

e75b397a1302cb1615aa7a4adfa457dc.ppt
- Количество слайдов: 37

 Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, forprofit delivery
Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, forprofit delivery
 Health care system Funding Private For-profit Public Not-for-profit Delivery Public For-profit Private Not-for-profit
Health care system Funding Private For-profit Public Not-for-profit Delivery Public For-profit Private Not-for-profit
 Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care is crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, for -profit delivery
Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care is crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, for -profit delivery
") According to OECD Source: OECD Health data, Organization for Economic Co-operation and Development (OECD) 2008
According to OECD Source: OECD Health data, Organization for Economic Co-operation and Development (OECD) 2008
 in 1992 Source: OECD 2004") Total Expenditure on Health (% GDP) in 1992 Source: OECD 2004
Total Expenditure on Health (% GDP) in 1992 Source: OECD 2004
 in 2005 Source: OECD 2008") Total Expenditure on Health (% GDP) in 2005 Source: OECD 2008
Total Expenditure on Health (% GDP) in 2005 Source: OECD 2008
 Isn’t health care eating up provincial budgets? • 1980 – health care 30% of Ontario budget • 2004 – health care 45% of Ontario budget • but public health care expenditure as % of GDP down, not up?
Isn’t health care eating up provincial budgets? • 1980 – health care 30% of Ontario budget • 2004 – health care 45% of Ontario budget • but public health care expenditure as % of GDP down, not up?
 What are we spending less on? • education – universities from 0. 5% GDP to < 0. 18% • employment insurance – 80% eligible to 40% in Ontario • social support • urban infrastructure • subsidized housing
What are we spending less on? • education – universities from 0. 5% GDP to < 0. 18% • employment insurance – 80% eligible to 40% in Ontario • social support • urban infrastructure • subsidized housing
 Ensuring sustainability • wait time initiatives • centralization of lists • integration of care – specialized surgical facilities • interprofessional Care • right provider, right place, right time • chronic disease management • self-care pathways • home care and community-based care • electronic Health Record • duplication minimization • safety and quality
Ensuring sustainability • wait time initiatives • centralization of lists • integration of care – specialized surgical facilities • interprofessional Care • right provider, right place, right time • chronic disease management • self-care pathways • home care and community-based care • electronic Health Record • duplication minimization • safety and quality
 Examples of Success • Hamilton – 70% decrease in referrals to psychiatrists • Alberta • reduced wait times for hip and knee replacements from 19 months to 11 weeks • Sault Ste. Marie – 50% reduction in readmissions of heart failure patients • Nova Scotia South Shore • no ventilator associated pneumonias in 14 months
Examples of Success • Hamilton – 70% decrease in referrals to psychiatrists • Alberta • reduced wait times for hip and knee replacements from 19 months to 11 weeks • Sault Ste. Marie – 50% reduction in readmissions of heart failure patients • Nova Scotia South Shore • no ventilator associated pneumonias in 14 months
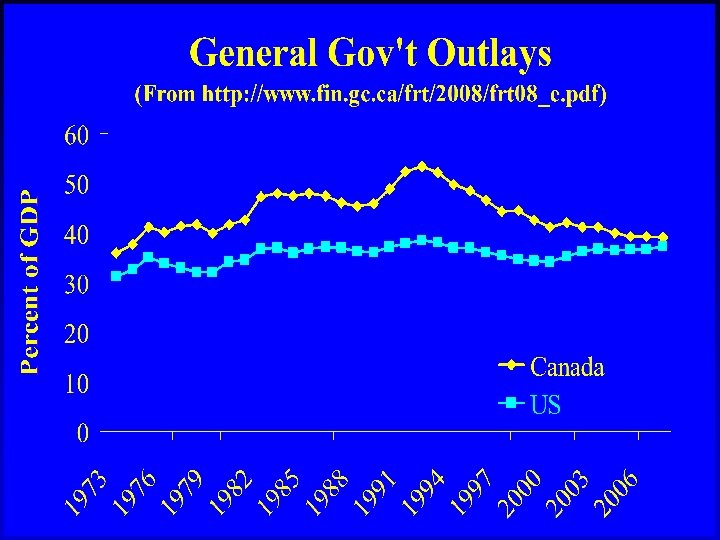
 Is high quality universal health care for all sustainable? • health care as % of GDP – total stable over last 15 years - public even less - Canada 2 nd 15 years ago, now middle of pack - tax cuts, not health spending, has compromised other social spending - innovation can further increase efficiency - Romanow: Health care as sustainable as we choose it to be
Is high quality universal health care for all sustainable? • health care as % of GDP – total stable over last 15 years - public even less - Canada 2 nd 15 years ago, now middle of pack - tax cuts, not health spending, has compromised other social spending - innovation can further increase efficiency - Romanow: Health care as sustainable as we choose it to be
 Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care is crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, for -profit delivery
Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care is crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, for -profit delivery
 Logic and logical problems • more money from private funding – more resources, wait times shorter • physician and nursing shortage – private funding won’t train more – publicly funded facilities lose best trained • privately funded care can only exist if waiting lists for publicly funded care • affluent support for publicly funded care dependent on participation
Logic and logical problems • more money from private funding – more resources, wait times shorter • physician and nursing shortage – private funding won’t train more – publicly funded facilities lose best trained • privately funded care can only exist if waiting lists for publicly funded care • affluent support for publicly funded care dependent on participation
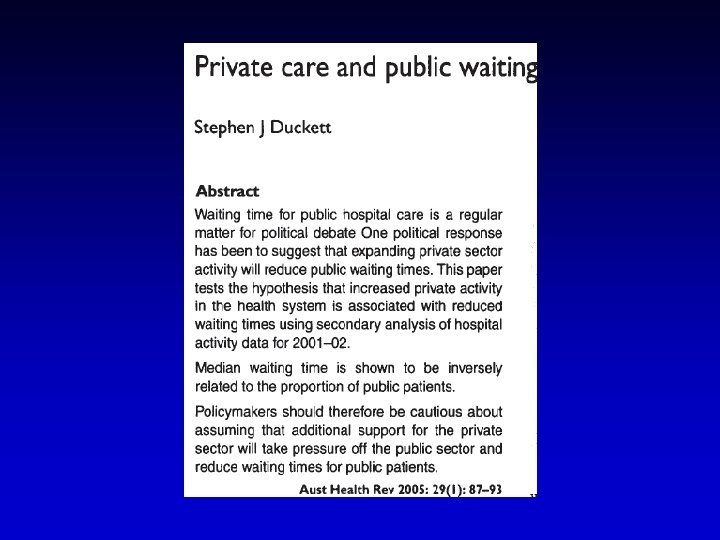
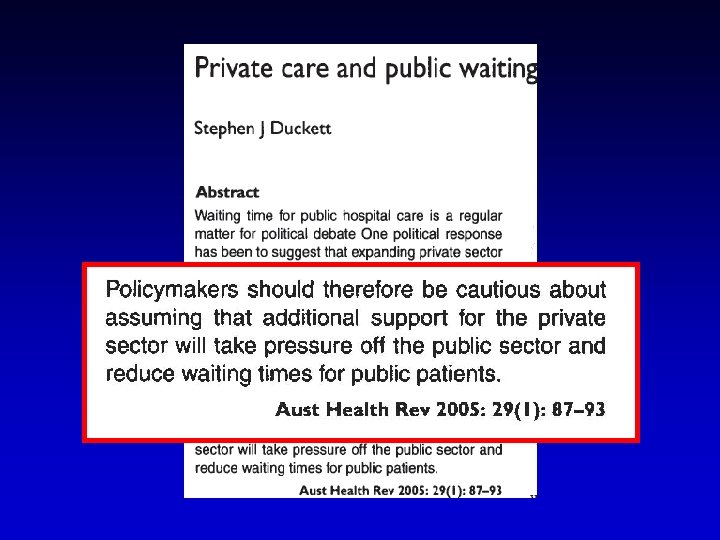
. Australian Health Review 29. 87.") Access More private care More public care Duckett. (2005). Australian Health Review 29. 87.
Access More private care More public care Duckett. (2005). Australian Health Review 29. 87.
 Hurley et. al
Hurley et. al
 Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care is crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, for -profit delivery
Myths and demystification • Canadian health care spending is out of control – universal health care is unsustainable – health care is crowding out other public spending • parallel privately funded care can shorten waiting lists • the private sector always does it better – efficiency gains with private funding, for -profit delivery
 Private Funding is Inefficient Total expenditure on health as a % of GDP 18 16 14 12 10 United States 8 Canada 6 4 2 0 1965 1970 OECD Health Data (2007) 1975 1980 1985 1990 1995 2000 2005
Private Funding is Inefficient Total expenditure on health as a % of GDP 18 16 14 12 10 United States 8 Canada 6 4 2 0 1965 1970 OECD Health Data (2007) 1975 1980 1985 1990 1995 2000 2005
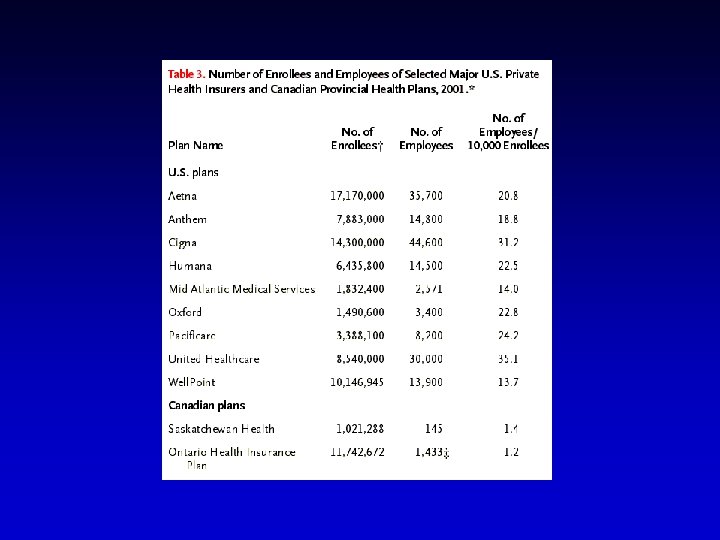
 Administration as % of Total HC Exp 35% 30% 25% 20% 15% 10% 5% 0% US CAN S Woolhandler Int J H Serv 2004; 34: 65 -78.
Administration as % of Total HC Exp 35% 30% 25% 20% 15% 10% 5% 0% US CAN S Woolhandler Int J H Serv 2004; 34: 65 -78.
 Administrative cost difference • developing insurance packages • selling insurance • evaluating applications • documenting use of services – hospital and physician offices • assessing claims • executive salaries • profits
Administrative cost difference • developing insurance packages • selling insurance • evaluating applications • documenting use of services – hospital and physician offices • assessing claims • executive salaries • profits
 Cost Control • public pay – physician services slight decrease • 15. 4% 1991 to 13. 4% – hospital marked decrease • 45% (1976) to 28% • pharmaceutical increase – 9% (1984) to 17. 4%
Cost Control • public pay – physician services slight decrease • 15. 4% 1991 to 13. 4% – hospital marked decrease • 45% (1976) to 28% • pharmaceutical increase – 9% (1984) to 17. 4%
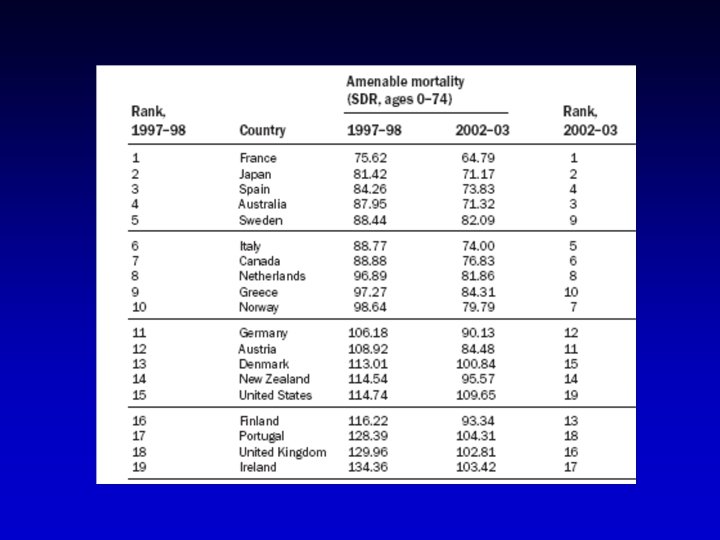
 Analysis of deaths considered “amenable to health care” in those under 75 years of age in 19 industrialized countries
Analysis of deaths considered “amenable to health care” in those under 75 years of age in 19 industrialized countries
 Systematic review health outcomes in Canada and US, 2007, Open Medicine. • 17 leading US/Canadian researchers • comprehensive search yielded 38 studies • compared outcomes of conditions with identical diagnosis • cancer, cardiovascular disease, renal dialysis, cataracts. . . • 14 studies showed better outcomes in Canada • 5/10 with broad populations, statistical adjustment • 5 studies favoured the U. S. • 2/10 high quality • 19 studies had equivalent or mixed results • 3/10 high quality
Systematic review health outcomes in Canada and US, 2007, Open Medicine. • 17 leading US/Canadian researchers • comprehensive search yielded 38 studies • compared outcomes of conditions with identical diagnosis • cancer, cardiovascular disease, renal dialysis, cataracts. . . • 14 studies showed better outcomes in Canada • 5/10 with broad populations, statistical adjustment • 5 studies favoured the U. S. • 2/10 high quality • 19 studies had equivalent or mixed results • 3/10 high quality
 Summary • single public pay more efficient – administrative efficiencies – effective cost control • single public payer cost-efficient – equal or better outcomes than much more efficient U. S. system
Summary • single public pay more efficient – administrative efficiencies – effective cost control • single public payer cost-efficient – equal or better outcomes than much more efficient U. S. system
 Health care system Funding Private For-profit Public Not-for-profit Delivery Public For-profit Private Not-for-profit
Health care system Funding Private For-profit Public Not-for-profit Delivery Public For-profit Private Not-for-profit
 Debate • advocates of investor owned private for-profit health care delivery argue – for-profit providers deliver care more efficiently • advocates of not-for-profit health care delivery fear – for-profit facilities compromise care to maintain investors returns
Debate • advocates of investor owned private for-profit health care delivery argue – for-profit providers deliver care more efficiently • advocates of not-for-profit health care delivery fear – for-profit facilities compromise care to maintain investors returns
 For-profit or not-for-profit? • for-profit initiatives – Ontario: home care, MRI/CT, P 3 hospitals – other provinces, surgical clinics • systematic reviews – investor-owned for-profit vs nfp • hospital death rates • dialysis death rates • hospital charges to payers
For-profit or not-for-profit? • for-profit initiatives – Ontario: home care, MRI/CT, P 3 hospitals – other provinces, surgical clinics • systematic reviews – investor-owned for-profit vs nfp • hospital death rates • dialysis death rates • hospital charges to payers
 Systematic review and meta-analysis • systematic review – focused question – explicit eligibility criteria – comprehensive search – assessment of validity of primary studies – eligibility and quality assessments are reproducible • meta-analysis combines the results of several studies
Systematic review and meta-analysis • systematic review – focused question – explicit eligibility criteria – comprehensive search – assessment of validity of primary studies – eligibility and quality assessments are reproducible • meta-analysis combines the results of several studies
 Screening process • 8665 unique citations • teams of 2 individuals – independently screened the titles and abstracts • 805 full text publications – identified for full review
Screening process • 8665 unique citations • teams of 2 individuals – independently screened the titles and abstracts • 805 full text publications – identified for full review
 • teams") Assessment of study eligibility • masked results (i. e. blacked them out) • teams of two individuals – independently evaluated each masked article to determine eligibility • disagreements resolved by consensus • agreement was excellent (Kappa 0. 83)
Assessment of study eligibility • masked results (i. e. blacked them out) • teams of two individuals – independently evaluated each masked article to determine eligibility • disagreements resolved by consensus • agreement was excellent (Kappa 0. 83)
 Results • all studies – comprehensive search, top quality studies – published in top peer-reviewjournals • hospital mortality – – – 38 million patients between 1982 -1995 2% more deaths in for-profit 2, 000 deaths in Canada (MVA, cancer, suicide) • dialysis mortality – 500, 000 patient years 1973 to 1997 – 8% more deaths in for-profit • charges 19 greater in for-profit
Results • all studies – comprehensive search, top quality studies – published in top peer-reviewjournals • hospital mortality – – – 38 million patients between 1982 -1995 2% more deaths in for-profit 2, 000 deaths in Canada (MVA, cancer, suicide) • dialysis mortality – 500, 000 patient years 1973 to 1997 – 8% more deaths in for-profit • charges 19 greater in for-profit
 Summary: overall • pressures on health spending but: – Canada better than most other countries – problem is tax cuts, not health spending • private pay won’t shorten waiting lists – will just make ability to pay, rather than need, the criterion to get to the front • single payer maximizes efficiency – not-for-profit more efficent than forprofit
Summary: overall • pressures on health spending but: – Canada better than most other countries – problem is tax cuts, not health spending • private pay won’t shorten waiting lists – will just make ability to pay, rather than need, the criterion to get to the front • single payer maximizes efficiency – not-for-profit more efficent than forprofit