aa6f3e32b3f5bdf50260ec7b56e16f1c.ppt
- Количество слайдов: 27
 NEFROLOGISK KLINIK P, RIGSHOSPITALET Grounds with case presentations Nordic Society of Nephrology 34 th Biennal Congress Malmö Sept 22 nd 2017 Wladimir Szpirt Department of Nephrology Rigshospitalet, Copenhagen, Denmark
NEFROLOGISK KLINIK P, RIGSHOSPITALET Grounds with case presentations Nordic Society of Nephrology 34 th Biennal Congress Malmö Sept 22 nd 2017 Wladimir Szpirt Department of Nephrology Rigshospitalet, Copenhagen, Denmark
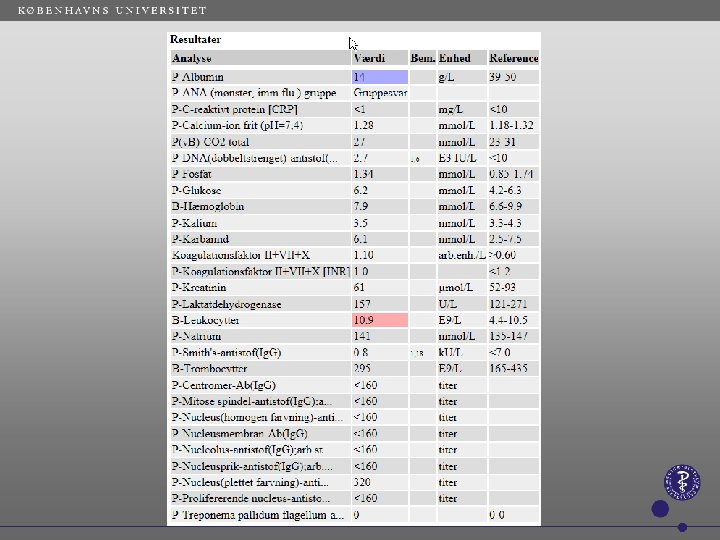
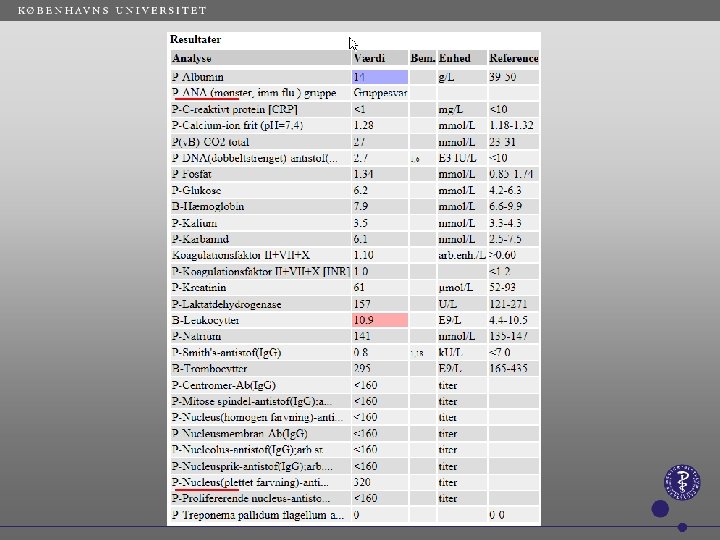
 17 yrs. old boy admitted by GP in April 2017 for nephrotic syndrome. We found normal creatinine, proteinuria 10 g/day, albumin 14 g/L. During childhood many infections especially respiratory, was coughing, had 2 x hemoptysis, After parkourt training legs swallowing for 1 month.
17 yrs. old boy admitted by GP in April 2017 for nephrotic syndrome. We found normal creatinine, proteinuria 10 g/day, albumin 14 g/L. During childhood many infections especially respiratory, was coughing, had 2 x hemoptysis, After parkourt training legs swallowing for 1 month.
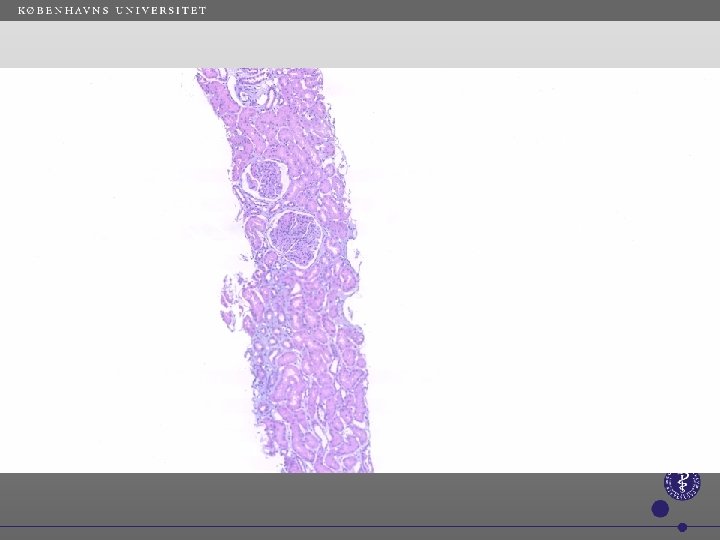
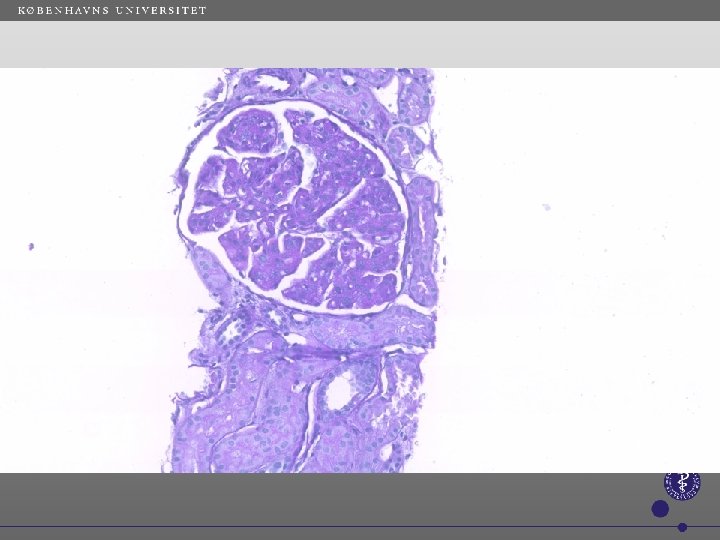
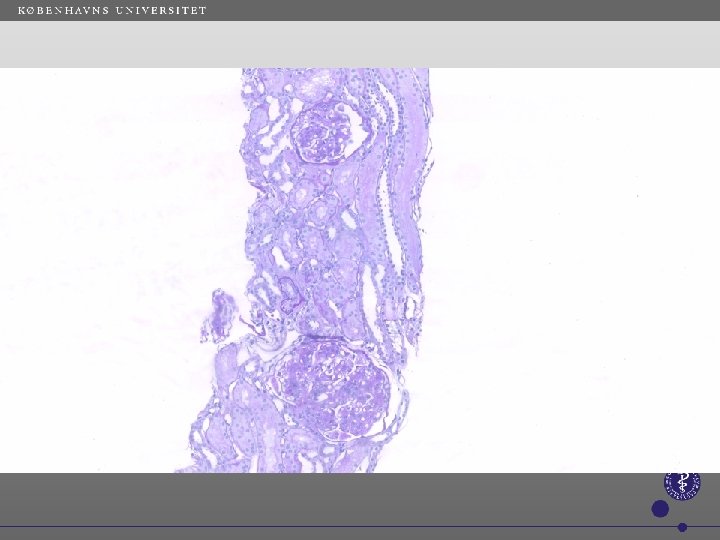
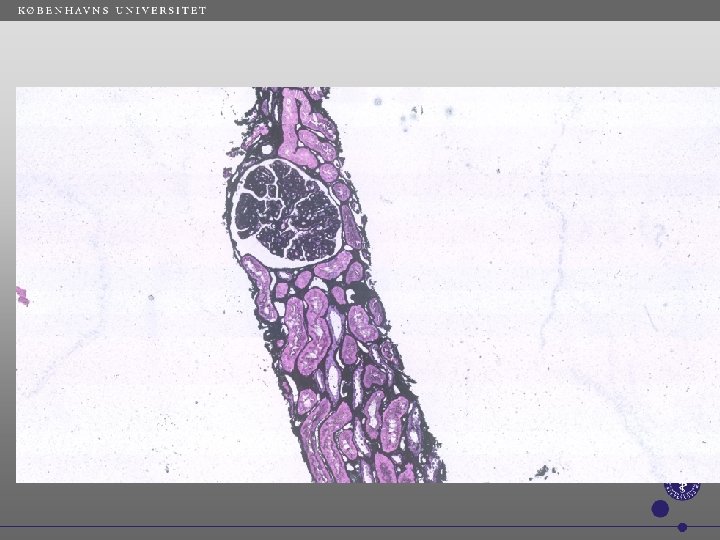
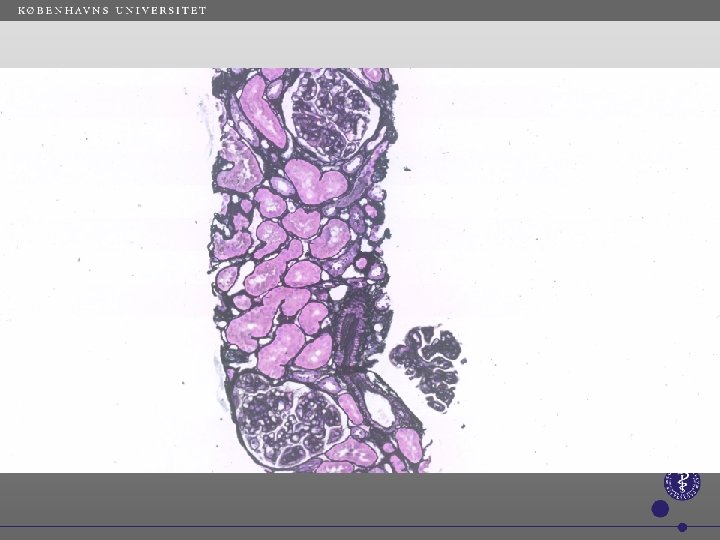
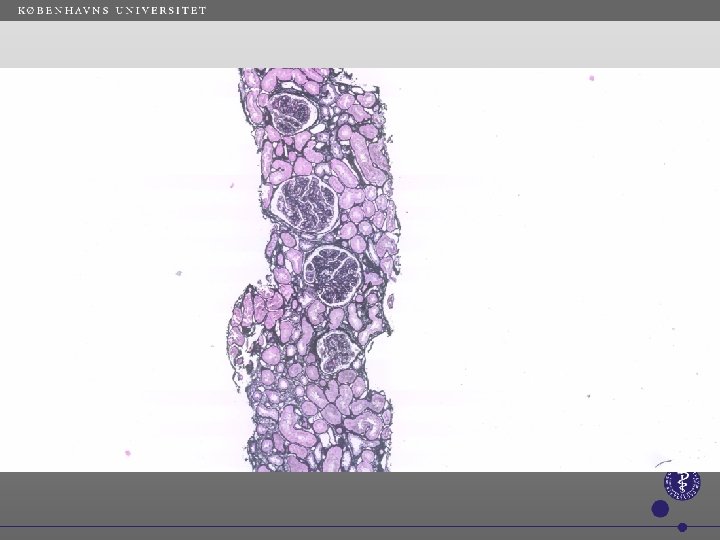
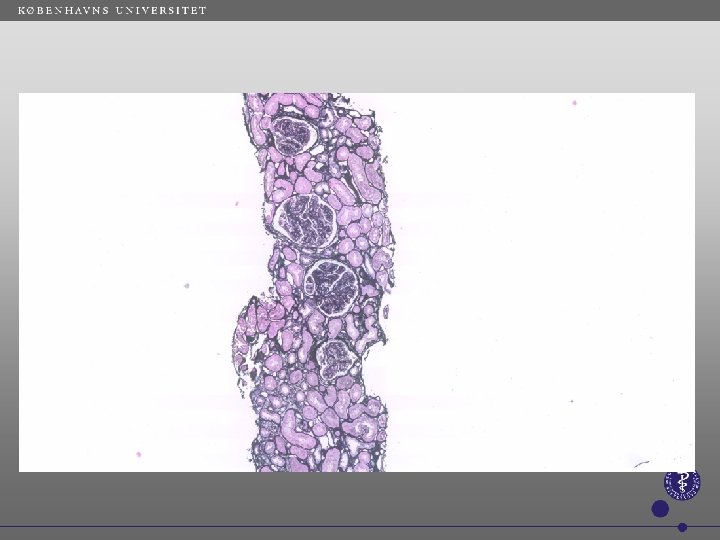
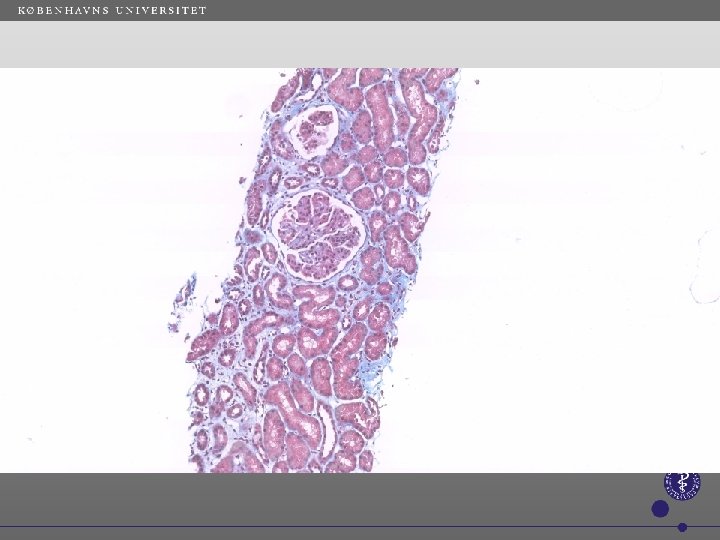
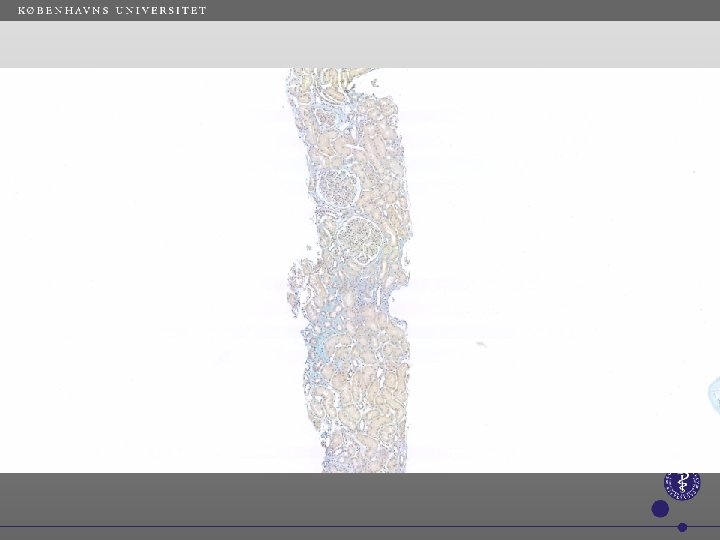
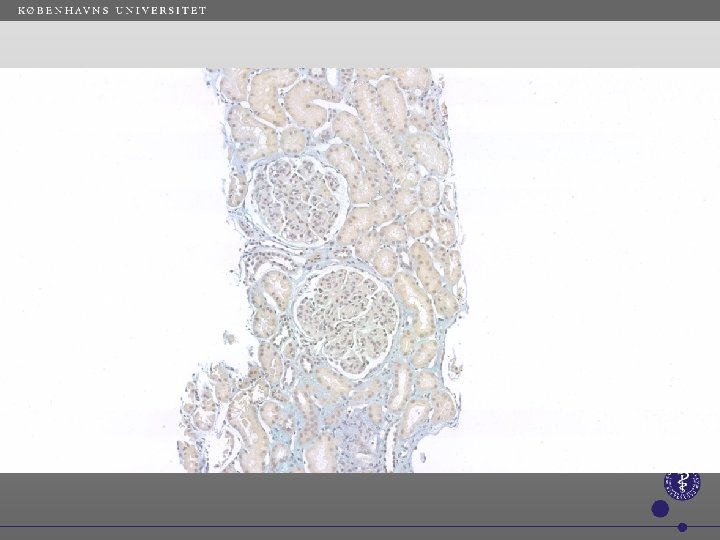
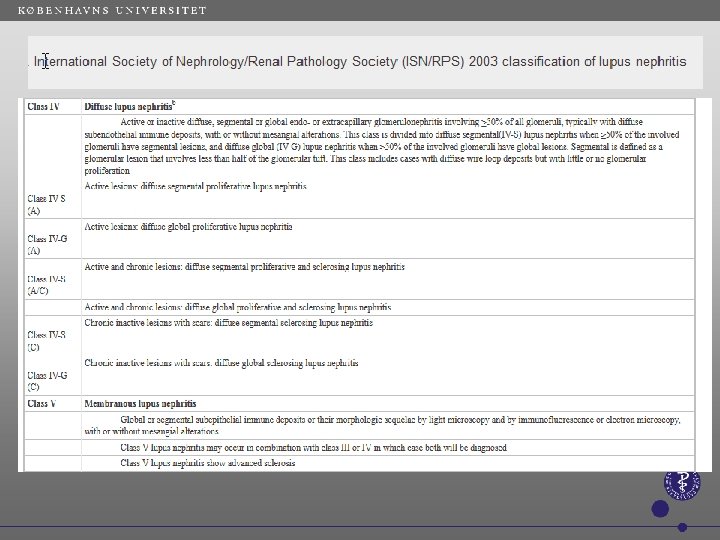
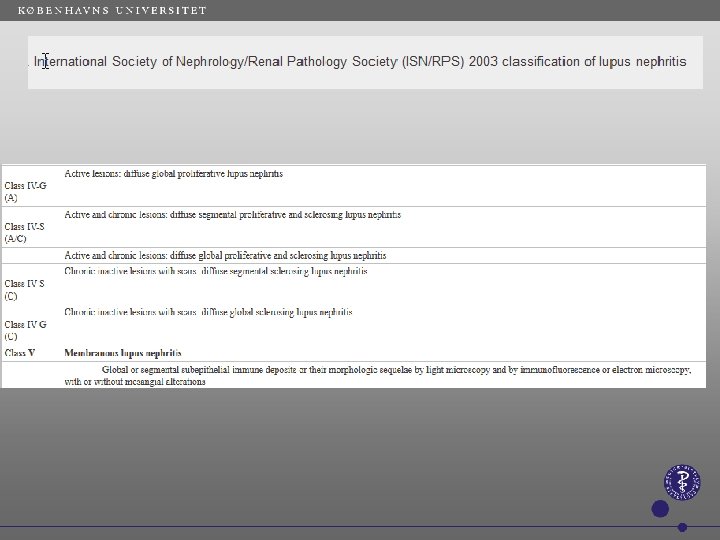
 Renal biopsy & lab. tests a. Immune complex mediated membrano proliferative GN with membranous component and SLE like nephritis, class IV-G + class V, full-house deposits of immunglobulins. b. 2 positive results for ANA. negative for anti-DNA & anti-Sm antibody. c. Low blood concentration of C 3. d. DAT neg. No lymphopenia. a. Neg. Hepatitis B & C, HIV b. Neg. anti-phosplipase A 2 receptor Abs (PLA-2 R) c.
Renal biopsy & lab. tests a. Immune complex mediated membrano proliferative GN with membranous component and SLE like nephritis, class IV-G + class V, full-house deposits of immunglobulins. b. 2 positive results for ANA. negative for anti-DNA & anti-Sm antibody. c. Low blood concentration of C 3. d. DAT neg. No lymphopenia. a. Neg. Hepatitis B & C, HIV b. Neg. anti-phosplipase A 2 receptor Abs (PLA-2 R) c.
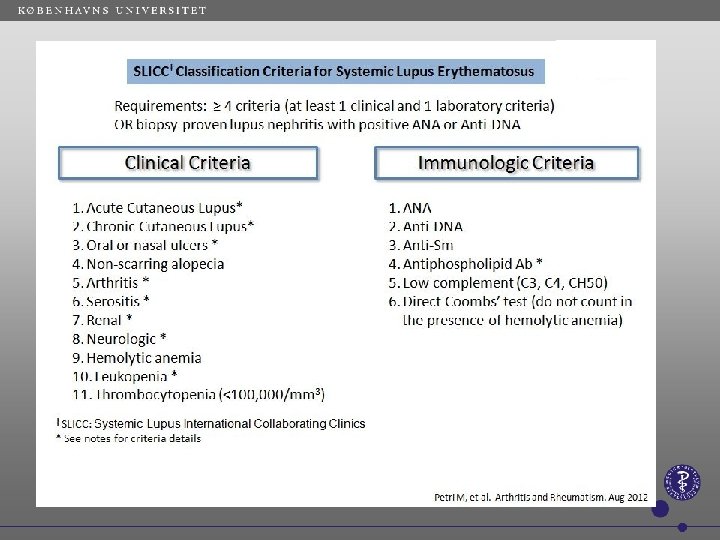
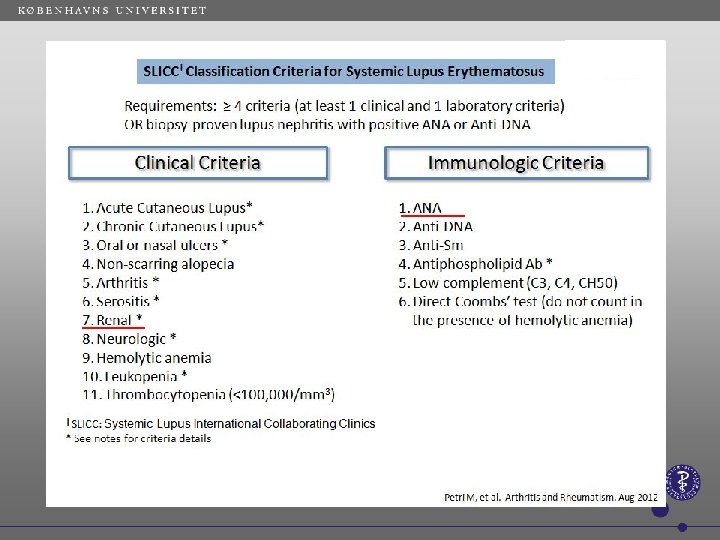
 Diagnostic evaluation: SLE based on SLICC: 1. Renal biopsy SLE 2. ANA-positive. 3. Low C 3 Extra renal: no other symptoms from cardio-pulmonal, no athralgias or myalgias, no photosensitivity, no skin symptoms, no mucous ulcerations. Look for immune defect as he had spontanous low Ig G, has normal B-T- cells and MBL (mannose binding lectin)
Diagnostic evaluation: SLE based on SLICC: 1. Renal biopsy SLE 2. ANA-positive. 3. Low C 3 Extra renal: no other symptoms from cardio-pulmonal, no athralgias or myalgias, no photosensitivity, no skin symptoms, no mucous ulcerations. Look for immune defect as he had spontanous low Ig G, has normal B-T- cells and MBL (mannose binding lectin)
 Plasma creatinine april – september 2017
Plasma creatinine april – september 2017
 Albumin in G/L during immunosupression
Albumin in G/L during immunosupression
 Proteinuria in g/d during immunosuppression
Proteinuria in g/d during immunosuppression
 Diagnosis based on biopsy. Typically proteinuria up to nephrotic") Membrano proliferative GN (MPGN) Diagnosis based on biopsy. Typically proteinuria up to nephrotic syndrome. Creatinine can be increased. Before type I-III based on electron microscopy. Now new classification based on immune deposits - not seen in our pt. Immune complex mediated MPGN Ig. G & complement complexes in biopsy, low C 4 and low/normal C 3 in blood. Can be primary (idiopatic) or more often secundary to autoimmun sygdom (SLE, RA or Sjøgrens), infection (hepatitis B/C, endocarditis, shunt nephritis, abscesses) Malignancy (typically plasmatic cell diseases) Complement mediated MPGN (C 3 G) Deposition of C 3 i glomerula with or without Ig-deposition. MPGN without Ig/complement Rare typically secondary to chronic MPA, Prothrombotic conditions transplant glomerulopathies
Membrano proliferative GN (MPGN) Diagnosis based on biopsy. Typically proteinuria up to nephrotic syndrome. Creatinine can be increased. Before type I-III based on electron microscopy. Now new classification based on immune deposits - not seen in our pt. Immune complex mediated MPGN Ig. G & complement complexes in biopsy, low C 4 and low/normal C 3 in blood. Can be primary (idiopatic) or more often secundary to autoimmun sygdom (SLE, RA or Sjøgrens), infection (hepatitis B/C, endocarditis, shunt nephritis, abscesses) Malignancy (typically plasmatic cell diseases) Complement mediated MPGN (C 3 G) Deposition of C 3 i glomerula with or without Ig-deposition. MPGN without Ig/complement Rare typically secondary to chronic MPA, Prothrombotic conditions transplant glomerulopathies
 C 1 q C 3 c
C 1 q C 3 c
 C 4 c Ig. G Ig. A Ig. M
C 4 c Ig. G Ig. A Ig. M
 kappa lambda
kappa lambda