3, 9) 3 (0, 4) 5 (1, 6) 3 (1, 5) 20 (11, 26) 45 (36, 52)
SURVIVAL WITH NO KNOWN MORBIDITY AND MORBIDITY AMONG SURVIVORS 2003 Ireland n=9 N=467 % Survival with no known morbidity 77 Morbidities CLD SEVERE IVH PVL NEC PNEUMOTHORAX ANY LATE INFECTION ONE OR MORE MORBIDITY VON n= 442 N=35, 165 %(quartiles) 85 (81, 90) 43 11 4 2 6 3 25 44 47 (40, 55) 27 (15, 33) 6 (3, 9) 3 (0, 4) 5 (1, 6) 3 (1, 5) 20 (11, 26) 45 (36, 52)
 SURVIVAL WITH NO KNOWN MORBIDITY AND MORBIDITY AMONG SURVIVORS 2004 NICORE n=14 N=467 % Survival with no known morbidity 42 (↓) Morbidities CLD SEVERE IVH PVL NEC PNEUMOTHORAX ANY LATE INFECTION ONE OR MORE MORBIDITY VON n= 504 N=38, 895 %(quartiles) 81 ( ) 85 (82, 90) 17 ( ) 7 ( ) 4 ( ) 5 (↓) 3 ( ) 30 ( ) 48 ( ) 49 (42, 59) 25 (14, 31) 6 (2, 8) 3 (0, 4) 4 (0, 6) 3 (1, 5) 20 (10, 26) 43 (32, 50)
SURVIVAL WITH NO KNOWN MORBIDITY AND MORBIDITY AMONG SURVIVORS 2004 NICORE n=14 N=467 % Survival with no known morbidity 42 (↓) Morbidities CLD SEVERE IVH PVL NEC PNEUMOTHORAX ANY LATE INFECTION ONE OR MORE MORBIDITY VON n= 504 N=38, 895 %(quartiles) 81 ( ) 85 (82, 90) 17 ( ) 7 ( ) 4 ( ) 5 (↓) 3 ( ) 30 ( ) 48 ( ) 49 (42, 59) 25 (14, 31) 6 (2, 8) 3 (0, 4) 4 (0, 6) 3 (1, 5) 20 (10, 26) 43 (32, 50)
 SURVIVAL WITH NO KNOWN MORBIDITY AND MORBIDITY AMONG SURVIVORS 2005 NICORE n=14 N=769 % 82 ( ) Survival with no known morbidity Morbidities CLD SEVERE IVH PVL NEC PNEUMOTHORAX ANY LATE INFECTION ONE OR MORE MORBIDITY VON n= 557 N=42, 937 %(quartiles) 86 (82, 90) 46 ( ) 49 (42, 60) 18 ( ) 6 (↓) 2 (↓) 6 ( ) 2 (↓) 30 ( ) 44 (↓) 26 (13, 31) 6 (2, 8) 3 (0, 4) 5 (2, 7) 3 (0, 5) 20 (10, 25) 43 (32, 50)
SURVIVAL WITH NO KNOWN MORBIDITY AND MORBIDITY AMONG SURVIVORS 2005 NICORE n=14 N=769 % 82 ( ) Survival with no known morbidity Morbidities CLD SEVERE IVH PVL NEC PNEUMOTHORAX ANY LATE INFECTION ONE OR MORE MORBIDITY VON n= 557 N=42, 937 %(quartiles) 86 (82, 90) 46 ( ) 49 (42, 60) 18 ( ) 6 (↓) 2 (↓) 6 ( ) 2 (↓) 30 ( ) 44 (↓) 26 (13, 31) 6 (2, 8) 3 (0, 4) 5 (2, 7) 3 (0, 5) 20 (10, 25) 43 (32, 50)
 The Model for Improvement What are we trying to accomplish? How will we know a change is an improvement ? What change can we make that will result in improvement? Act Study Plan Aim Measures Change CYCLES for Testing and Implementing Change Do Langley, Nolan, Norman, Provost; Improvement Guide, 1996
The Model for Improvement What are we trying to accomplish? How will we know a change is an improvement ? What change can we make that will result in improvement? Act Study Plan Aim Measures Change CYCLES for Testing and Implementing Change Do Langley, Nolan, Norman, Provost; Improvement Guide, 1996
 Repeated Use of the Cycle TA A D S Evidence Theories Ideas A P S D A D D S P A A P S D Changes That Result in Improvement Increasing --complexity number of people different situations. . . P Time
Repeated Use of the Cycle TA A D S Evidence Theories Ideas A P S D A D D S P A A P S D Changes That Result in Improvement Increasing --complexity number of people different situations. . . P Time
 Vermont Oxford Network 4 Key Habits Habit for Change Habit for Evidence Based Practice BETTER PRACTICES Clinical Organizational Operational Habit for Collaborative Learning Habit for Systems Thinking
Vermont Oxford Network 4 Key Habits Habit for Change Habit for Evidence Based Practice BETTER PRACTICES Clinical Organizational Operational Habit for Collaborative Learning Habit for Systems Thinking
 i. NICQ 2005 Collaborative April June July Sept Intro HH CVL Bundle Nov Abx Use Case Studies Faculty Coaching A P S D Conference Calls Email Discussion List
i. NICQ 2005 Collaborative April June July Sept Intro HH CVL Bundle Nov Abx Use Case Studies Faculty Coaching A P S D Conference Calls Email Discussion List
 i. NICQ Encephalopathy Series 2006 Jan Intro Feb April Cooling EEG/a. EEG June Sept Imaging F/U Families Prework before each session 30 minute work time Email Discussion List
i. NICQ Encephalopathy Series 2006 Jan Intro Feb April Cooling EEG/a. EEG June Sept Imaging F/U Families Prework before each session 30 minute work time Email Discussion List
 Progress to Date • Southern Ireland Group Report produced on VLBW infants in 2003 and All Ireland Group Report in 2004 & 2005. • Data submitted for 2006 and membership subscription and data collection ongoing for 2007 • Benchmarking neonatal intensive care services with defined professional standards nationally and internationally
Progress to Date • Southern Ireland Group Report produced on VLBW infants in 2003 and All Ireland Group Report in 2004 & 2005. • Data submitted for 2006 and membership subscription and data collection ongoing for 2007 • Benchmarking neonatal intensive care services with defined professional standards nationally and internationally
 Progress to Date • Collaborative Guideline production by Neonatal Subcommittee of Faculty of Paediatrics commenced in response to Ireland Annual Group Report • Enrolment of 9 units in South in VON i. NICQ projects, aiming to reduce nosocomial infection in 2005 and focussing on neonatal encephalopathy in 2006 • 4 largest units in South in expanded database and VON Encephalopathy Registry in 2006
Progress to Date • Collaborative Guideline production by Neonatal Subcommittee of Faculty of Paediatrics commenced in response to Ireland Annual Group Report • Enrolment of 9 units in South in VON i. NICQ projects, aiming to reduce nosocomial infection in 2005 and focussing on neonatal encephalopathy in 2006 • 4 largest units in South in expanded database and VON Encephalopathy Registry in 2006
 Future Plans • National Perinatal Epidemiology Centre planned by DOHC to open in Cork University Maternity Hospital 2007 • Ireland Group Representation at Annual VON Quality Congress each December • Collaboration with UK VON Network
Future Plans • National Perinatal Epidemiology Centre planned by DOHC to open in Cork University Maternity Hospital 2007 • Ireland Group Representation at Annual VON Quality Congress each December • Collaboration with UK VON Network
 Future Plans • Build Links with EURONEOSTAT on all Ireland basis. EURONEOSTAT has submitted project proposal and requested funding from the European Commission • National Data for Neonatal Subcommittee and Faculty of Paediatrics for informed decision making regarding neonatal intensive care services in Ireland
Future Plans • Build Links with EURONEOSTAT on all Ireland basis. EURONEOSTAT has submitted project proposal and requested funding from the European Commission • National Data for Neonatal Subcommittee and Faculty of Paediatrics for informed decision making regarding neonatal intensive care services in Ireland
 Welcome, B. P. Murphy, MD Summaries | Workspace | Admin Tools | Options | Help | Log Out
Welcome, B. P. Murphy, MD Summaries | Workspace | Admin Tools | Options | Help | Log Out
 GA Week Cases/N < 22 Weeks 0/1 23 0/0 24 0/3 25") Center (2007) GA Week Cases/N < 22 Weeks 0/1 23 0/0 24 0/3 25 % 0/0 22 Network (2005) N % (Q 1, Q 3) 0 0. 0% 1, 005 5. 4% (0. 0%, 0. 0%) 1, 964 29. 9% (0. 0%, 50. 0%) 0. 0% 3, 309 55. 4% (33. 3%, 75. 0%) 1/2 50. 0% 3, 641 72. 6% (60. 0%, 100. 0%) 26 0/1 0. 0% 4, 283 81. 9% (71. 7%, 100. 0%) 27 5/5 100. 0% 4, 837 88. 3% (83. 3%, 100. 0%) 28 2/2 100. 0% 5, 468 92. 3% (87. 0%, 100. 0%) 29 4/4 100. 0% 6, 227 94. 7% (91. 7%, 100. 0%)
Center (2007) GA Week Cases/N < 22 Weeks 0/1 23 0/0 24 0/3 25 % 0/0 22 Network (2005) N % (Q 1, Q 3) 0 0. 0% 1, 005 5. 4% (0. 0%, 0. 0%) 1, 964 29. 9% (0. 0%, 50. 0%) 0. 0% 3, 309 55. 4% (33. 3%, 75. 0%) 1/2 50. 0% 3, 641 72. 6% (60. 0%, 100. 0%) 26 0/1 0. 0% 4, 283 81. 9% (71. 7%, 100. 0%) 27 5/5 100. 0% 4, 837 88. 3% (83. 3%, 100. 0%) 28 2/2 100. 0% 5, 468 92. 3% (87. 0%, 100. 0%) 29 4/4 100. 0% 6, 227 94. 7% (91. 7%, 100. 0%)
 critical care patient management Cork University Maternity Hospital Neonatal Unit
critical care patient management Cork University Maternity Hospital Neonatal Unit
