

3cb3d2cf492f0785cde635832f0ae115.ppt
- Количество слайдов: 23
 MENTAL HEALTH POLICY IN RWANDA: The local responses and challenges. Prof. Eugene Rutembesa University of Rwanda
MENTAL HEALTH POLICY IN RWANDA: The local responses and challenges. Prof. Eugene Rutembesa University of Rwanda
 • 23 years ago each April from 7 th to 13 th is the week period of genocide commemoration. ( Mourning week). • Many people are deeply affected ( emotionally, affectively and psychologically due to remembering the darkness period of 1994. ( 100 days of darkness)>
• 23 years ago each April from 7 th to 13 th is the week period of genocide commemoration. ( Mourning week). • Many people are deeply affected ( emotionally, affectively and psychologically due to remembering the darkness period of 1994. ( 100 days of darkness)>
 1. 074.") 1. Background: 1 out of 4 children is an orphan (census, 2005) 1. 074. 017 people killed (1/7 of the population) Genocide 1994 0. 6 to 1 million from exile (30 years) CAME IN 1. 951. 388 accused of participation (2/7) 2. 5 millions exile after the genocide, WENT OUT A mixture of situations that have in common to be highly
1. Background: 1 out of 4 children is an orphan (census, 2005) 1. 074. 017 people killed (1/7 of the population) Genocide 1994 0. 6 to 1 million from exile (30 years) CAME IN 1. 951. 388 accused of participation (2/7) 2. 5 millions exile after the genocide, WENT OUT A mixture of situations that have in common to be highly
 Trauma and other commorbidities The concept of trauma comes of the Greek " Traumatismos ": action to wound, injury. Transmission of a psychic shock, psychological modification. Trauma is disconnecting the victim ( thoughts, feelings and environment). N. Munyandamutsa et all. (2011) PTSD: 28, 54 % Depression: 54% /PTSD, – Alcoholism 10% /PTSD, – Somatoform disorder ( headach) 71%/ PTSD.
Trauma and other commorbidities The concept of trauma comes of the Greek " Traumatismos ": action to wound, injury. Transmission of a psychic shock, psychological modification. Trauma is disconnecting the victim ( thoughts, feelings and environment). N. Munyandamutsa et all. (2011) PTSD: 28, 54 % Depression: 54% /PTSD, – Alcoholism 10% /PTSD, – Somatoform disorder ( headach) 71%/ PTSD.
 Genocide against Tutsi chaos Devastating Psycho-trauma reconstruction actions.
Genocide against Tutsi chaos Devastating Psycho-trauma reconstruction actions.
 1995 2014 Psychiatrists 1 7 Psychologists 5 599 Psychiatric nurses 3 348 11. 3 million residents (2012)
1995 2014 Psychiatrists 1 7 Psychologists 5 599 Psychiatric nurses 3 348 11. 3 million residents (2012)
 Appui au desk: Assist Technique Planification Équipements Fonctionnement Politique Nationale de SM PNSM Sensibilisation Deuil National AS SIS TA E TE CH NI QU E Services nationaux de référence POSM* 1 POSM 2 POSM 3 POSM 4 POSM 5 POSM 6 HD HD Interventions dans la communauté • POSM: pôles opérationnels de santé mentale • HD: Hôpitaux de district HD HD Supervision Médicaments Équipements Fonctionnement Formation spéci Supervision Médicaments POSM: Réhabilitation Équipements Formation Activités Formation A S
Appui au desk: Assist Technique Planification Équipements Fonctionnement Politique Nationale de SM PNSM Sensibilisation Deuil National AS SIS TA E TE CH NI QU E Services nationaux de référence POSM* 1 POSM 2 POSM 3 POSM 4 POSM 5 POSM 6 HD HD Interventions dans la communauté • POSM: pôles opérationnels de santé mentale • HD: Hôpitaux de district HD HD Supervision Médicaments Équipements Fonctionnement Formation spéci Supervision Médicaments POSM: Réhabilitation Équipements Formation Activités Formation A S
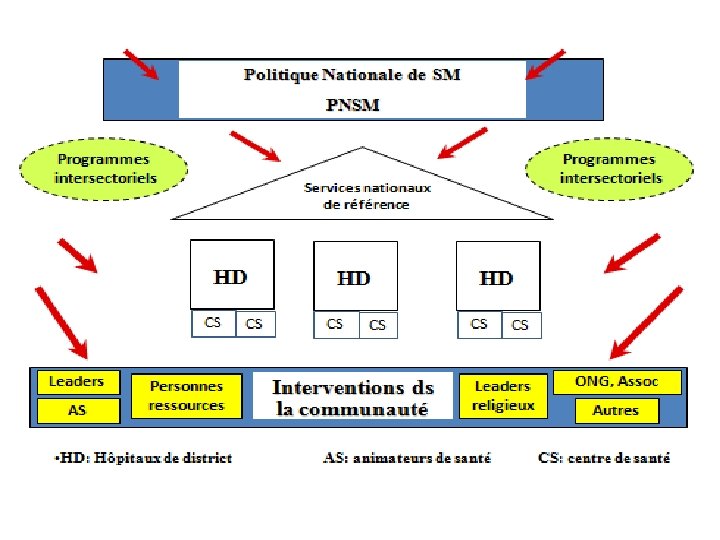
 The Sector is the focal point where the population receives services and where is organized the Community participation, with the collection of information. The Cell is responsible for the assessment the needs and their priorisation as well as mobilization of the Community actions. Finally, “Umudugudu” is in charge of the construction of the co-operation and solidarity between the members with the community.
The Sector is the focal point where the population receives services and where is organized the Community participation, with the collection of information. The Cell is responsible for the assessment the needs and their priorisation as well as mobilization of the Community actions. Finally, “Umudugudu” is in charge of the construction of the co-operation and solidarity between the members with the community.
 Lacement des mutuelles de santé
Lacement des mutuelles de santé
 Psychotropics 13
Psychotropics 13
 • Antidepressant") Psychotropic drugs used • Neuroleptics or anti psychotropics (psychotic and behavor’s disorders) • Antidepressant (depression and Obsessivecompulsive disorder). • Anti-anxiety ( anxiety) • Thymoregulators ( Mood stabilizer) • During commemoration: prescription of anxiolytics et sedatives ( reduce the pain).
Psychotropic drugs used • Neuroleptics or anti psychotropics (psychotic and behavor’s disorders) • Antidepressant (depression and Obsessivecompulsive disorder). • Anti-anxiety ( anxiety) • Thymoregulators ( Mood stabilizer) • During commemoration: prescription of anxiolytics et sedatives ( reduce the pain).
. • Psychiatrists ( 11) most of them in RH •") Available resources ( 2015). • Psychiatrists ( 11) most of them in RH • Clinical psychologists ( 10 with Ph. D’s and different orientations (UR); 30 with masters and 2000 undergraduate degree; • Psychiatric nurses around ( 600) • Social workers ( from former NUR) • Medical doctors ( some of them trained to diagnosis and treat mental illnesses. • Creation of department of Psychiatry ( 2014).
Available resources ( 2015). • Psychiatrists ( 11) most of them in RH • Clinical psychologists ( 10 with Ph. D’s and different orientations (UR); 30 with masters and 2000 undergraduate degree; • Psychiatric nurses around ( 600) • Social workers ( from former NUR) • Medical doctors ( some of them trained to diagnosis and treat mental illnesses. • Creation of department of Psychiatry ( 2014).
 Academic training in mental Health 1. Training of clinical psychologist: Since 1999 graduands with bachelor’s degree (541). 2. Masters in clinical psychology 2008: 15 in 2015 were (30). 3. Department of the social workers: Faculty of political and social Sciences(600 graduands) ;
Academic training in mental Health 1. Training of clinical psychologist: Since 1999 graduands with bachelor’s degree (541). 2. Masters in clinical psychology 2008: 15 in 2015 were (30). 3. Department of the social workers: Faculty of political and social Sciences(600 graduands) ;
: Since 1998, trained the nurses (A 1) in mental health") Kigali Health Institute (KHI): Since 1998, trained the nurses (A 1) in mental health (600 graduans); 8. In the private sector, INATEK developed a program of clinical psychology. It is similar of the NUR (500). 9. Vocational training of the counselling with the KHI.
Kigali Health Institute (KHI): Since 1998, trained the nurses (A 1) in mental health (600 graduans); 8. In the private sector, INATEK developed a program of clinical psychology. It is similar of the NUR (500). 9. Vocational training of the counselling with the KHI.
 developed a Professional program to train") Professional training • Trauma Counsellor Rwandan Association (ARCT-Ruhuka) developed a Professional program to train counsellors from different Associations ( 1 year). Exit profile: certificate in trauma counselling (115). ( active listening). • Community approach: sector, cell and umudugudu. ( Psychosocial Assistant ( APS) (11000 -12 000). decentralisation
Professional training • Trauma Counsellor Rwandan Association (ARCT-Ruhuka) developed a Professional program to train counsellors from different Associations ( 1 year). Exit profile: certificate in trauma counselling (115). ( active listening). • Community approach: sector, cell and umudugudu. ( Psychosocial Assistant ( APS) (11000 -12 000). decentralisation
 REALITIES AND CHALLENGES Challenges • Medicalization of mental health services. No recognized status of psychologist; ( DH). • Need to engage psychologists (in D H, prisons, HC). . . ; • Even at the University level, psychology is not considered as priority; consequently research is not encouraged in domain. • Lack of collaboration between civil society, university and Ministry of Health.
REALITIES AND CHALLENGES Challenges • Medicalization of mental health services. No recognized status of psychologist; ( DH). • Need to engage psychologists (in D H, prisons, HC). . . ; • Even at the University level, psychology is not considered as priority; consequently research is not encouraged in domain. • Lack of collaboration between civil society, university and Ministry of Health.
 Strengths • A national program of Mental Health; • Initiatives taken by civil society; • Implication of the universities in training ( public and private universities). • Increasing number of professionals ( psychiatrists, psychologists, counsellors…). • Developing the collaborations with outside universities ( France, Belgium, Canada, Italy…).
Strengths • A national program of Mental Health; • Initiatives taken by civil society; • Implication of the universities in training ( public and private universities). • Increasing number of professionals ( psychiatrists, psychologists, counsellors…). • Developing the collaborations with outside universities ( France, Belgium, Canada, Italy…).
 Conclusion • After the genocide against Tutsi 1994, the mental health was introduced like priority of health. • Several years after the genocide, in Rwanda the mental health remains always a priority of public health and risk to still remain it during several years.
Conclusion • After the genocide against Tutsi 1994, the mental health was introduced like priority of health. • Several years after the genocide, in Rwanda the mental health remains always a priority of public health and risk to still remain it during several years.
 • The mental health was classified in the primary education care at the ministry for health; • Unfortunately, a great number of psychologists and social workers remains jobless. ( The place of psychologist is not well defined).
• The mental health was classified in the primary education care at the ministry for health; • Unfortunately, a great number of psychologists and social workers remains jobless. ( The place of psychologist is not well defined).
 23") Thank you for your attention 2018/3/17 jrnk, Rwanda (NAU, 30 Aug 05) 23
Thank you for your attention 2018/3/17 jrnk, Rwanda (NAU, 30 Aug 05) 23