

thomashyde-110614154412-phpapp02.pptx
- Количество слайдов: 115
") National University of Health Sciences Thomas E. Hyde, DC, DACBSP, CSTI, ICSSD, FRCCSS (Hon)
National University of Health Sciences Thomas E. Hyde, DC, DACBSP, CSTI, ICSSD, FRCCSS (Hon)
 How about an adjustment?
How about an adjustment?
 Don’t be afraid to jump into the unknown….
Don’t be afraid to jump into the unknown….
 El Misti 08/05 Summit being treated by Greg Doerr, DC at 19, 223 feet
El Misti 08/05 Summit being treated by Greg Doerr, DC at 19, 223 feet
 Objectives of this lecture • Teach you something new to consider using in your practice • Not to teach you to be an expert by the end of the lecture • Stimulate you to learn more • To provide you options to better treat your patients
Objectives of this lecture • Teach you something new to consider using in your practice • Not to teach you to be an expert by the end of the lecture • Stimulate you to learn more • To provide you options to better treat your patients
 Objectives of this lecture • Teach you something new to consider using in your practice • Not to teach you to be an expert by the end of the lecture • Stimulate you to learn more • To provide you options to better treat your patients
Objectives of this lecture • Teach you something new to consider using in your practice • Not to teach you to be an expert by the end of the lecture • Stimulate you to learn more • To provide you options to better treat your patients
 Before Treatment Begins 1. Take a complete history 2. Perform a complete examination 3. Make your best clinical decision regarding whether you feel your diagnosis for this patient would be best served by you treating them with whatever technique/s you employ 4. If not, refer to someone you feel would be more likely to help them
Before Treatment Begins 1. Take a complete history 2. Perform a complete examination 3. Make your best clinical decision regarding whether you feel your diagnosis for this patient would be best served by you treating them with whatever technique/s you employ 4. If not, refer to someone you feel would be more likely to help them
 Buttler Never Flossing") Soft Tissue Techniques Ø Ø Ø Ø Nimmo Cyriax Mattes (AIS) Buttler Never Flossing Myofascial Release Tech Active Release Tech ® Postisolation Relaxation Proprioceptive Neurolmuscular Facilitation (PNF) Stretching/gliding/pulling /pushing/compression Stecco Gua Sha Graston Technique® Sound Assisted Soft Tissue Technique ASTYM Rolfing Massage Strain Counterstrain Pin and Stretch Mulligan Functional Position Patterns by Gary Gray Muscle Energy Technique
Soft Tissue Techniques Ø Ø Ø Ø Nimmo Cyriax Mattes (AIS) Buttler Never Flossing Myofascial Release Tech Active Release Tech ® Postisolation Relaxation Proprioceptive Neurolmuscular Facilitation (PNF) Stretching/gliding/pulling /pushing/compression Stecco Gua Sha Graston Technique® Sound Assisted Soft Tissue Technique ASTYM Rolfing Massage Strain Counterstrain Pin and Stretch Mulligan Functional Position Patterns by Gary Gray Muscle Energy Technique
 Which Technique would you chose for these folks?
Which Technique would you chose for these folks?
 Lowe continues to state that when traumatized and inflamed, a fascial lesion heals by spider-webbing together with irregularly arranged collagen. Lowe
Lowe continues to state that when traumatized and inflamed, a fascial lesion heals by spider-webbing together with irregularly arranged collagen. Lowe
 Where fascia has been intermittently stressed, fibroblasts produce more linearly arranged collagen to reinforce the loaded myofascia. Chamberlain, GJ. “Cyriax’s frictionmassage: a review. ” JOSPT, 1082; 4: p 20
Where fascia has been intermittently stressed, fibroblasts produce more linearly arranged collagen to reinforce the loaded myofascia. Chamberlain, GJ. “Cyriax’s frictionmassage: a review. ” JOSPT, 1082; 4: p 20
 Muscle and fascia can’t be separated in that they function and dysfunction together. Where there is a tight muscle, there is usually tight fascia. Fascial-release techniques, then become important. John Lowe, Ma, DC
Muscle and fascia can’t be separated in that they function and dysfunction together. Where there is a tight muscle, there is usually tight fascia. Fascial-release techniques, then become important. John Lowe, Ma, DC
 Nimmo – lumbar spine
Nimmo – lumbar spine
 Nimmo - gluteals
Nimmo - gluteals
 Nimmo Anyone? ?
Nimmo Anyone? ?
 Race Track
Race Track
 Acu-Force Another instrument assisted from of soft tissue treatment. There are 4 instruments used in an attempt to break up fascial restriction. There a small and large star, an Sshaped instrument and a 7 pound larger Ishaped instrument
Acu-Force Another instrument assisted from of soft tissue treatment. There are 4 instruments used in an attempt to break up fascial restriction. There a small and large star, an Sshaped instrument and a 7 pound larger Ishaped instrument
 Acu-Force – forearm flexors
Acu-Force – forearm flexors
 Acu. Force
Acu. Force
 Acu-Force – trapezius/thoracic
Acu-Force – trapezius/thoracic
 Acu-Force – lumbar spine
Acu-Force – lumbar spine
 I always feel better after my Acu-Force treatment.
I always feel better after my Acu-Force treatment.
 Death Valley
Death Valley
 Cyriax Felt moving across the fibers at a right angle would not injure the normal healing tissue but would prevent the formation of or break down abnormal scar tissue. Hammer
Cyriax Felt moving across the fibers at a right angle would not injure the normal healing tissue but would prevent the formation of or break down abnormal scar tissue. Hammer
 Cyriax Stated TF moved the involved tissue while longitudinal friction affected the transportation of blood and lymph. Hammer
Cyriax Stated TF moved the involved tissue while longitudinal friction affected the transportation of blood and lymph. Hammer
 Cyriax In the acute phase, only necessary to use a light force In the chronic stages a deep, stronger friction is necessary. Hammer
Cyriax In the acute phase, only necessary to use a light force In the chronic stages a deep, stronger friction is necessary. Hammer
 Cyriax Friction creates anesthesia Usually within 3 minutes of friction, anesthesia begins
Cyriax Friction creates anesthesia Usually within 3 minutes of friction, anesthesia begins
 Cyriax – Shoulder - Knee
Cyriax – Shoulder - Knee
 Cyriax Elbow
Cyriax Elbow
 Cyriax can repair any damaged tissue
Cyriax can repair any damaged tissue

 1. Enhance proliferative invasion of vascular elements and fibroblasts followed by: 2. Collagen deposition and 3. Ultimate maturation. Nirschl RP, Ashman ES. Elbow tendinopathy: tennis elbow. Clin Sports Med 22 (2003):
1. Enhance proliferative invasion of vascular elements and fibroblasts followed by: 2. Collagen deposition and 3. Ultimate maturation. Nirschl RP, Ashman ES. Elbow tendinopathy: tennis elbow. Clin Sports Med 22 (2003):
 Increased collagen alone is not enough to heal a degenerated tendinosis Equally important is the correct orientation of the collagen fibers.
Increased collagen alone is not enough to heal a degenerated tendinosis Equally important is the correct orientation of the collagen fibers.
 Necessity of post treatment stretching & strengthening to provide the forces necessary for adaptive remodeling of new collagen in the affected areas. Exercise creates collagen alignment and stimulates collagen cross-linkage formation thereby improving tensile strength.
Necessity of post treatment stretching & strengthening to provide the forces necessary for adaptive remodeling of new collagen in the affected areas. Exercise creates collagen alignment and stimulates collagen cross-linkage formation thereby improving tensile strength.

 Superficial Posterior Spinal Fascial Lamina Barker PJ, Briggs CA. Attachments of the Posterior Layer of Lumbar Fascia. Spine 24 (17): 175764.
Superficial Posterior Spinal Fascial Lamina Barker PJ, Briggs CA. Attachments of the Posterior Layer of Lumbar Fascia. Spine 24 (17): 175764.
 Deep Posterior Spinal Lamina FUSION OF SUPERFICIAL & DEEP LAMINAE Barker PJ, Briggs CA. Attachments of the Posterior Layer of Lumbar Fascia. Spine 24 (17): 1757 -64. SERRATUS POSTERIOR INFERIOR GLUTEUS MEDIUS SACROTUBEROUS LIGAMENT
Deep Posterior Spinal Lamina FUSION OF SUPERFICIAL & DEEP LAMINAE Barker PJ, Briggs CA. Attachments of the Posterior Layer of Lumbar Fascia. Spine 24 (17): 1757 -64. SERRATUS POSTERIOR INFERIOR GLUTEUS MEDIUS SACROTUBEROUS LIGAMENT
 Lighthouse Tasmania
Lighthouse Tasmania
 New Research with IASTM During the Fascial Conference at Harvard in 2007, research emphasized that ALL types of soft tissue mechanical loading including exercise, injury, manual muscle treatments such as fascial release, stretching techniques, and IASTM act by affecting the fibroblasts. The fibroblasts are located within the ECM where repair, regeneration and maintenance of soft tissue takes place. Hammer W. April 2008
New Research with IASTM During the Fascial Conference at Harvard in 2007, research emphasized that ALL types of soft tissue mechanical loading including exercise, injury, manual muscle treatments such as fascial release, stretching techniques, and IASTM act by affecting the fibroblasts. The fibroblasts are located within the ECM where repair, regeneration and maintenance of soft tissue takes place. Hammer W. April 2008
 Hammer continued Use of light manual fascial methods stimulation of fibroblasts can respond with anti-inflammatory cytokines, growth factors and vasoactive compounds that underlie positive clinical outcomes. Standley showed how injury strains fibroblasts and fascia in negative ways while manual muscle treatment strains fibroblasts in curative ways. Hammer W. April 2008
Hammer continued Use of light manual fascial methods stimulation of fibroblasts can respond with anti-inflammatory cytokines, growth factors and vasoactive compounds that underlie positive clinical outcomes. Standley showed how injury strains fibroblasts and fascia in negative ways while manual muscle treatment strains fibroblasts in curative ways. Hammer W. April 2008
 Superficial Back Line Fascia Removed From Cadaver
Superficial Back Line Fascia Removed From Cadaver
 Superficial Back Line
Superficial Back Line
 Superficial Front Line
Superficial Front Line
 Lateral Line
Lateral Line
 Spiral Line
Spiral Line
 Arm Line
Arm Line
 Front And Back Functional Lines
Front And Back Functional Lines
 Deep Front Line
Deep Front Line
 What size and shape is your box? Are you willing to change that shape or size? What will you do differently tomorrow, next week, next year and each year thereafter?
What size and shape is your box? Are you willing to change that shape or size? What will you do differently tomorrow, next week, next year and each year thereafter?
 Is your box open or closed?
Is your box open or closed?

 FAKTR-PM Developed by: › Greg Doerr, DC, CCSP, CKTP › Tom Hyde. DC, DACBSP, CKTP, FCCSS (Hon) › Contributions by: Vince De. Bono, DC, CCSP, CSCS (KT Tape) Warren Hammer, DC, MS Dick Vincent, DC Shawn Burger, PT Mike Cicero, PT Mike Schneider, DC, Ph. D Phil Page, ATC, PT, Ph. D, CSCS Andre Labbe, PT Ed Feinberg, DC, CCSP Ted Forcum, DC, DACBSP Kay Pearce Donna Strachan
FAKTR-PM Developed by: › Greg Doerr, DC, CCSP, CKTP › Tom Hyde. DC, DACBSP, CKTP, FCCSS (Hon) › Contributions by: Vince De. Bono, DC, CCSP, CSCS (KT Tape) Warren Hammer, DC, MS Dick Vincent, DC Shawn Burger, PT Mike Cicero, PT Mike Schneider, DC, Ph. D Phil Page, ATC, PT, Ph. D, CSCS Andre Labbe, PT Ed Feinberg, DC, CCSP Ted Forcum, DC, DACBSP Kay Pearce Donna Strachan
 Functional and Kinetic Treatment with Rehab, Provocation and Motion. FAKTR-PM F - Functional and K - Kinetic T - Treatment with R - Rehab P - Provocation and M - Motion
Functional and Kinetic Treatment with Rehab, Provocation and Motion. FAKTR-PM F - Functional and K - Kinetic T - Treatment with R - Rehab P - Provocation and M - Motion
 Functional What activity causes a reproduction of the patient’s pain, loss or ROM, tightness, loss of function Is this with motion, without motion, active, passive, with resistance, without resistance What activity can you patient NOT do
Functional What activity causes a reproduction of the patient’s pain, loss or ROM, tightness, loss of function Is this with motion, without motion, active, passive, with resistance, without resistance What activity can you patient NOT do
 Kinetic Once the patient has been treated in the position of provocation with functional assessment, they are brought back to a nonpain producing position, then asked to assume the position of pain once more with functional testing. Many times, the pain will move up or down the kinetic chain – you now chase that pain.
Kinetic Once the patient has been treated in the position of provocation with functional assessment, they are brought back to a nonpain producing position, then asked to assume the position of pain once more with functional testing. Many times, the pain will move up or down the kinetic chain – you now chase that pain.
 Treatment is rendered in the position of provocation and with the function mechanism in play Treatment can be performed utilizing many different soft tissue modalities
Treatment is rendered in the position of provocation and with the function mechanism in play Treatment can be performed utilizing many different soft tissue modalities
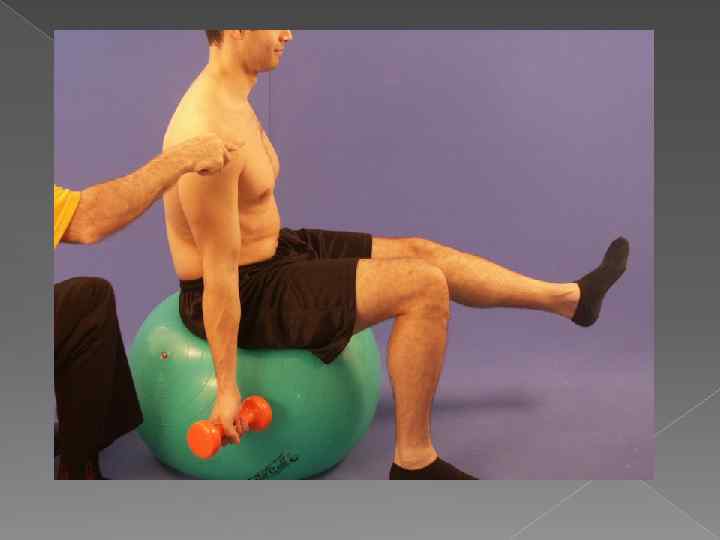
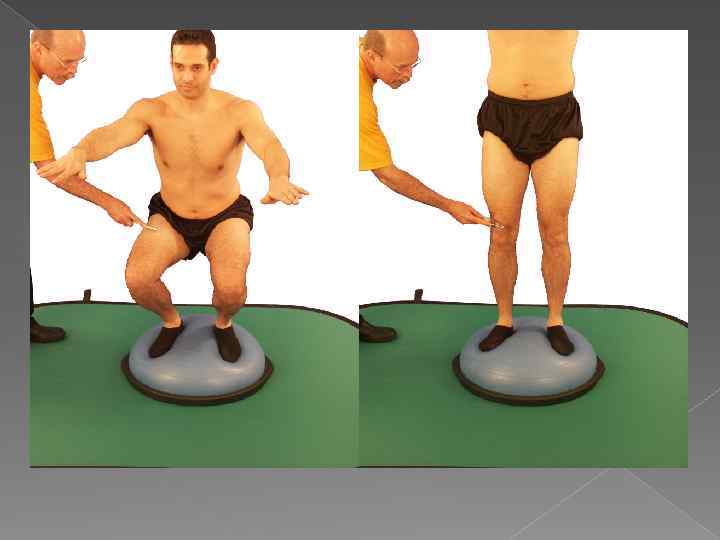
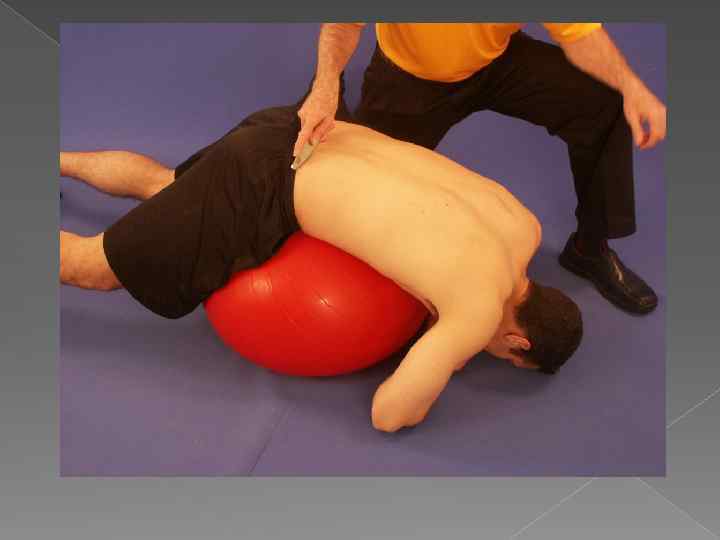
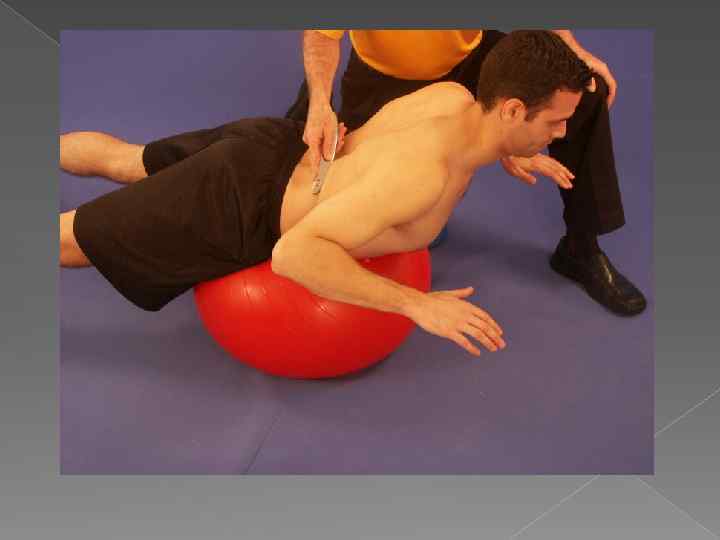
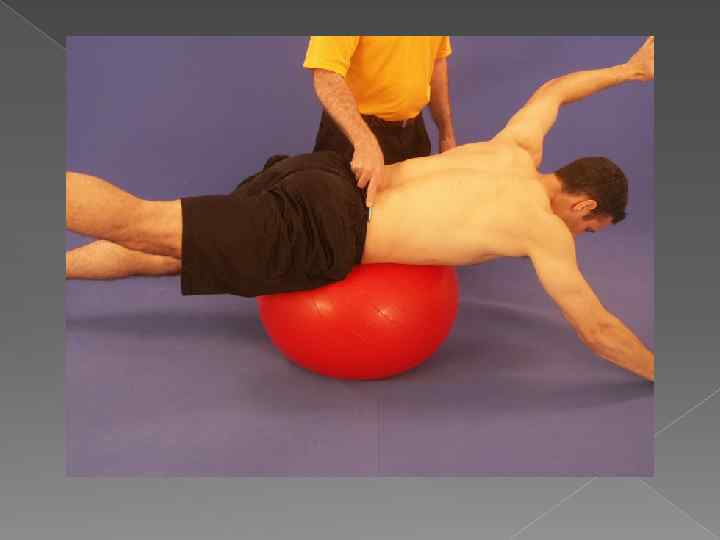
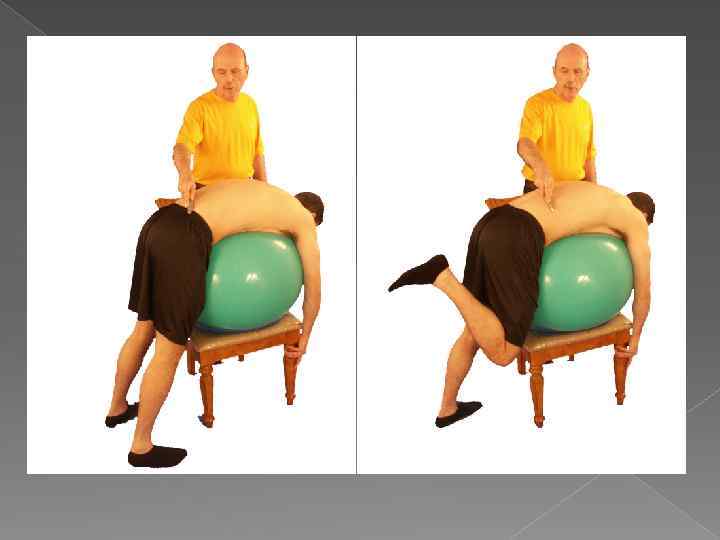
 This entails the use of many types of low tech rehab devices") Rehabilitation (Rehab) This entails the use of many types of low tech rehab devices such as the Swiss Ball, Both Sides Up (BOSU), balance pads and boards, tubing, Therabands, and more
Rehabilitation (Rehab) This entails the use of many types of low tech rehab devices such as the Swiss Ball, Both Sides Up (BOSU), balance pads and boards, tubing, Therabands, and more
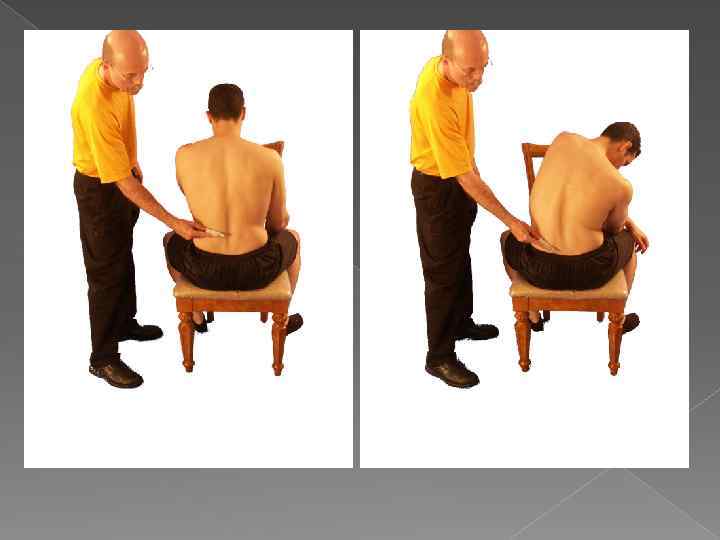
 Provocation The patient is asked to assume the position of provocation, that is the position that will reproduce their pain If the complaint is low back pain, you must determine if the pain is seated, standing, leaning, bending, etc This applies to any area of the body where pain is secondary to musculoskeletal disorders
Provocation The patient is asked to assume the position of provocation, that is the position that will reproduce their pain If the complaint is low back pain, you must determine if the pain is seated, standing, leaning, bending, etc This applies to any area of the body where pain is secondary to musculoskeletal disorders
 Motion What motion, if any, will reproduce the patient’s pain Consider treating the patient in motion such as low back pain brought on by getting up from a seated position for example
Motion What motion, if any, will reproduce the patient’s pain Consider treating the patient in motion such as low back pain brought on by getting up from a seated position for example
 Myofascial treatment has always worked for me.
Myofascial treatment has always worked for me.

 Gua Sha involves palpation and cutaneous stimulation where the skin is pressured, in strokes, by a round-edged instrument; that results in the appearance of small red petechiae called 'sha', that will fade in 2 to 3 days. http: //www. guasha. com/
Gua Sha involves palpation and cutaneous stimulation where the skin is pressured, in strokes, by a round-edged instrument; that results in the appearance of small red petechiae called 'sha', that will fade in 2 to 3 days. http: //www. guasha. com/
 Raising Sha removes blood stagnation considered pathogenic, promoting normal circulation and metabolic processes. The patient experiences immediate relief from pain, stiffness, fever, chill, cough, nausea, and so on. Gua Sha is valuable in the prevention and treatment of acute infectious illness, upper respiratory and digestive problems, and many other acute or chronic disorders.
Raising Sha removes blood stagnation considered pathogenic, promoting normal circulation and metabolic processes. The patient experiences immediate relief from pain, stiffness, fever, chill, cough, nausea, and so on. Gua Sha is valuable in the prevention and treatment of acute infectious illness, upper respiratory and digestive problems, and many other acute or chronic disorders.

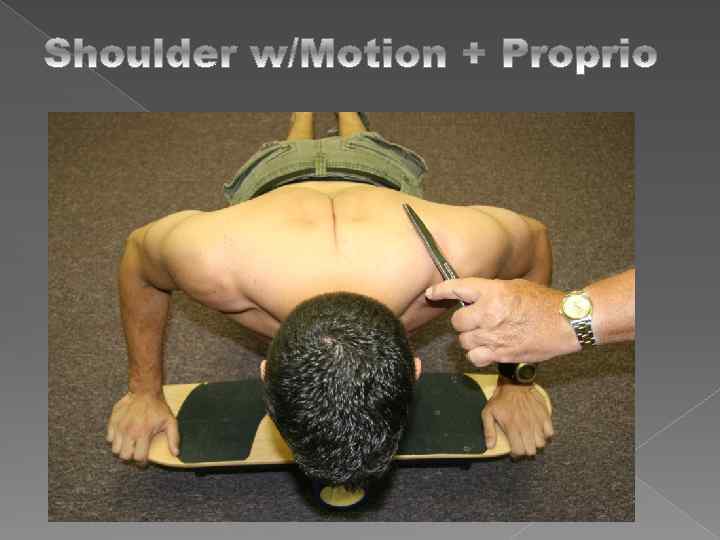
 Demonstration Shoulder Active Supraspinatus
Demonstration Shoulder Active Supraspinatus
 Isometric Supraspinatus
Isometric Supraspinatus
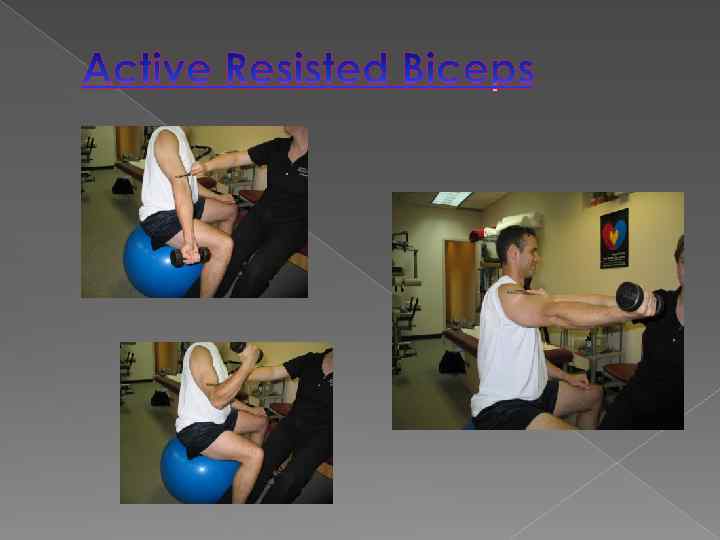
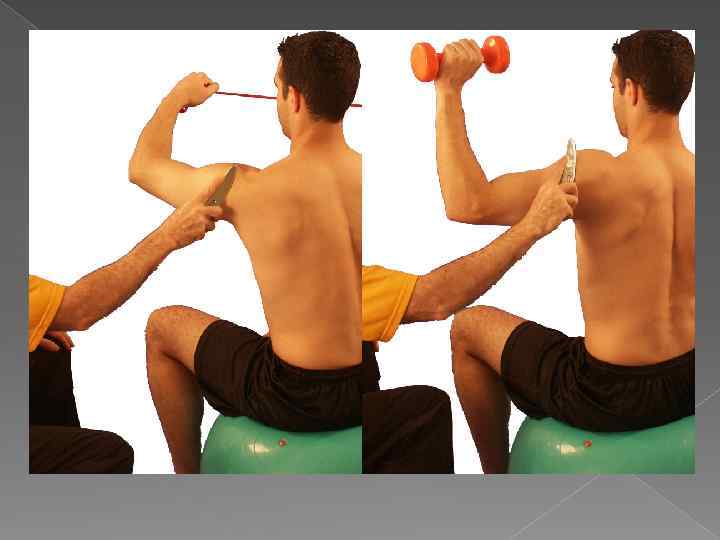
 Active Resisted Subscap
Active Resisted Subscap
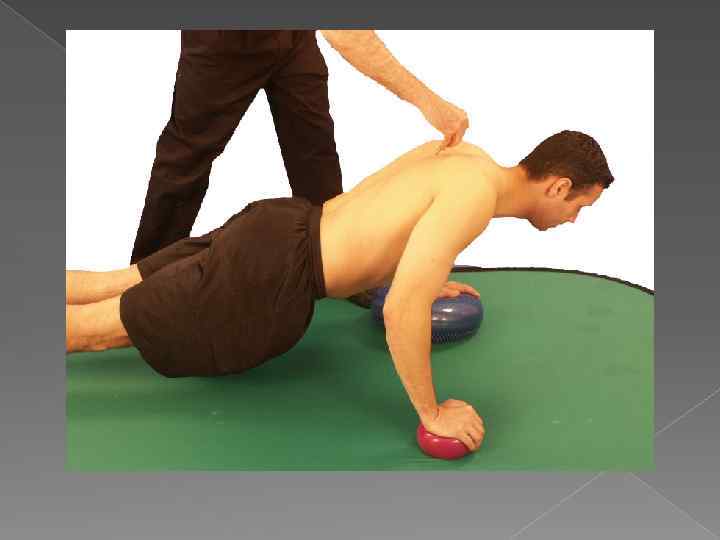
 Active Resisted Serratus
Active Resisted Serratus
 Active Resisted Scapular Stabilizers
Active Resisted Scapular Stabilizers
 Active Resisted Scapular Stabilizers
Active Resisted Scapular Stabilizers


 Knee Demonstration
Knee Demonstration
 Active Resisted Quad
Active Resisted Quad
 Quad, Patellar Tendon with Ball Squat
Quad, Patellar Tendon with Ball Squat
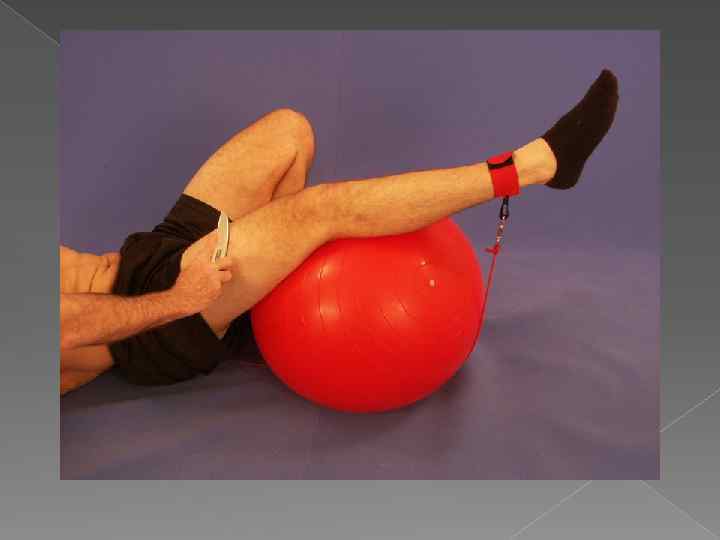

 QUAD JUMPERS
QUAD JUMPERS
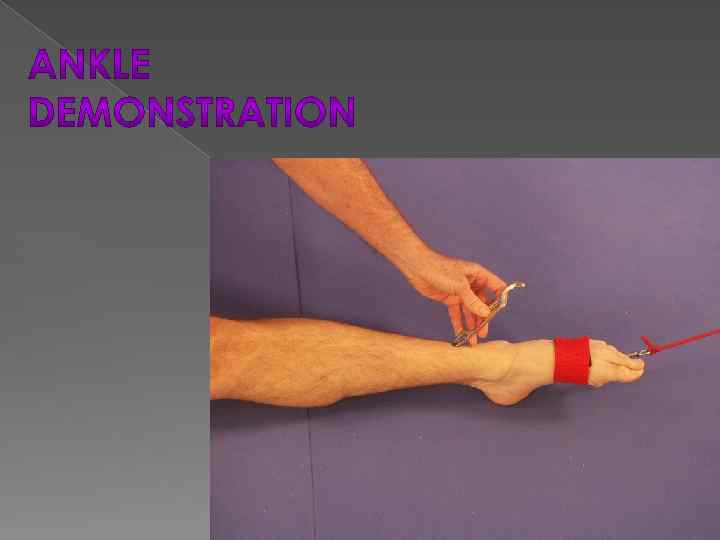
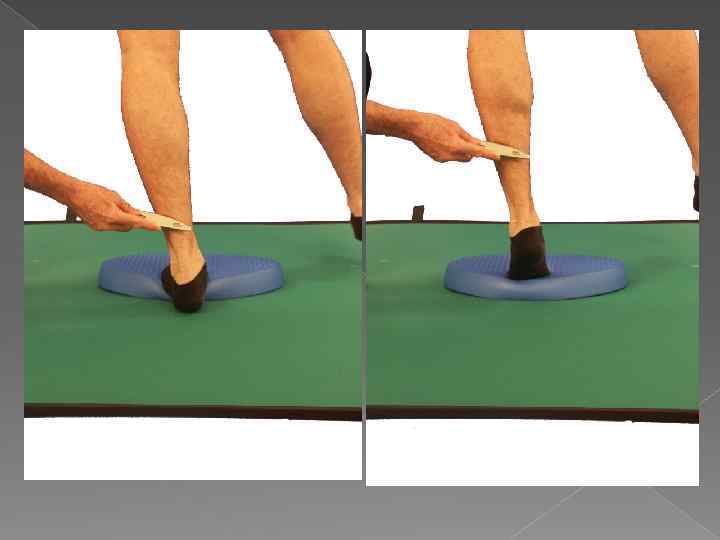
 Ankle Propiroception
Ankle Propiroception
 ANTERIOR SHIN SPLINTS
ANTERIOR SHIN SPLINTS
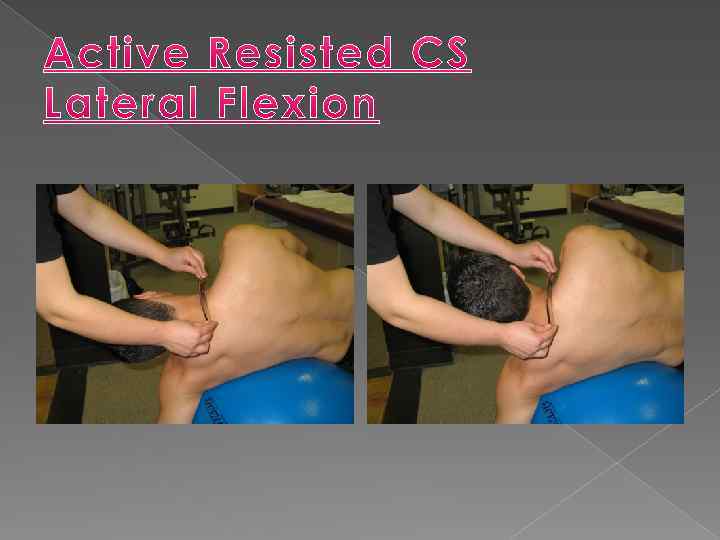
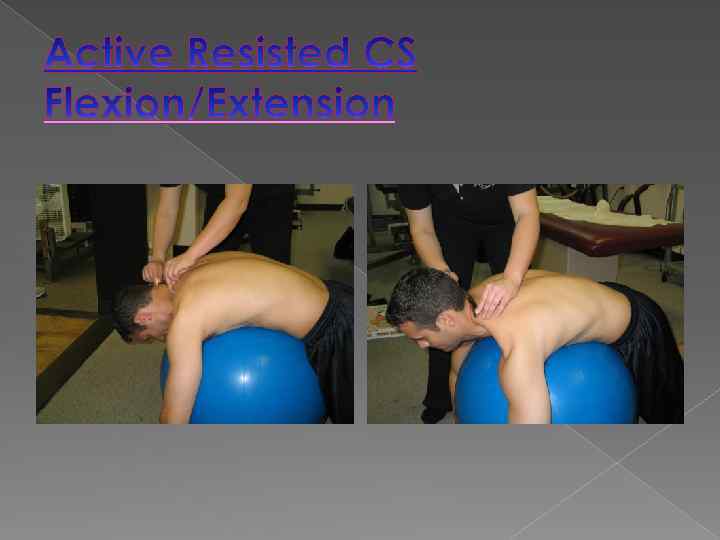
 Cervical Spine Demonstration
Cervical Spine Demonstration
 Cervical Flexion/Extension GT
Cervical Flexion/Extension GT
 Active Resisted CS with Rotation
Active Resisted CS with Rotation
 Active Resisted Upper Trap/Levator Scap
Active Resisted Upper Trap/Levator Scap

 CERVICAL SPRAIN/STRAIN Correction Strip
CERVICAL SPRAIN/STRAIN Correction Strip



 Questions and Answers
Questions and Answers

 Every patient is different, and that’s why there is no cook book for care.
Every patient is different, and that’s why there is no cook book for care.
 www. spine-health. com www. thera-bandacademy. com www. grastontechnique. com www. faktr-pm. com http: //www. stretchingusa. com/ http: //www. spidertech. com
www. spine-health. com www. thera-bandacademy. com www. grastontechnique. com www. faktr-pm. com http: //www. stretchingusa. com/ http: //www. spidertech. com
 Thank You Thyde 444@bellsouth. net
Thank You Thyde 444@bellsouth. net