Myocardial infarctions.ppt
- Количество слайдов: 70
 Myocardial infarctions
Myocardial infarctions
 T wave • ST segment –") Initial period • High-amplitude positive tall peaked (hyperacute) T wave • ST segment – elevated (3 -4 up to 10 -15 mm elevation). • Elevated ST segment with peaked T-wave form typical monophase curve (“cat’s back”) • Reciprocal changes - ST depression in leads, opposite the infarction zone • Transient sign: inraventricular block: increase of QRS duration to 0. 12; slow R increase; QRS voltage rise, increase of VAT to 0. 045 sec in leads, directed towards infarction zone. Disappear with Q appearance and T invertion.
Initial period • High-amplitude positive tall peaked (hyperacute) T wave • ST segment – elevated (3 -4 up to 10 -15 mm elevation). • Elevated ST segment with peaked T-wave form typical monophase curve (“cat’s back”) • Reciprocal changes - ST depression in leads, opposite the infarction zone • Transient sign: inraventricular block: increase of QRS duration to 0. 12; slow R increase; QRS voltage rise, increase of VAT to 0. 045 sec in leads, directed towards infarction zone. Disappear with Q appearance and T invertion.
 Acute period • Inverted symmetric T wave • ST segment – arch-formed elevation; decrease of the elevation to the middle of the 1 st week, small ST rise may persist during the whole phase • Pathologic Q (duration 0. 04 sec and more; height ¼ R and more): QR; Qr, QS • Three-phase curve: elevation of ST with inverted T complexes • Reciprocal changes (in leads, opposite the infarction zone) reveal: ST depression and upright or isoelecric T
Acute period • Inverted symmetric T wave • ST segment – arch-formed elevation; decrease of the elevation to the middle of the 1 st week, small ST rise may persist during the whole phase • Pathologic Q (duration 0. 04 sec and more; height ¼ R and more): QR; Qr, QS • Three-phase curve: elevation of ST with inverted T complexes • Reciprocal changes (in leads, opposite the infarction zone) reveal: ST depression and upright or isoelecric T
 Subacute • QR, Qr, QS complexes • Isoelectric ST (horizontal or a little bit convex) • Inversed symmetrical T, wide, deep (maximal depth – end of the 4 rth week) • Prolonged QT (prolonged electric systole) • Later – gradual decrease of T depth, beginning from the peripheric sites of the infarction zone
Subacute • QR, Qr, QS complexes • Isoelectric ST (horizontal or a little bit convex) • Inversed symmetrical T, wide, deep (maximal depth – end of the 4 rth week) • Prolonged QT (prolonged electric systole) • Later – gradual decrease of T depth, beginning from the peripheric sites of the infarction zone
 Post-infarction period • scar changes in one or more leads (QR, QS, low-amplitude flattered r, negative but not deep T) • Possible signs of chronic coronary insufficience • Chronic LV aneurism – convex or elevated ST
Post-infarction period • scar changes in one or more leads (QR, QS, low-amplitude flattered r, negative but not deep T) • Possible signs of chronic coronary insufficience • Chronic LV aneurism – convex or elevated ST
 Localization ECG leads artery affected Anteriorseptal V 1 -V 2 Left descendent branch (septal branches) Anteriorseptal V 2 -V 4 Left descendent or its branches Anteriorlateral V 4 -V 6, I, a. VL Left descendent or circumflex Wide-spread anterior V 1 -V 6, I, a. VL Left descendent Inferior II, III, a. VF Right, more rare left circumflex Dorsal V 1 and V 2 reciprocal changes Circumflex or right coronary Right ventricle V 1 and r. V 3 -r. V 4 (right leads, respecting V 3 -V 4) Right coronary
Localization ECG leads artery affected Anteriorseptal V 1 -V 2 Left descendent branch (septal branches) Anteriorseptal V 2 -V 4 Left descendent or its branches Anteriorlateral V 4 -V 6, I, a. VL Left descendent or circumflex Wide-spread anterior V 1 -V 6, I, a. VL Left descendent Inferior II, III, a. VF Right, more rare left circumflex Dorsal V 1 and V 2 reciprocal changes Circumflex or right coronary Right ventricle V 1 and r. V 3 -r. V 4 (right leads, respecting V 3 -V 4) Right coronary
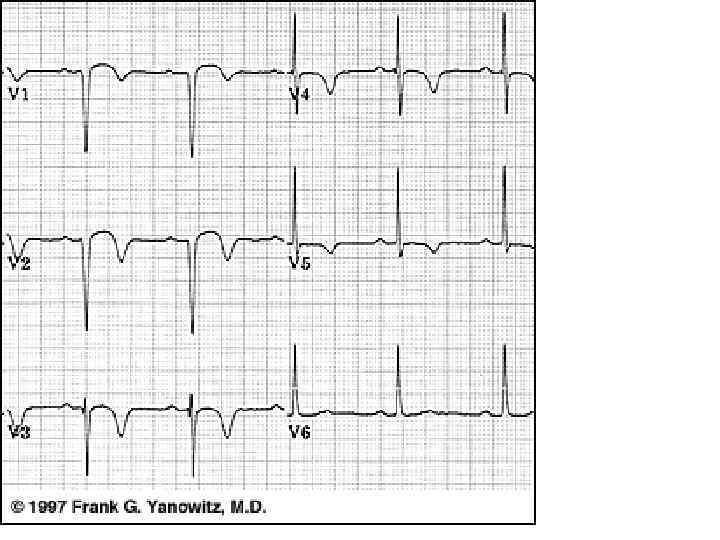
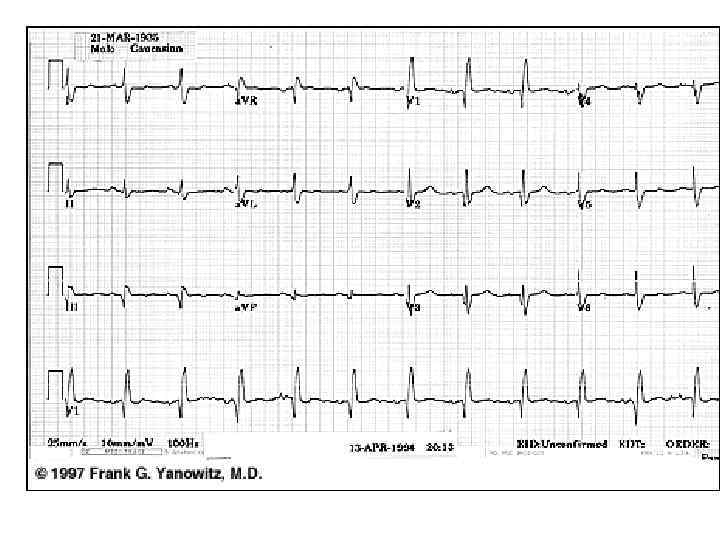
 Anteroseptal MI with spreading to lateral wall
Anteroseptal MI with spreading to lateral wall
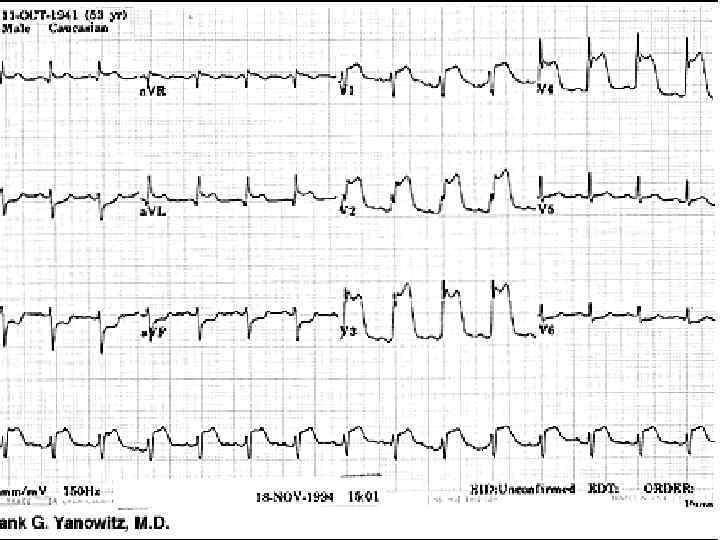
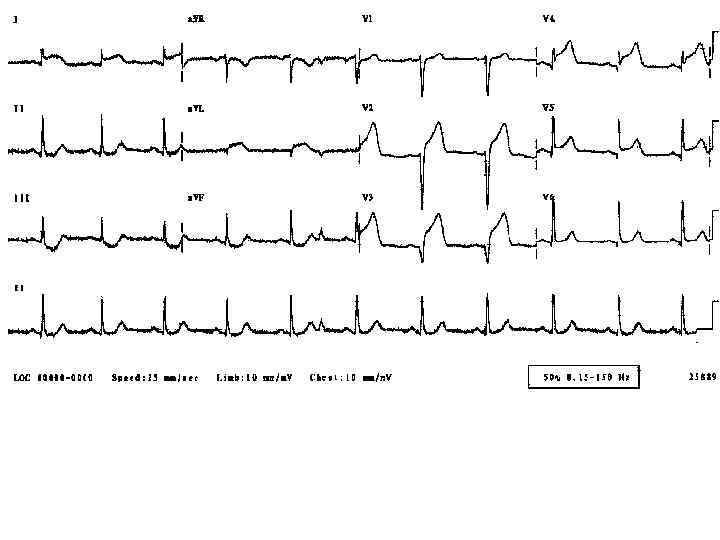
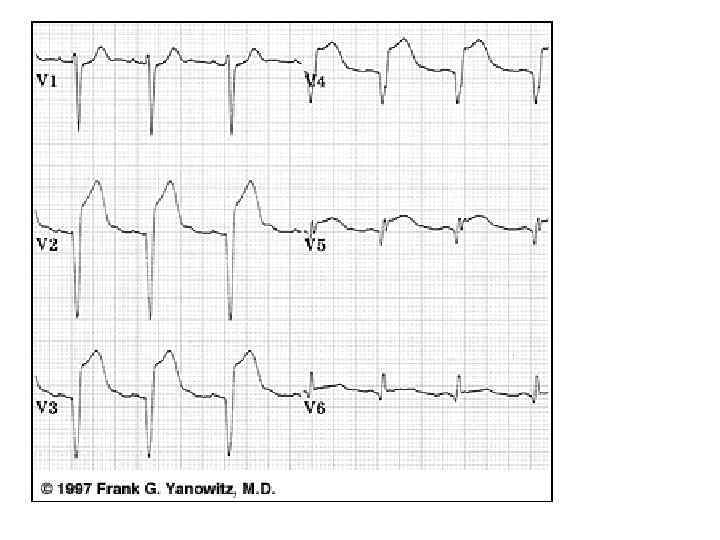
 Extensive Anterior/Anterolateral MI
Extensive Anterior/Anterolateral MI
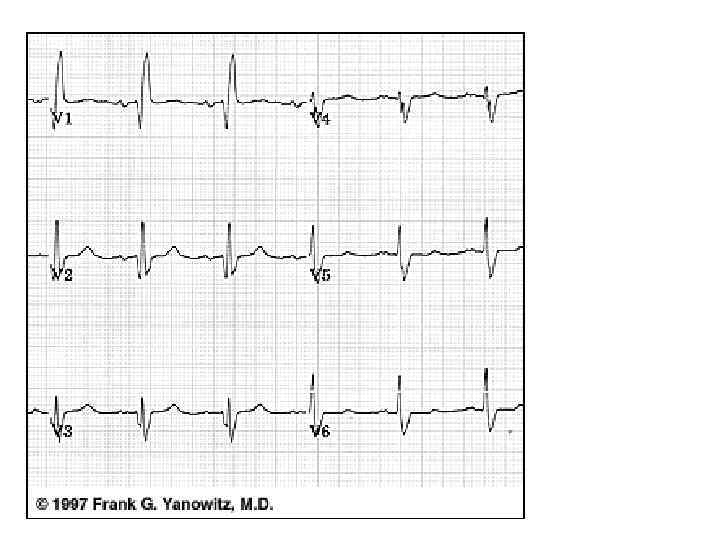
 Anteroseptal/lateral
Anteroseptal/lateral
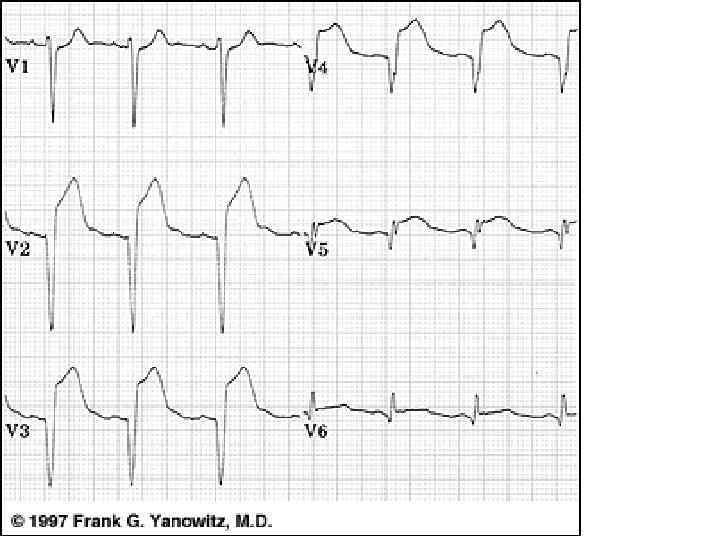
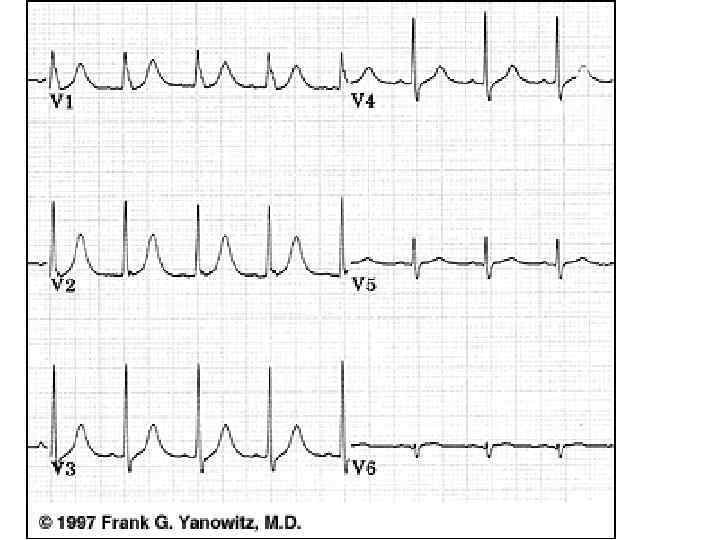
 Anterolateral
Anterolateral
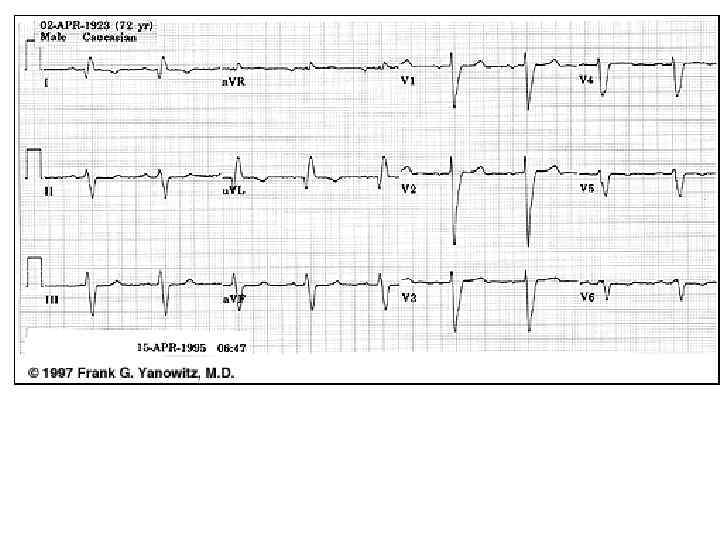
") Anterolateral (without Q)
Anterolateral (without Q)
") High Lateral Wall MI (seen in a. VL)
High Lateral Wall MI (seen in a. VL)
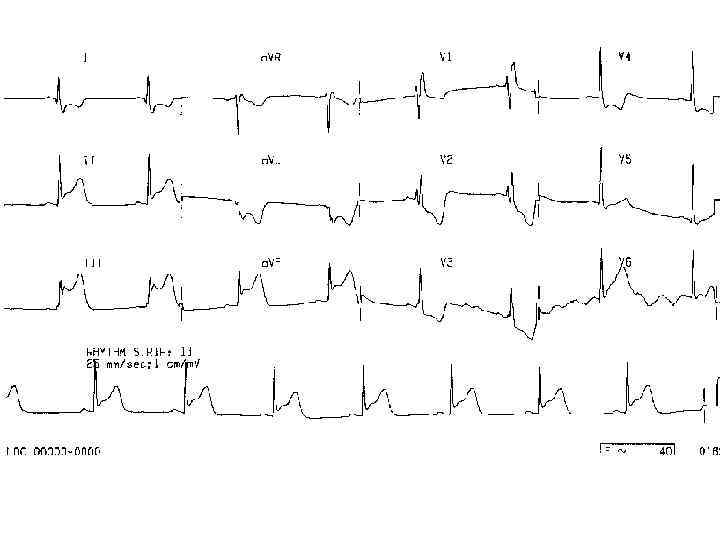
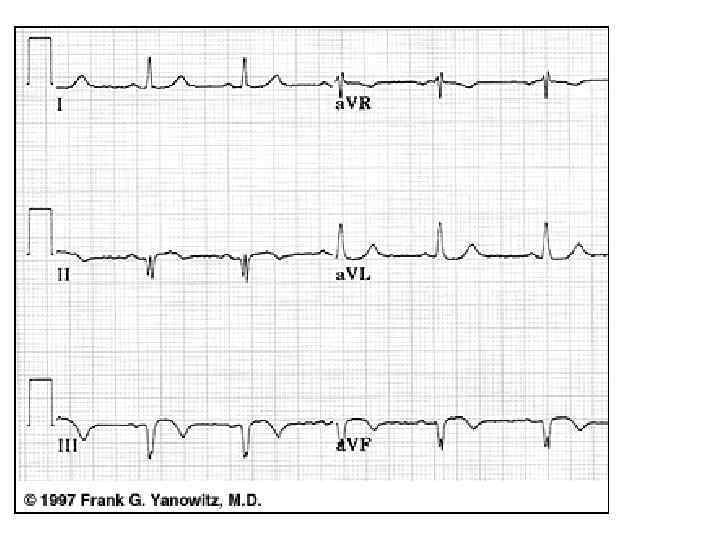
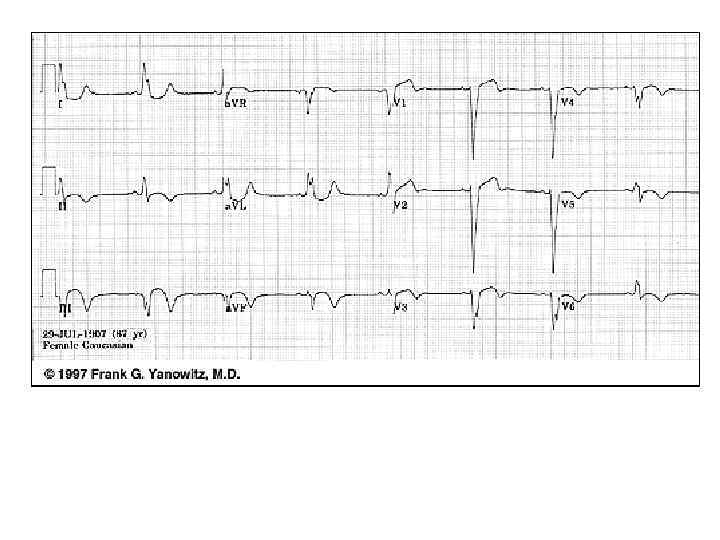
 Inferior
Inferior
 Infero-posterior MI
Infero-posterior MI
 Inferior
Inferior
 Old inferior
Old inferior
 Acute Inferoposterior MI
Acute Inferoposterior MI
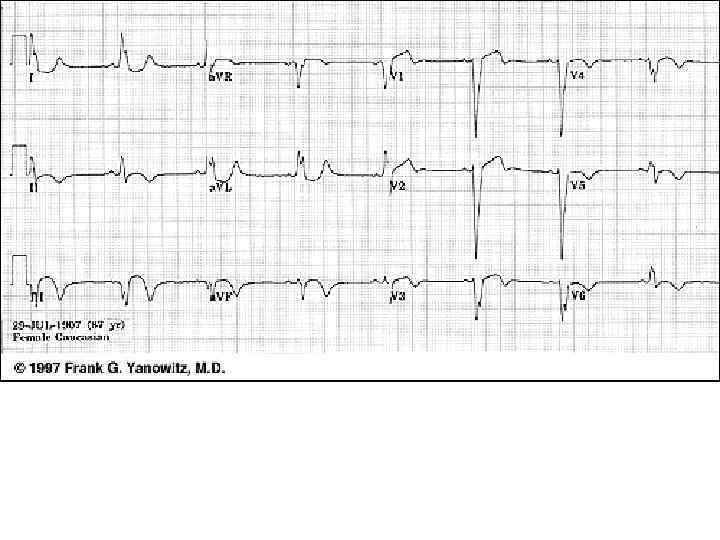
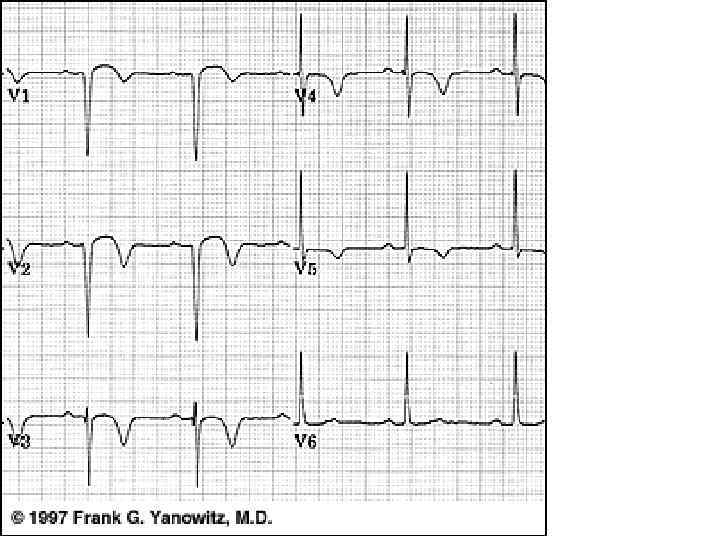
 Posterior • pathologic R waves in leads V 1 -2 (equivalent of pathologic Q waves seen from the perspective of the anterior leads) • Tall T waves in V 1 -V 2 - posterior equivalent of inverted T waves
Posterior • pathologic R waves in leads V 1 -2 (equivalent of pathologic Q waves seen from the perspective of the anterior leads) • Tall T waves in V 1 -V 2 - posterior equivalent of inverted T waves
 Postero-lateral MI
Postero-lateral MI
 Posterior-lateral
Posterior-lateral
 Inferoposterior MI
Inferoposterior MI
 Old Infero-posterior MI
Old Infero-posterior MI
 Old Inferior MI
Old Inferior MI
 Old Inferior MI, PVCs, and Atrial Fibrillation
Old Inferior MI, PVCs, and Atrial Fibrillation
 Old Inferior MI
Old Inferior MI
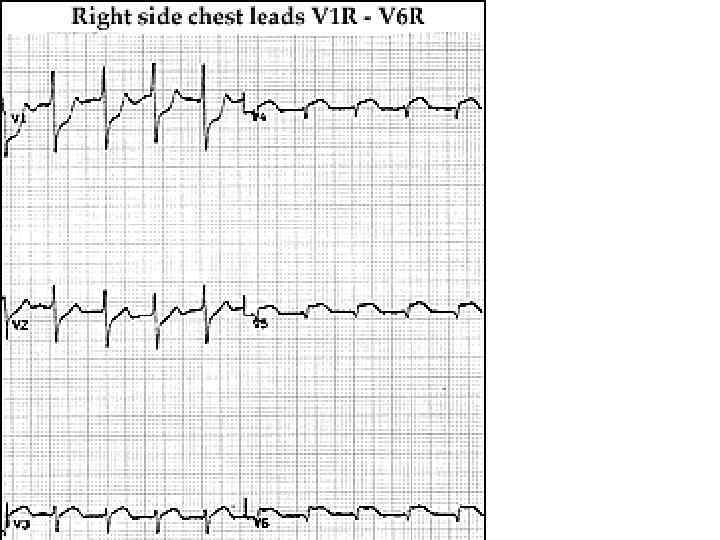
 Right ventricle MI • Right precordial leads V 1 R - V 6 R • Reciprocal ST segment depression in leads I and a. VL. Sometimes posterior wall changes may be • Hyperacute ST segment elevation in leads II, III, a. VF (inferior location) • ST depression is seen in leads V 1 -2 (an expression of posterior wall injury).
Right ventricle MI • Right precordial leads V 1 R - V 6 R • Reciprocal ST segment depression in leads I and a. VL. Sometimes posterior wall changes may be • Hyperacute ST segment elevation in leads II, III, a. VF (inferior location) • ST depression is seen in leads V 1 -2 (an expression of posterior wall injury).
 Inferoposterior with Right Ventricular MI
Inferoposterior with Right Ventricular MI
 True Posterior MI and Right Ventricular MI • V 1 R - V 6 R • True posterior MI: marked ST segment elevation in V 1 R (actual V 2) and V 2 R (actual V 1). • The RV MI: ST elevation in V 3 R to V 6 R.
True Posterior MI and Right Ventricular MI • V 1 R - V 6 R • True posterior MI: marked ST segment elevation in V 1 R (actual V 2) and V 2 R (actual V 1). • The RV MI: ST elevation in V 3 R to V 6 R.
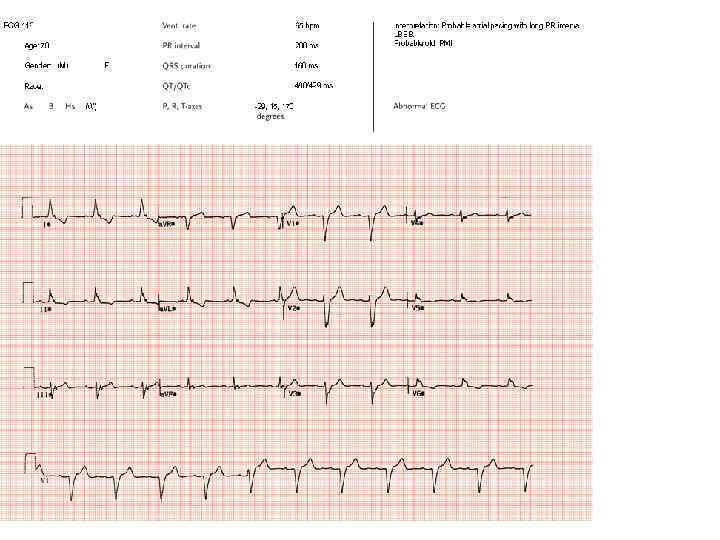
 Infero-posterior MI & RBBB • • - MI: Deep Q waves in II, III, a. VF tall R waves in V 1 -2 Q in V 5 -6 - apical lateral wall extension RBB wide QRS (>0. 12 s) Rs. R in V 1 RBBB with initial R in V 1 equal or greater than the R', true posterior MI must be considered.
Infero-posterior MI & RBBB • • - MI: Deep Q waves in II, III, a. VF tall R waves in V 1 -2 Q in V 5 -6 - apical lateral wall extension RBB wide QRS (>0. 12 s) Rs. R in V 1 RBBB with initial R in V 1 equal or greater than the R', true posterior MI must be considered.
 Infero-posterior MI with RBBB • initial R is taller than R' in V 1. - true posterior MI. • tall initial R wave in V 1 is a "pathologic R" wave analagous to the "pathologic Q" wave of an anterior MI.
Infero-posterior MI with RBBB • initial R is taller than R' in V 1. - true posterior MI. • tall initial R wave in V 1 is a "pathologic R" wave analagous to the "pathologic Q" wave of an anterior MI.
 Inferior MI and RBBB
Inferior MI and RBBB
 Inferior & Anteroseptal MI + RBBB • Pathologic Q waves in II, III, a. VF (inferior MI) and in leads V 1 -3 (anteroseptal MI) • RBBB - wide QRS (>0. 12 s) + anterior/rightwards orientation of terminal QRS forces. • When anteroseptal MI complicates RBBB (or visa versa) r. SR' complex in V 1 (typical of RBBB) becomes q. R
Inferior & Anteroseptal MI + RBBB • Pathologic Q waves in II, III, a. VF (inferior MI) and in leads V 1 -3 (anteroseptal MI) • RBBB - wide QRS (>0. 12 s) + anterior/rightwards orientation of terminal QRS forces. • When anteroseptal MI complicates RBBB (or visa versa) r. SR' complex in V 1 (typical of RBBB) becomes q. R
 Atypical LBBB with Q Waves in Leads I and a. VL • In typical LBBB, there are no initial Q waves in leads I, a. VL, and V 6. If Q waves are present in 2 or more of these leads, myocardial infarction is present.
Atypical LBBB with Q Waves in Leads I and a. VL • In typical LBBB, there are no initial Q waves in leads I, a. VL, and V 6. If Q waves are present in 2 or more of these leads, myocardial infarction is present.
 Atypical LBBB with Primary T Wave Abnormalities • T waves in the same direction as the major deflection of the QRS • seen in leads I, III, a. VL, V 2 -4. • Most likely - myocardial infarction.
Atypical LBBB with Primary T Wave Abnormalities • T waves in the same direction as the major deflection of the QRS • seen in leads I, III, a. VL, V 2 -4. • Most likely - myocardial infarction.
 MI +LBBB
MI +LBBB
 MI +LBBB
MI +LBBB
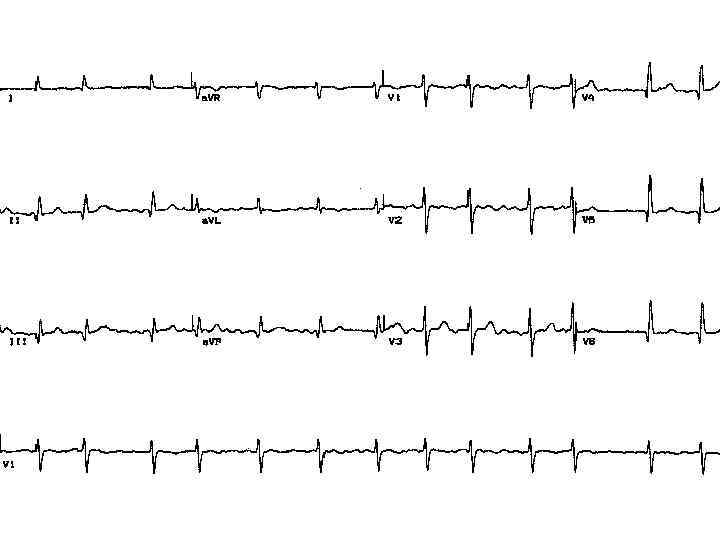
 Accelerated Junctional Rhythm and Inferior MI
Accelerated Junctional Rhythm and Inferior MI
 Old inferior-posterior MI with intraventricular conduction abnormalities
Old inferior-posterior MI with intraventricular conduction abnormalities
 • • PMIs frequently occur without the classical tall, broad R-waves in V 1 and V 2. Often there is a reduction of >50% in the R-wave between leads V 4 and V 6 with S-wave reduction and prominent notching in the anterior chest leads. In addition, the amplitude of the Twaves in the anterior chest leads may be increased and appear atypically symmetrical.
• • PMIs frequently occur without the classical tall, broad R-waves in V 1 and V 2. Often there is a reduction of >50% in the R-wave between leads V 4 and V 6 with S-wave reduction and prominent notching in the anterior chest leads. In addition, the amplitude of the Twaves in the anterior chest leads may be increased and appear atypically symmetrical.
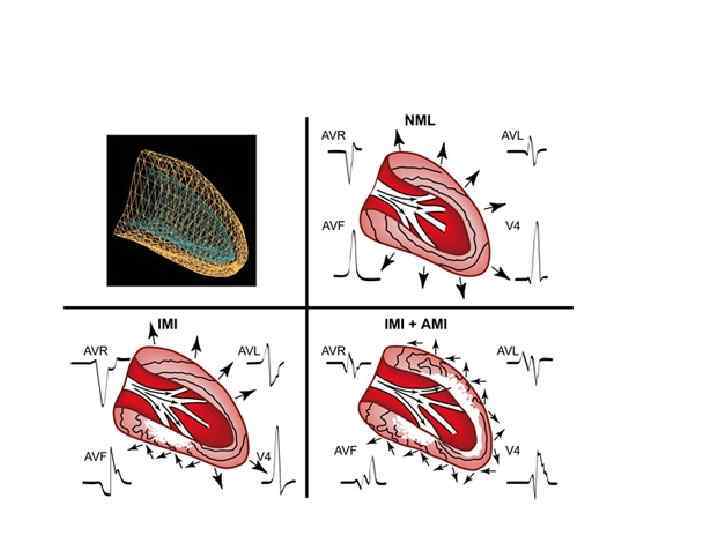
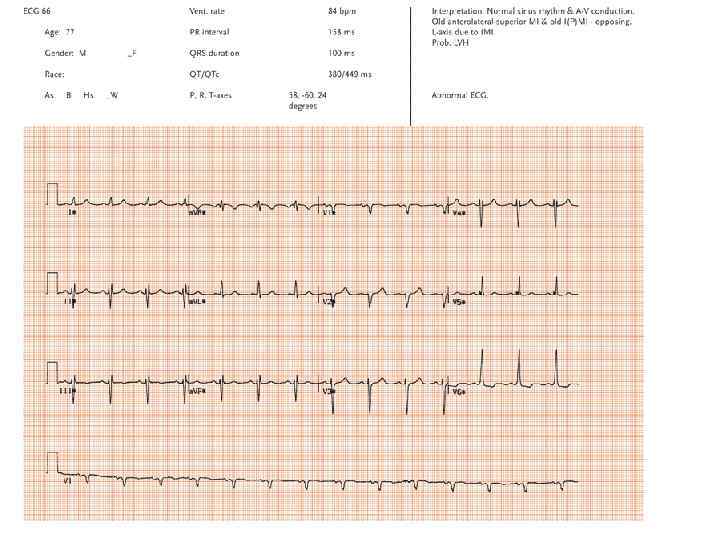
") • . An ECG from a patient with opposing inferior and anterolateral (superior) MIs. Note that although no Q-waves are present, there are complex QRS waveforms referred to as M and W complexes in both the inferior and anterolateral leads which are diagnostically equivalent to opposing Qwaves.
• . An ECG from a patient with opposing inferior and anterolateral (superior) MIs. Note that although no Q-waves are present, there are complex QRS waveforms referred to as M and W complexes in both the inferior and anterolateral leads which are diagnostically equivalent to opposing Qwaves.
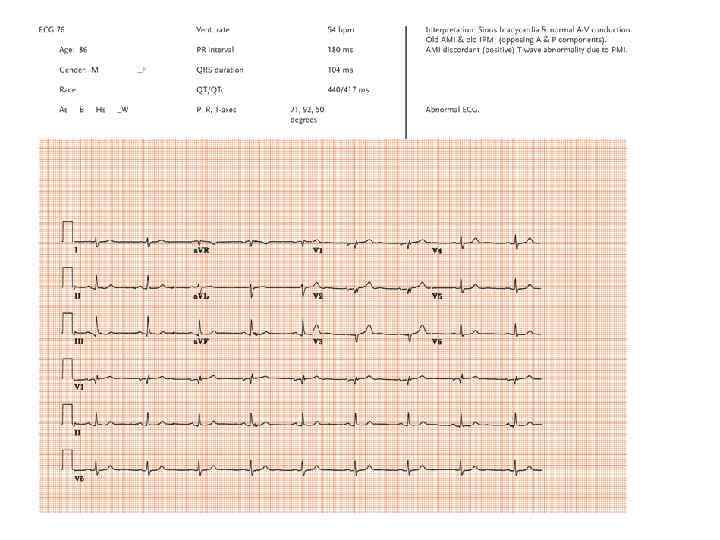
 • This ECG is from a patient with opposing anterior and posterior infarcts. Note the absence of initial r-waves V 1 -V 3 due to the ASMI. The PMI results in the reduced amplitude with prominent notchings of Swave in V 2 and the reduced S-wave and small terminal r-wave in V 1.
• This ECG is from a patient with opposing anterior and posterior infarcts. Note the absence of initial r-waves V 1 -V 3 due to the ASMI. The PMI results in the reduced amplitude with prominent notchings of Swave in V 2 and the reduced S-wave and small terminal r-wave in V 1.
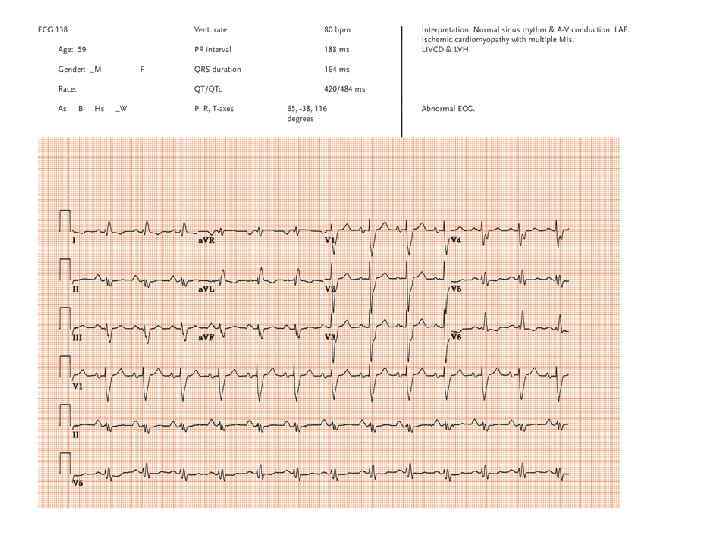
 • ECGs in patients with ischemic cardiomyopathy demonstrate an unusual repetition of this complex pattern characterized by prolonged QRS of the LV delay type, increased QRS voltage, tall narrow anterior R-waves, marked QRS notching, slurring and axis shifts.
• ECGs in patients with ischemic cardiomyopathy demonstrate an unusual repetition of this complex pattern characterized by prolonged QRS of the LV delay type, increased QRS voltage, tall narrow anterior R-waves, marked QRS notching, slurring and axis shifts.
 • An ECG from a patient with left bundle branch block and an old IMI. Note the marked notching of the mid-QRS which reflects the time and location of the wavefront as it passes by the irregular border zone in the surviving subepicardium overlying the infarct.
• An ECG from a patient with left bundle branch block and an old IMI. Note the marked notching of the mid-QRS which reflects the time and location of the wavefront as it passes by the irregular border zone in the surviving subepicardium overlying the infarct.