6a24261ae98758e4671c02a459504400.ppt
- Количество слайдов: 92



Modern Advances in Cervical Cancer Screening 高雄長庚紀念醫院 婦產部 婦癌科 助理教授 林浩 醫師
肝 19% 21% 子宮頸(5985人) (4625人)肺 14% 18% 乳房(5065人) (4178人)結腸及直腸")
男女性十大癌症發生分率 年 : 民國 90 (6193人)肝 19% 21% 子宮頸(5985人) (4625人)肺 14% 18% 乳房(5065人) (4178人)結腸及直腸 13% 11% 結腸及直腸(3188人) (3230人)口腔 10% 8% 肝(2391人) (2356人)胃 7% 8% 肺(2156人) (2012人)攝護腺 6% 4% 胃(1176人) (1290人)膀胱 4% 3% 甲狀腺(956人) (1151人)食道 3% 3% 皮膚(929人) (1039人)皮膚 3% 3% 卵巢(741人) (1004人)鼻咽 3% 2% 子宮體(671人) (6079人)其他癌症 18% 男性共 33, 157人 備註 : 子宮頸癌含原位癌 , 口腔癌含下咽及口咽 18% 其他癌症(5192人) 女性共 28, 450人
 順位 1 報告數 人(%) 原發部位 粗發生率 (每十萬 年齡標準化 發生率 子宮頸 5,")
民國九十年女性十大癌症發生率 人口 ) 順位 1 報告數 人(%) 原發部位 粗發生率 (每十萬 年齡標準化 發生率 子宮頸 5, 985 ( 21. 0) 54. 59 49. 51 子宮頸原位癌 3, 554 ( 12. 5) 32. 42 29. 18 子宮頸侵襲癌 2, 431 ( 8. 5) 22. 17 20. 33 2 女性乳房 5, 065 ( 17. 8) 46. 20 41. 70 3 結腸及直腸 3, 188 ( 11. 2) 29. 08 26. 85 4 肝及肝內膽管 2, 391 ( 8. 4) 21. 81 20. 80 5 肺、支氣管及氣管 2, 156 ( 7. 6) 19. 66 18. 22 6 胃 1, 176 ( 4. 1) 10. 73 9. 71 7 皮膚 929 ( 3. 3) 8. 47 8. 09 8 甲狀腺 956 ( 3. 4) 8. 72 7. 98 9 卵巢、輸卵管及寬韌帶 741 ( 2. 6) 6. 76 6. 28 10 子宮體 671 ( 2. 4) 6. 12 5. 81 259. 49 243. 41 註:年齡標準化發生率係使用 全癌症 2000年世界標準人口為標準人口。 28, 450 (100. 0)

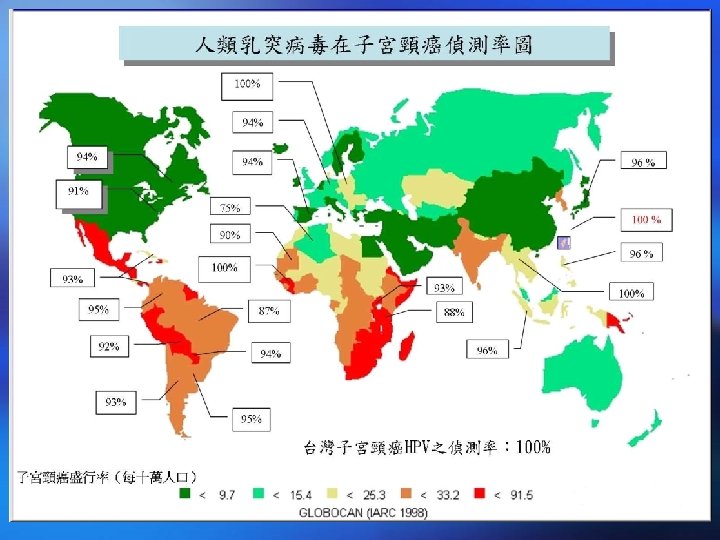
Cervical Cancer: Worldwide

26. 86 23. 97 22. 96 21. 19 16. 91 13. 42 12. 34 8. 65 13. 62 21. 30 11. 75 女性十大癌症年齡標準化發生率之五年變化率 , 民國 86 -90年
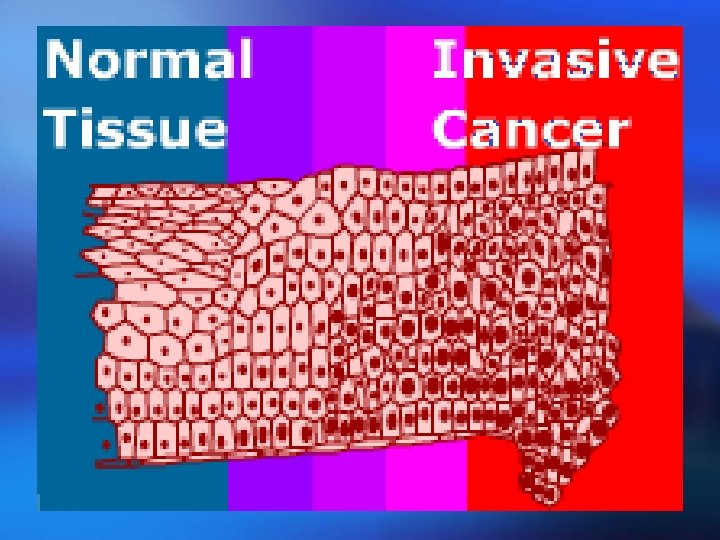
 ¡ Mechanism: Not completely")
Introduction ¡ Normal CIN Invasive cx ca. (Cervical Intraepithelial Neoplasia) ¡ Mechanism: Not completely understood. May be due to infection of sexually transmitted agent such as HPV.
")
Cervical Intraepithelial Neoplasia (CIN)
 Infected both to human &")
Classification & Types of HPV ¡ Human papillomavirus (HPV) Infected both to human & animals. Highly species specific, do not cross infect other species. Over 100 different types of HPV (based on DNA contents). Epitheliotrophic, produce focal epithelial proliferation.

Classification & Types of HPV ¡ Approximately 30 infect the ano- genital region. ¡ Of which 13 are considered 'high risk' as they have the potential to cause high-grade abnormalities of the cervix. ¡ The 13 'high risk' types of HPV (16, 18, 31, 33, 35, 39, 45, 51, 56, 58, 59, 68).

Natural History of HPV Infection 正常子宮頸 約 60% 在 2 -3 年恢復 正常 HPV感染有關之變化 CIN 1 15%在 3 -4年進展 CIN 2, CIN 3 30 -70%在 10年進展 子宮頸侵犯性癌 持續感染 促進因子

History of Cervical Cancer Screening

Screening for Cervical Cancer Effect Skill Cost 2003 HPV testing + Pap smear 1998 Pap. Sure test 1998 automated Pap smear 1996 Thin layer Pap test 1943 Papanicolaou smear 1920 Colposcope

The Colposcope: History ¡ Originally developed by Hans Hinselmann ¡ ¡ in the 1920 s. Pap smear: 1943, as the 1 st line modality for cancer screening. 1960: the colposcope was rediscovered as a complementary test for women with abnormal cytologic findings. Allows the cervix to be viewed at 6~40 fold magnification. Focal length: 200~300 mm.

1920 Colposcope

1920 Colposcope 塗冰醋酸前 塗冰醋酸 30秒後 醋酸白為不正常

Tissue Basis for Colposcopy Normal Squamous Epithelium

Tissue Basis for Colposcopy Atypical Squamous Epithelium

Tissue Basis for Colposcopy Atypical Vessels

Disadvantages of Colposcopy as a Screening Tool for Cervical Cancer 1. Expensive equipment. 2. Technically required. 3. Time consuming. 4. Available only in medical center.

Current Goals of Colposcopy ¡ Indicated for patients with abnormal ¡ ¡ pap smear tests. Diagnostic tool for cervical neoplasia (colposcopic-guided cervical biopsy). Identify occult invasive cancer. Determine degree and extent of abnormality and treat. Follow patients at risk for cervical cancer.

Screening for Cervical Cancer Effect Skill Cost 2003 HPV testing + Pap smear 1998 Pap. Sure test 1998 automated Pap smear 1996 Thin layer Pap test 1943 Papanicolaou smear 1920 Colposcope

1943 Papanicolaou Smear ¡ George Papanicolaou was a Greek physician and anatomist in the United States (1883 - 1962). ¡ Dr. Papanicolaou is the discoverer of "Pap Smear" or "Papanicolaou Smear", a life saving test, saving millions of lives of women around the world by early detecting the cancer of the cervix of uterus and other premalignant conditions of the female genital tract.
")
George Papanicolaou: New Cancer Diagnosis (1928)

Expected Exfoliation of Dysplastic Cells Shedding Dysplastic Cells Adhesion molecules at basement membrane
")
George Papanicolaou: Diagnosis of Uterine Cancer by Vaginal Smear (1943)

1943 Papanicolaou Smear Dr. George Papanicolaou

1943 Papanicolaou Smear

1943 Papanicolaou Smear

1943 Papanicolaou Smear

1943 Papanicolaou Smear Normal HPV Koilocytes LSIL: CIN 1 HSIL: CIN 2 HSIL: CIN 3 Squamous cell carcinoma
 Normal (I) Benign")
RESULTS REPORTED WITH BETHESDA SYSTEM Adequacy Satisfactory Limited Unsatisfactory Descriptive (Class) Normal (I) Benign epithelial cell abnormality Inflammation, atrophic (II) Atypical squamous cells of unknown significance (ASCUS) (III) Low grade squamous intraepithelial lesion (LSIL) (III) High grade squamous intraepithelial lesion (HSIL) (IV) Carcinoma (V)

Screening Results: Management Normal • Conventional cervical cytology smears: Annually • Liquid-based cytology: every 1 -2 years Pap with Hybrid Capture II test: Every 3 years >30 years old ASC-US • Use ASCCP triage guidelines, consider reflex testing LSIL • Colposcopy with directed biopsy HSIL • Colposcopy with directed biopsies Invasive Cancer • Refer to gynecologic oncologist

Screening Interval

Screening Interval
 High False-Negative Rate ! ! !")
子宮頸癌發生率趨勢 (美 國) High False-Negative Rate ! ! !

子宮頸癌篩檢率與發生率及死亡率之長期趨勢 , 民國 81 -92年

False-Negative Rate of Pap Smear

False-Negative Rate of Pap Smear
 ¡ Errors in detecting cervical abnormalities ¡")
False-Negative Rate of Pap Smear (10 -55%) ¡ Errors in detecting cervical abnormalities ¡ ¡ ¡ may occur due to barriers to exfoliation or "shedding" of cells from the surface of the cervix Inadequate cell sample collection Omissions or mistakes in transferring cells to a slide Human error in evaluating cancerous cells that are collected

Unfortunately. . . Biochemical Data Show In many instances adhesion molecules persist to surface Non-Shedding Dysplastic Cells Does this affect Pap ? Felix JC, et al. Am J Obstet Gynecol. 2002; 186: 1308 -14.

Screening for Cervical Cancer Effect Skill Cost 2003 HPV testing + Pap smear 1998 Pap. Sure test 1998 automated Pap smear 1996 Thin layer Pap test 1943 Papanicolaou smear 1920 Colposcope

1996 Thin Layer Pap Test

1996 Thin Layer Pap Test

1996 Thin Layer Pap Test

1996 Thin Layer Pap Test

Clinical Outcome Trial of the Thin. Prep® Pap Test

Clinical Outcome Trial of the Thin. Prep® Pap Test Site Total Conventional Pap Smear (n) HSIL + Percent (%) Total Thin. Prep Pap Test (n)* HSIL + Percent (%) Percent Change (%) S 1 2, 439 51 2. 1 1, 218 26 2. 1 +2. 1 S 2 2, 075 44 2. 1 1, 001 57 5. 7 +168. 5 S 3 2, 034 7 0. 3 1, 016 16 1. 6 +357. 6 S 4 2, 043 14 0. 7 1, 000 19 1. 9 +177. 3 S 5 2, 040 166 8. 1 1, 004 98 9. 8 +20. 0 S 6 2, 011 37 1. 8 1, 004 39 3. 9 +111. 1 S 7 2, 221 58 2. 6 1, 000 45 4. 5 +72. 3 S 8 2, 039 61 3. 0 983 44 4. 5 +49. 6 S 9 2, 000 4 0. 2 1, 000 5 0. 5 +150. 0 S 10 2, 015 69 3. 4 1, 000 50 5. 0 +46. 0 Total 20, 917 511 2. 4 10, 226 399 3. 9 +59. 7 (p<0. 001)

Recent independent, multi-study reviews consistent increased detection with the Thin. Prep Pap Test More sensitive and more specific in detecting cervical dysplasia vs. conventional Pap smear METHOD FINDINGS 10 studies published between 1990 -2002 comparing cytology with biopsy-proven diagnosis for 21, 752 patients The Thin. Prep Pap Test showed an 11. 7% increase in sensitivity (76% vs. 68%) and an 8. 9% increase in specificity (86% vs. 79%). "The increased sensitivity of Thin. Prep results in increased cytologic diagnosis of cervical atypia, LGSIL, HGSIL. . . "

Clinical Benefits of Thin Layer Pap Test ¡ More Effective improved the detection of precancerous lesions by 59% in screening populations when compared with the conventional Pap smear ¡ Improved Specimen Quality ¡ Additional Diagnostic Testing ¡ Economic Advantages?

Screening for Cervical Cancer Effect Skill Cost 2003 HPV testing + Pap smear 1998 Pap. Sure test 1998 automated Pap smear 1996 Thin layer Pap test 1943 Papanicolaou smear 1920 Colposcope

1998 Pap. Sure Test ¡ Pap. Sure: Pap. Sure® is the combination of a traditional Pap Smear and a simple visual exam The value of direct visual examination:

1998 Pap. Sure Test

1998 Pap. Sure Test

Clinical Examples of Pap. Sure Test

The results of Pap. Sure Test Pap. Sure has a 99. 1% negative predictive value

The results of Pap. Sure Test ¡ The sensitivity for detecting abnormalities during a cervical screening: 92 percent. ¡ The specificity for detecting abnormalities during a cervical screening: 80 percent. ¡ Greatly reduces false negative rate. ¡ Pap. Sure has a 99. 1 percent negative predictive value Wertlake PT, Francus K, Newkirk GR, Parham GP. Effectiveness of the Papanicolaou smear and speculoscopy as compared with the Papanicolaou alone: A community based clinical trial. Obstet Gynecol. 1997; 90: 421 -427. Loiudice L, Abbiati R, Boselli F, et al. Improvement of Pap smear sensitivity using a visual adjunctive procedure: a cooperative Italian study on speculoscopy (GISPE). Eur J Cancer Prev. 1998; 7: 295 -304. Prev. Wertlake PT, Goodstone G, Gornbein J. Effectiveness of the Pap smear combined with speculoscopy, as compared to the Pap smear alone. A community based clinical trial of 7000 women. Proceedings of speculoscopy, World Congress of Cervical Pathology and Colposcopy, Chicago, Illinois, May 1993. Colposcopy,

The results of Pap. Sure Test

Major disadvantage of Pap. Sure ¡ Relative high percentage of false-positive rate. ¡ Lead to anxiety of the patients and clinicians. ¡ Lead to subsequent unnecessary examinations (colposcopy examination, cervical biopsy, conization……)

Screening for Cervical Cancer Effect Skill Cost 2003 HPV testing + Pap smear 1998 Pap. Sure test 1998 automated Pap smear 1996 Thin layer Pap test 1943 Papanicolaou smear 1920 Colposcope

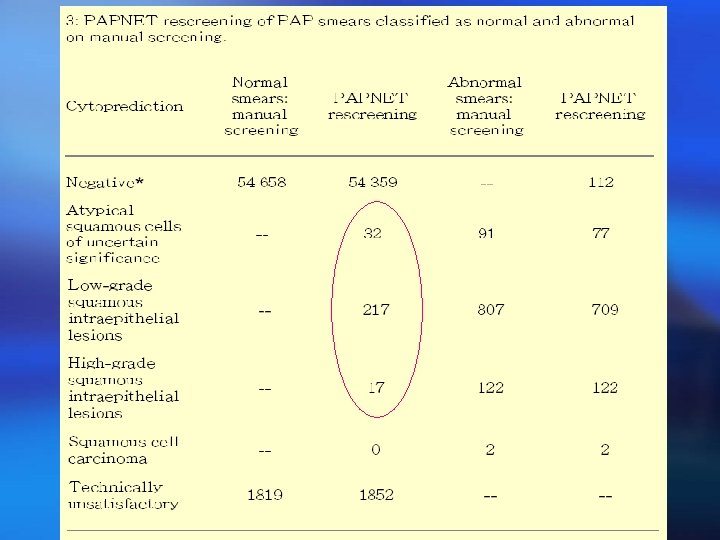
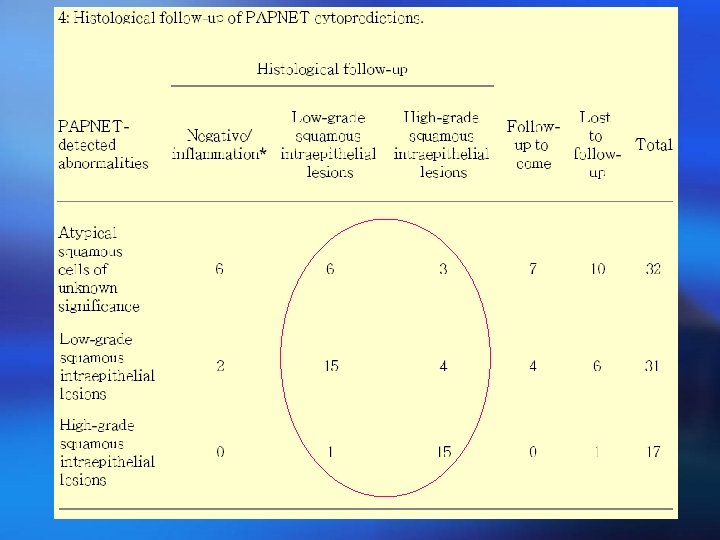
1998 Automated Pap Smears Computerized Screener ¡ The automated screening system detects higher numbers of abnormal PAP smears than manual screening ¡ A study conducted at the IMVS further confirmed the value of computerized rescreening for the detection of false negative cases Annabelle Farnsworth, Fay M Chambers and Colin S Goldschmidt. Evaluation of the PAPNET system in a general pathology service. MJA 1996; 165: 429 -431 Stevens MW, Milne AJ, James KA, Brancheau D, Ellison D, Kuan L. Effectiveness of Automated Cervical Cytology Rescreening Using the Auto. Pap 300 QC System. Diagn Cytopathol 1997; 16: 505 -512

1998 Automated Pap Smears Computerized Screener

Screening for Cervical Cancer Effect Skill Cost 2003 HPV testing + Pap smear 1998 Pap. Sure test 1998 automated Pap smear 1996 Thin layer Pap test 1943 Papanicolaou smear 1920 Colposcope

HPV prevalence in general population ¡ 600 female university students who were tested every 6 months for high risk HPV. ¡ Over the course of 3 years, new HPV infections occurred in more than 40% of the women. ¡ Most infections lasted about 8 months and then subsided. ¡ About 10% of the women: persistent infection. Groopman 1999

HPV prevalence in general population ¡ Typical prevalence of HPV for women under the age of 25 is between 28 and 46 percent. (Burk, 1996; Bauer, 1991) ¡ Prevalence of HPV infection for women of all ages is about 20% in Southern Taiwan. (4570 cases) (Lin et al, 2006)

HPV persistent infection • A total of 1611 women with no cytological lesions. • Pap smear cytology and HPV testing every 4 months in the first year and twice yearly thereafter. • Rate of SIL: 0. 73/1000 among women free of HPV at the 2 initial visits. • Rate of SIL: 8. 68/1000 among women with HPV infections persisting over both visits. A strong relationship exists between persistent HPV infections and SIL incidence. JAMA 2001; 286: 3106 -14

HPV persistent infection HPV 16 or 18 plus other HPV types 0. 50 0. 45 HPV 16 or 18 only 0. 40 0. 35 Cumulative Proportion 0. 30 0. 25 0. 20 0. 15 0. 10 HPV Negative 0. 05 0 0 4 8 12 16 20 months Source: Koutsky et al. , New England Journal of Medicine 1992 24

HPV prevalence in cervical neoplasm ¡ HPVs can be identified in 90% patients of CIN. Lorincz et al. Obstet Gynecol 1992; 79: 328 -37. ¡ High-risk HPVs can be identified in 96. 4~99. 7% patients of invasive carcinoma. Judson 1992; Walboomers et al 1999 ¡ Our data for high-risk HPV: Cx ca 96. 4%, CIN 89. 7% Lin et al, Gynecol Oncol 2005.

HPV type and Cervical Cancer

HPV type and Cervical Cancer HPV type %Ca 16 45 52 58 59 56 68 53. 6 0. 0 7. 2 0. 0 %Ca 18 31 33 35 51 39 Lin et al. Gynecol Oncol 2005 18. 0 0. 0 10. 8 3. 6 0. 0 HPV type

Primary Screening ¡ 8554 women in Costa Rica. ¡ Hybrid Capture II, which detect HPV DNA. ¡ Using an HPV level of 1 pg/ml (1 picogram of HPV DNA per milliliter of solution) as cutoff point. ¡ Sensitivity for detecting CIN 88. 4%; cancer 100%. ¡ Specificity 89%. Source: JAMA, 2000; 283: 87 -93
")
Primary Screening ¡ 7932 women who had routine cervical examination ¡ ¡ ¡ (HC-II) Sensitivity for detecting HSIL: HPV: 100%. Conventional pap: 68. 1%. Thin-layer cytology: 87. 8%. Specificity for detecting HSIL: HPV all age: 85% HPV age >30: 90% HPV testing could be proposed in primary screening in association with cytology. Source: British Journal of Cancer 2001; 84: 1616 -23.

HPV Testing and Cervical Cytology For Screening in Women Aged ≥ 30 Source: Obstet Gynecol 2004; 103: 304 -9

FDA Approves Expanded Use of HPV Test : 2003 March ¡ The new indication allows the test to be used for screening, in conjunction with the Pap test, of women over age 30 for HPV infection. ¡ The HPV DNA test is not intended to substitute for regular Pap screening. Nor is it intended to screen women under 30 who have normal Pap tests. ¡ Most infections in women <30 y/o are shortlived and not associated with cervical cancer.

HPV testing together with Pap: An alternative for screening ¡ Pap smear normal + negative HPV: are at virtually no risk of developing cervical cancer or a high-grade precursor in the next 5 to 10 years (assuming no new sexual partners). ¡ Pap smear normal + positive HPV: repeat HPV test 6 -12 months later.
")
國家衛生研究院 臺灣癌症 臨床研究合作組織 (2004 年版 )

Evaluation of Self-Collected Cervicovaginal Cell Samples for Human Papillomavirus Testing Patti E. Gravitt, James V. Lacey, Jr. , Louise A. Brinton, Willard A. Barnes, Janet R. Kornegay, Mitchell D. Greenberg, Sarah M. Greene, Olympia C. Hadjimichael, Larry Mc. Gowan, Rodrique Mortel, Peter E. Schwartz, Richard Zaino, Allan Hildesheim Cancer Epidemiology, Biomarkers & Prevention. Vol. 10, 95– 100, February 2001

Agreement of HPV results between self-collected and clinician-collected swabsa Clinician-collected swab HPV Clinician-collected swab positive negative Total Self-administered HPV positive Self-administered HPV negative 74 18 92 14 162 176 Total 88 180 268 a Percentage of agreement, 236 of 268 (88. 1%); percentage of agreement among positives, 74 of 106 (69. 8%); κ= 0. 73 (95% CI: 0. 61– 0. 85).

Thomas C. Wright, Jr. HPV DNA Testing of Self-collected Vaginal Samples Compared With Cytologic Screening to Detect Cervical Cancer. JAMA. 2000; 283: 81 -86

John W. Sellors et al. Comparison of self-collected vaginal, vulvar and urine samples with physician-collected cervical samples for human papillomavirus testing to detect high-grade squamous intraepithelial lesions. CMAJ 2000; 163(5): 513 -8

Self-Collected Cervicovaginal Cell Samples for Human Papillomavirus Testing

Comparison of Different Screening Modalities Method Pap smear Thin. Prep Pap. Sure Pap. Net HPV test Pap+HPV Sensitivity Specificity Cost CGMH
.")
Current Goals of Cervical Cancer Prevention ¡ Education. ¡ Increase screening rate (25% 70~80%). ¡ Increase screening accuracy.

台灣地區子宮頸抹片篩檢之參與率

Causes of low screening rate in Taiwan 35% 太忙沒空 再怎麼忙一年有超過 的沒空嗎? 100 天的週末真 23% 害怕內診 有護士跟診,也有女醫師,別怕! 16% 自己覺得很健康沒 必要 幾乎所有的新病例都是沒做過抹片的。 13% 不好意思 為了健康,請相信醫療專業。 11% 到醫院太麻煩 醫院診所都有假日門診,而且做抹片 免掛號。 11% 不了解抹片是什麼 真的沒聽過 6 分鐘護一生嗎?


Dr. Hao Lin Assistant Professor Division of Gynecologic Oncology OBS & GYN Dept. Chang Gung Memorial Hospital
6a24261ae98758e4671c02a459504400.ppt