774db697a34f79bd4aa495fc8ef0d48e.ppt
- Количество слайдов: 53



Medicines Reimbursement and funding arrangements in Europe Multicountry meeting of the Visegrad group countrieson reimbursement and pricing of drugs Warsaw, October 29 -30, 2007 Kees de Joncheere WHO Regional Office for Europe

Overview n Health and health care in Europe : some data n Pharmaceutical figures in Europe n Pharmaceutical policies and strategies on improving use and containing costs n Challenges and conclusions

Functions and objectives of a health system Functions the system performs Objectives of the system Stewardship (oversight) Responsiveness (to people’s non-medical expectations) Creating resources Delivering services (investment and training) (provision) Health Fair Financing(collecting, pooling and purchasing) (financial contribution)
 Source: PPRI")
Total Pharmaceutical Expenditure per capita in Euro-PPP 2005 PPRI ( source PPRI) Source: PPRI 2006
 § European averages § 18.")
Pharmaceutical Expenditure in % of Health Expenditure (2005, PPRI) § European averages § 18. 6% § EU-15: 15. 6 % § § EU-25: EU-10: 23. 7% Member States differences § <= 10%: LU, DK, IE, NL; NO § => 25%: BG, HU, LT, PL, SI, SK

WHO pays ? n Public health expenditure as % total health expenditure ä EU-25: 74 % ä EU-15: 78 % ä EU-10: 70 % Source : PPRI
")
Medicines expenditures OECD countries (2004)

Who pays ? options and issues n Tax based n Compulsory health insurance n Private out of pocket n Private or complementary insurance Considerations n Fiscal sustainability of the system n Equitable access for patients n Protection against catastrophic costs of illness

Goals for pharmaceutical policies in Europe n Equitable access for patients to effective, safe and good quality medicines n Enhancing appropriate use of medicines for better health outcomes n Ensuring value for money n Balance with industrial policy objectives n Underpinning values : equity, solidarity, access, quality, participation

“Equity” as value in the goals for pharmaceutical policies in Europe In-equality means differences in health and access to health care that are considered n Unnecessary n Avoidable n Unfair n Unjust

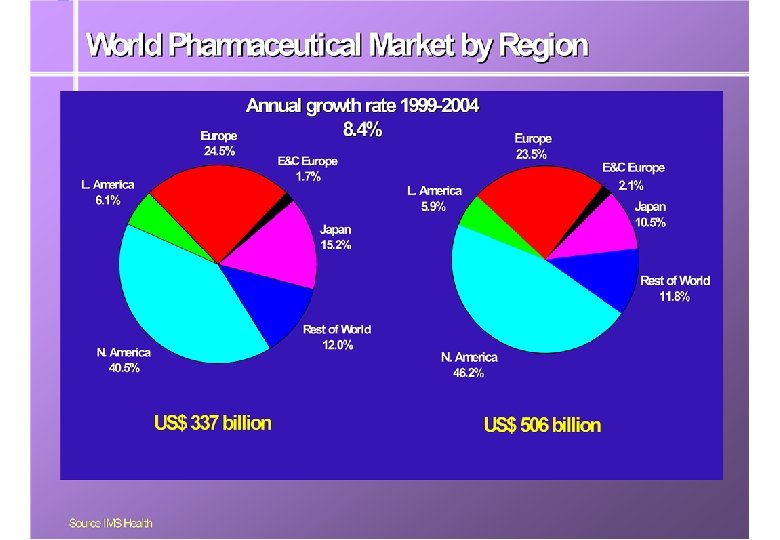
The rising costs on medicines Higher volumes and higher price component Ø Ageing Ø Shift to new medicines in same therapeutic category Ø New drugs for prevention, and for diseases that could not be treated e. g. AIDS, MS Ø “Life-style drugs” Ø Hospital - primary care shifts Ø especially for Eastern Europe : increase public coverage and close treatment gap

A changing pharmaceutical policy panorama q. Till 1995 § Patent = Innovation = Premium Price q Over the last years § Cost containment focus § More cost – effectiveness evaluations and HTA § International price referencing § Therapeutic price referencing § Additional market access hurdles q Concern over decreasing innovation

R&D spending increases but number of NMEs approved not increasing

Mind the gap n Public finance cannot keep up with increase in drug expenditures n Options for policy-makers ä Increase health budgets : funding from …? ä Limit range of drugs to be reimbursed : cave medical need and quality treatment ä Increase efficiency ( regulation of prices, prescribing, use, …) : requires sustainable funding and programmes ä Shift expenditures to patients : equity, solidarity …?

Improving the use of medicines and containing costs n Education and information n Managerial and administrative measures n Financial measures

Pharmaceutical policies and the EU n One EU regulatory framework and legislation (including EMEA in London) ä n Review 2003, in force 2005 National responsibilities on pricing and reimbursement (“subsidiarity”), but ä Transparency directive ä DG Health - High Level Pharma committee, ä G 10 ä Pharmaceutical Forum
")
Selecting medicines for reimbursement n Prof. Don Birkett ( former chair of PBAC Australia) ä “If you are going to buy a car, it makes sense to take a look at it first”

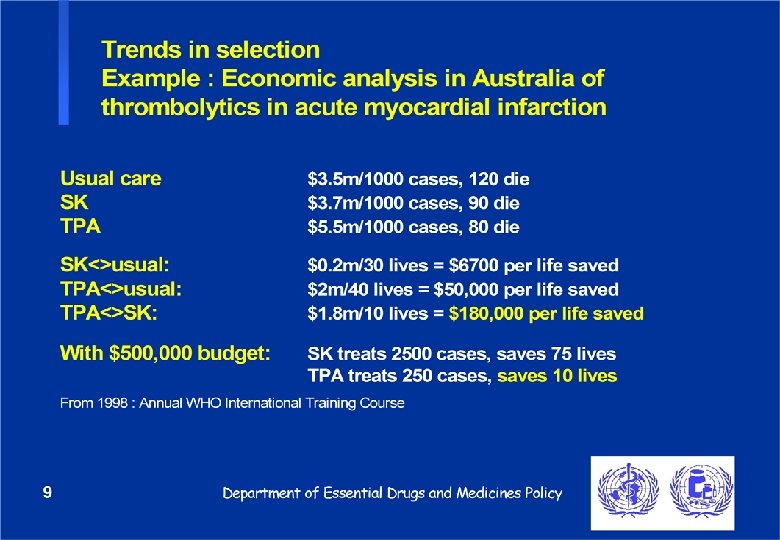
Increasing use of strategies to select medicines for public provision n n n n Positive list for reimbursement ( NL, DK, Swe, …) Reference pricing, with generic or therapeutic groups (D, Ita, NL, Por, Rom, …) Differential reimbursement % ( Fr, Bul, …) Economic evaluation of medicines ( Fin, NL, Swe, UK, …) Promote use of generics ( UK, D, Fr, …) Co-payment mechanism (DK, N, Esp, …) Standard treatment guidelines (UK, DK, Esp, …) …
 n For market entry : ä n")
Evaluation criteria and medical decision making (1) n For market entry : ä n quality, efficacy, safety For reimbursement ä Medical need ä Health gain and added therapeutic value ä Cost-effectiveness ä Budget impact ä Equity considerations ä …
 n For medical practice ä Evaluation by")
Evaluation criteria and medical decision making (2) n For medical practice ä Evaluation by drug bulletins, professional associations on the “place in therapy” of a new medicine ä Consistency between reimbursement indications and therapeutic guidelines ? ä Reviews by national HTA commissions
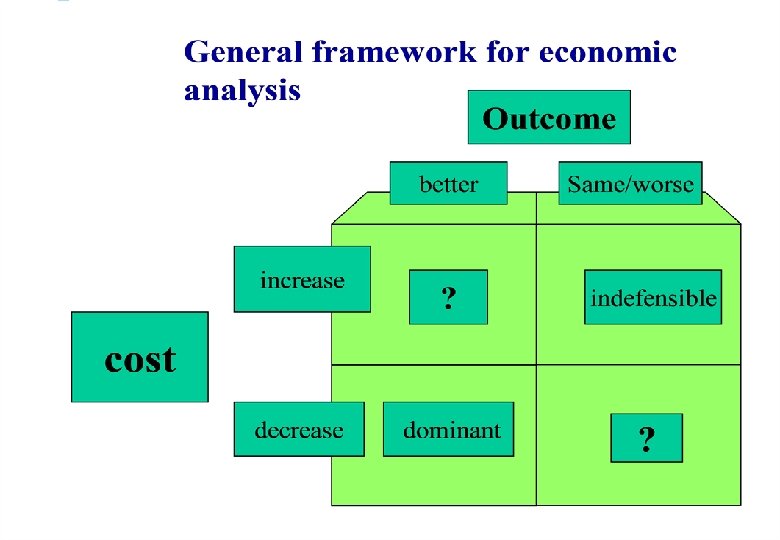

Implications of cost-effectiveness analysis n Health-based reason to justify a price premium for the proposed drug n Relate extent and nature of health gain to justify price increase, including cost off-sets in health sector n Common outcome measure (QALY, life year gained, . . ) n Pristine value judgement

Economic evaluations n Two main approaches ä ä n on a “cost-minimisation” basis as “acceptably cost-effective” Two main “levers” ä restrict to particular patients ä price of the proposed drug

Reimbursement decision-making process : after the initial reimbursement decision … n Post-listing reviews (at least annually) ä ä n prices restrictions and listings Post-listing monitoring (at least annually) ä ä n usage (including predicted versus actual) cost to reimbursement system Coordinate post-listing activities
 (1) § § §")
Compilation of problems countries encountered with pharmaco-economic evaluations (WHO 2000) (1) § § § No references to source of data § § Lack of transparency in economic modelling Study design and methodology not clearly described Differences in time measurement for the new and the standard treatment Not relevant in the context of criteria for reimbursement
 (2) n Population that")
Compilation of problems countries encountered with pharmaco-economic evaluations (WHO 2000) (2) n Population that was most likely to use the treatment not adequately identified and described n No head-to-head trials, or inappropriate comparators n Relevance of outcomes worth paying for ? surrogate and final outcomes n Sensitivity analyses not performed
 n Separate licensing and reimbursement decisions n Positive list")
Making cost-effectiveness evaluations work (1) n Separate licensing and reimbursement decisions n Positive list n Price negotiations n Ability to restrict indications n Adequate guidelines for submissions n Competent evaluations of submissions n Consistent and informed decision-maker
 n Inclusiveness in decision-making and input")
Making cost-effectiveness evaluations work : decision-making process (2) n Inclusiveness in decision-making and input from all stakeholders n Reimbursement committees with external experts : managing potential conflict-of-interests n Health Technology Assessment agencies and committees often not directly linked with reimbursement decisions

International collaboration on evaluation of medicines n Each health care system different ä ä n different levers different solutions Problems tend to be the same ä ä n similar cost drivers similar evidence Basis for common guidance, and exchange of information, and “lessons learned” ? !

Conclusion and challenge : promote efficiency, maintain equity § Reaffirm goals and values of health systems and pharmaceutical policies : quality treatment at affordable cost, as needed § Be selective – need and efficiency – on which medicines get reimbursed § Enhance the use of generics § Strengthen appropriate prescribing § Increase efficiency and negotiation capacity of buyers, while protecting patients § Shift to reference pricing schemes § Networking among authorities

http: //www. who. int / medicines http: //euro. who. int/pharmaceuticals Thank you

Slides for discussion
 n Profit control ä ä Voluntary arrangement ä Innovative drugs ä")
Price regulation (1) n Profit control ä ä Voluntary arrangement ä Innovative drugs ä Claw back ä n F. e. UK PPRS, Free prices Price - volume arrangements
 n Regulating distribution margins ä In Europe, pharmacies 10 -30% and")
Price regulation (2) n Regulating distribution margins ä In Europe, pharmacies 10 -30% and wholesalers 1 -10% ä Use degressive margins ä How to deal with rebates and discounts ?
 n Cost-plus pricing (ask companies for information on production costs) ä")
Price regulation (3) n Cost-plus pricing (ask companies for information on production costs) ä ä n How to get real data ? How to deal with overheads ? Price reductions, price freezes
 n International price referencing ä ä Which drugs (innovators, generics) ä")
Price regulation (4) n International price referencing ä ä Which drugs (innovators, generics) ä n Which countries How to calculate ( average, lowest ? ) Internal reference pricing / value based pricing ä Relate price to expected benefit ä Compare with other drugs in same class
")
Patented medicines prices in selected countries (2004)

Importance of promoting national strategies for the use of generic medicines n Efficiency savings through price competition n Improve health care affordability and close treatment gap n Headroom for innovation n Appropriate use by avoiding interaction and double medication

Making national strategies on the use of generic medicines work § Supportive legislation and regulation, e. g. Bolar, fees, generic substitution, … § Reliable quality assurance : a credible, effective European regulatory system § Professional and public acceptance, e. g. university education, patient information § Economic incentives, e. g. dispensing fees v. margins, % generic prescribing, reference pricing

International differences in antibiotic consumption Outpatient antibiotic sales in 1997 in the European Union Cars et al Lancet 2001

Disease impact and reimbursement – beyond DALYs and QALYs and value considerations n Favouring survival over quality of life n Favouring ‘severe’ diseases n ‘Rule of rescue’ n ‘Fair innings’ n Culpability / fault issues n Favouring economically productive n Potential for misuse / “leakage”

Use of cost-effectiveness analysis in reimbursement in Europe n CEA needs to relate to goals, values, and priorities of the health care systems n Growing requirements and increasing need for resources n RCTs do not provide all information needed n How to deal with “point-decisions” vis-à-vis re-assessment of the evidence ? n Major difficulties in implementation of CEA decisions in the health care environment ; “silo-budgeting” limits application n Shift to conditional reimbursement with prospective trials : from paying for the medicine to buying an agreed upon therapeutic outcome

Aims of the Networking agreement § Better information for better decisions at national level § Efficiency gains § Learning from good experiences on medicines reimbursement policies and pricing regulations § Potential to contribute to better insight in access to medicines, medicines use and population health outcomes § Support policy makers, scientific community, all stakeholders in pharma-policy development

Networking agreement § Clinical effectiveness evaluations § Price and pricing information § Country pharmaceutical profiles § Website / Portal for competent authorities § Permanent secretariat , modelled after “Heads of Agencies” § Annual meetings § Working groups
 § Medicines evaluation for")
Proposal : Information exchange on clinical effectiveness evaluation (“extended MEDEV”) § Medicines evaluation for reimbursement - first assessment - post-listing review § Discuss guidelines for medicines assessment § Discuss criteria for re-assessment § Discuss criteria for therapeutic equivalence and interchangeability ( reference pricing ? )

Proposal : make price information available § Exchange information on prices § Linking national sites via website portal § National sites with - Pricing structure - Search function ( per active ingredient, ATC group) § Build on DG SANCO funded PPRI - project

PPRI Pharmaceutical country profiles § Making DG SANCO funded PPRI project sustainable § A “living” web-based overview of national pharmaceutical policy, maintained by the competent national authority
774db697a34f79bd4aa495fc8ef0d48e.ppt