

50497670df40fb2d6f88b977131a4173.ppt
- Количество слайдов: 65
 Medical-Legal Partnerships: From Idea to Reality to Changing Pediatric Practice November 3, 2015 Molly Senn-Mc. Nally, M. D. Assistant Professor of Pediatrics Baystate Medical Center Tufts University School of Medicine Jay E. Sicklick, J. D. Clinical Instructor, Department of Pediatrics Univ. of Connecticut School of Medicine Deputy Director, Center for Children’s Advocacy Director – Medical-Legal Partnership Project mlpp
Medical-Legal Partnerships: From Idea to Reality to Changing Pediatric Practice November 3, 2015 Molly Senn-Mc. Nally, M. D. Assistant Professor of Pediatrics Baystate Medical Center Tufts University School of Medicine Jay E. Sicklick, J. D. Clinical Instructor, Department of Pediatrics Univ. of Connecticut School of Medicine Deputy Director, Center for Children’s Advocacy Director – Medical-Legal Partnership Project mlpp
 Disclosure & Accreditation Acknowledgement is made on behalf of the Department that: There is no commercial support for this Grand Rounds. Confirmation is also made that today’s lecture and faculty disclosure have been peer reviewed and there are no conflicts of interest. mlpp
Disclosure & Accreditation Acknowledgement is made on behalf of the Department that: There is no commercial support for this Grand Rounds. Confirmation is also made that today’s lecture and faculty disclosure have been peer reviewed and there are no conflicts of interest. mlpp
 Presentation Goals o Define poverty and provide an overview of critical social determinants of health o Introduce Medical Legal Partnerships (MLPs) o Examine how MLPs address childhood adversities that affect health o Utilize cases to demonstrate MLP intervention and strategies o Translate advocacy skills to everyday practice mlpp
Presentation Goals o Define poverty and provide an overview of critical social determinants of health o Introduce Medical Legal Partnerships (MLPs) o Examine how MLPs address childhood adversities that affect health o Utilize cases to demonstrate MLP intervention and strategies o Translate advocacy skills to everyday practice mlpp
 Two Cases In a Day What Would You Do? mlpp
Two Cases In a Day What Would You Do? mlpp
 Case #1: Asthma mlpp
Case #1: Asthma mlpp
 Case #1: Asthma o 12 year old patient w/asthma o Treated in PCP’s office and medically stable o Adherent with treatments, but returns to office frequently with acute attacks o Father notes that house is infested with roaches and is moldy due to leaking water, yet landlord refuses to address complaints What Would You Do? mlpp
Case #1: Asthma o 12 year old patient w/asthma o Treated in PCP’s office and medically stable o Adherent with treatments, but returns to office frequently with acute attacks o Father notes that house is infested with roaches and is moldy due to leaking water, yet landlord refuses to address complaints What Would You Do? mlpp
 Case #2: Expulsion mlpp
Case #2: Expulsion mlpp
 Case #2: Expulsion o 7 year old patient whose parent calls PCP complaining that child has been suspended “again” (third out-of-school suspension in four months) o Now principal stating that child no longer welcome in school, although tutoring at home will be provided until child is “in control” What Would You Do? mlpp
Case #2: Expulsion o 7 year old patient whose parent calls PCP complaining that child has been suspended “again” (third out-of-school suspension in four months) o Now principal stating that child no longer welcome in school, although tutoring at home will be provided until child is “in control” What Would You Do? mlpp
 Knowing the Territory
Knowing the Territory
 What is Poverty? o Definition – US Dept. of Health and Human Services federal poverty level (“FPL”) o Family of three - What’s your guess? n n $19, 130 $20, 090 $22, 616 $24, 854 ANSWER: $20, 090 mlpp Source: Federal Register. 80 FR 3236. Jan. 22, 2015
What is Poverty? o Definition – US Dept. of Health and Human Services federal poverty level (“FPL”) o Family of three - What’s your guess? n n $19, 130 $20, 090 $22, 616 $24, 854 ANSWER: $20, 090 mlpp Source: Federal Register. 80 FR 3236. Jan. 22, 2015
?") Poverty Quiz o What is the child poverty rate in Massachusetts (children under 18)? n n 8% 11% 14% 17% ANSWER: 11% mlpp U. S. Census Bureau American Community Survey 2009 -13
Poverty Quiz o What is the child poverty rate in Massachusetts (children under 18)? n n 8% 11% 14% 17% ANSWER: 11% mlpp U. S. Census Bureau American Community Survey 2009 -13
 Poverty Quiz o What is the poverty rate for children under the age of 18 in Springfield (2009 -13)? n n 13% 21% 27% 44% ANSWER: 44% mlpp U. S. Census Bureau American Community Survey 2009 -13
Poverty Quiz o What is the poverty rate for children under the age of 18 in Springfield (2009 -13)? n n 13% 21% 27% 44% ANSWER: 44% mlpp U. S. Census Bureau American Community Survey 2009 -13
 Poverty Quiz o What was the birthrate/1000 of teen mothers, ages 15 -17 years, in Springfield (2013)? n n 26. 1 38. 6 42. 3 55. 7 ANSWER: 42. 3 mlpp Source: Mass. Dept. of Public Health (Dec. 2014)
Poverty Quiz o What was the birthrate/1000 of teen mothers, ages 15 -17 years, in Springfield (2013)? n n 26. 1 38. 6 42. 3 55. 7 ANSWER: 42. 3 mlpp Source: Mass. Dept. of Public Health (Dec. 2014)
 Poverty Quiz o What was the birthrate/1000 of teen mothers, ages 15 -17 years, in Longmeadow (2013)? n n 0 4 8 12 ANSWER: 0 mlpp
Poverty Quiz o What was the birthrate/1000 of teen mothers, ages 15 -17 years, in Longmeadow (2013)? n n 0 4 8 12 ANSWER: 0 mlpp
 Poverty Quiz o What is the percentage of eligible children in Mass who are enrolled in either Medicaid or CHIP? n n 72. 1 84. 7 88. 2 96. 8 ANSWER: 96. 8 mlpp CMS Monthly Applications June 2015
Poverty Quiz o What is the percentage of eligible children in Mass who are enrolled in either Medicaid or CHIP? n n 72. 1 84. 7 88. 2 96. 8 ANSWER: 96. 8 mlpp CMS Monthly Applications June 2015
 The Case for Social Determinants
The Case for Social Determinants
 Fundamental Needs for Children o Peace o Shelter o Education o Food o Income o Social Justice o Equity mlpp Source: World Health Org. Ottawa Charter for Health Promotion (1986)
Fundamental Needs for Children o Peace o Shelter o Education o Food o Income o Social Justice o Equity mlpp Source: World Health Org. Ottawa Charter for Health Promotion (1986)
 mlpp Us Census Bureau American") Springfield Poverty and Unemployment Rates by Race/Ethnicity (2007 -11) mlpp Us Census Bureau American Community Surveys 2006 -10 (Poverty), 2007 -11 (Unemployment)
Springfield Poverty and Unemployment Rates by Race/Ethnicity (2007 -11) mlpp Us Census Bureau American Community Surveys 2006 -10 (Poverty), 2007 -11 (Unemployment)
 Springfield Education Level by Race/Ethnicity, 2006 -2010 mlpp Source: US Census Bureau American Community Survey 2006 -10
Springfield Education Level by Race/Ethnicity, 2006 -2010 mlpp Source: US Census Bureau American Community Survey 2006 -10
 mlpp USDA Economic Research") Springfield – Food Security & the Food Desert Problem (2009) mlpp USDA Economic Research Service Food Access Research Atlas 2010
Springfield – Food Security & the Food Desert Problem (2009) mlpp USDA Economic Research Service Food Access Research Atlas 2010
 Springfield Teen Birth Rates by Demographic ID Mass. Dept. Public Health Birth Dataset 2010
Springfield Teen Birth Rates by Demographic ID Mass. Dept. Public Health Birth Dataset 2010
 Springfield Asthma Hospitalization Rates, Children 0 -14, per 100, 000 Mass Dept. Public Health Hospitalization Dataset 2009 -11
Springfield Asthma Hospitalization Rates, Children 0 -14, per 100, 000 Mass Dept. Public Health Hospitalization Dataset 2009 -11
 Social Disparities & Child Health: The Problem Persists o “Children are the poorest segment of society: 22 percent of U. S. children live below the federal poverty level, a prevalence that has persisted since the 1970 s. The effects of poverty on children’s health and well-being are well-documented. Poor children have increased infant mortality; more frequent and severe chronic diseases such as asthma; poorer nutrition and growth; less access to quality health care; lower immunization rates; and increased obesity and its complications. ” mlpp American Academy Pediatrics: May 24, 2013
Social Disparities & Child Health: The Problem Persists o “Children are the poorest segment of society: 22 percent of U. S. children live below the federal poverty level, a prevalence that has persisted since the 1970 s. The effects of poverty on children’s health and well-being are well-documented. Poor children have increased infant mortality; more frequent and severe chronic diseases such as asthma; poorer nutrition and growth; less access to quality health care; lower immunization rates; and increased obesity and its complications. ” mlpp American Academy Pediatrics: May 24, 2013
 “Preventive Pediatrics” A New Paradigm is Born mlpp
“Preventive Pediatrics” A New Paradigm is Born mlpp
 Preventive Pediatrics o “Double jeopardy” of children in poverty n More frequently exposed to risks to health and development n Suffer more negative consequences from such exposures than their more advantaged peers o Preventive pediatrics model in 1995 was not sufficient mlpp Source: Zuckerman & Parker, 95 Pediatrics 5 (May 1995)
Preventive Pediatrics o “Double jeopardy” of children in poverty n More frequently exposed to risks to health and development n Suffer more negative consequences from such exposures than their more advantaged peers o Preventive pediatrics model in 1995 was not sufficient mlpp Source: Zuckerman & Parker, 95 Pediatrics 5 (May 1995)
 Preventive Pediatrics o Solution: link needed services within the pediatric office n n mlpp Legal advocacy Parenting and child development Two-generation approach Parental mental health Source: Zuckerman & Parker, 95 Pediatrics 5 (May 1995)
Preventive Pediatrics o Solution: link needed services within the pediatric office n n mlpp Legal advocacy Parenting and child development Two-generation approach Parental mental health Source: Zuckerman & Parker, 95 Pediatrics 5 (May 1995)
 Legal Advocacy: Why Doctors Really Do Need Lawyers? mlpp
Legal Advocacy: Why Doctors Really Do Need Lawyers? mlpp
 Medical-Legal Partnerships: From Idea to Practice mlpp
Medical-Legal Partnerships: From Idea to Practice mlpp
 Medical-Legal Partnerships: From Idea to Practice o Founded in 1993 at Boston City Hospital (now Boston Medical Center) as the Family Advocacy Project (FAP) o Idea generated from need… o Lawyer as member of pediatric treatment team mlpp
Medical-Legal Partnerships: From Idea to Practice o Founded in 1993 at Boston City Hospital (now Boston Medical Center) as the Family Advocacy Project (FAP) o Idea generated from need… o Lawyer as member of pediatric treatment team mlpp
 Medical-Legal Partnerships: From Idea to Practice o 1993 – Establishment of Boston FAP o 2000 – Establishment of Hartford Connecticut’s Medical-Legal Partnership Project (MLPP) at Conn. Children’s Medical Center (CCMC) o 2006 – National Center for MLP founded (Boston), now in DC at GW School of Public Health o 2015 n In over 292 hospitals/health centers in 36 states n Providing legal assistance to over 34, 000 individuals and families n Have trained over 15, 000 healthcare providers about the connections between poverty, health, and unmet legal needs mlpp
Medical-Legal Partnerships: From Idea to Practice o 1993 – Establishment of Boston FAP o 2000 – Establishment of Hartford Connecticut’s Medical-Legal Partnership Project (MLPP) at Conn. Children’s Medical Center (CCMC) o 2006 – National Center for MLP founded (Boston), now in DC at GW School of Public Health o 2015 n In over 292 hospitals/health centers in 36 states n Providing legal assistance to over 34, 000 individuals and families n Have trained over 15, 000 healthcare providers about the connections between poverty, health, and unmet legal needs mlpp
 Medical-Legal Partnerships: From Idea to Practice o Contributed to curricula at 51 law schools, 36 medical schools, and 46 residency programs o MLP nationwide pilot included in first Affordable Care Act bill (and independent MLP for Health Act July 2010) o HRSA recognizes civil legal aid as “enabling service” for health centers mlpp
Medical-Legal Partnerships: From Idea to Practice o Contributed to curricula at 51 law schools, 36 medical schools, and 46 residency programs o MLP nationwide pilot included in first Affordable Care Act bill (and independent MLP for Health Act July 2010) o HRSA recognizes civil legal aid as “enabling service” for health centers mlpp
 Medical-Legal Partnerships: National Survey • • • mlpp 152 hospitals 136 health centers 36 health schools 142 legal aid agencies 51 law schools 71 pro bono partners 2015 MLP National Site Survey @ www. medicallegalpartnership. org/mlp-network
Medical-Legal Partnerships: National Survey • • • mlpp 152 hospitals 136 health centers 36 health schools 142 legal aid agencies 51 law schools 71 pro bono partners 2015 MLP National Site Survey @ www. medicallegalpartnership. org/mlp-network
 Attacking Poverty Collaboratively and Collaterally o September 2, 2015 PBS Newshour: Why Doctors are Prescribing Legal Aid for Patients o https: //www. youtu be. com/watch? v=K KVFHwj. Wih 8 mlpp
Attacking Poverty Collaboratively and Collaterally o September 2, 2015 PBS Newshour: Why Doctors are Prescribing Legal Aid for Patients o https: //www. youtu be. com/watch? v=K KVFHwj. Wih 8 mlpp
 Doctors and Lawyers in the Clinical Setting Legal Assistance in the Healthcare Setting Health and Legal Institutions Practice Transformation Policy Change mlpp
Doctors and Lawyers in the Clinical Setting Legal Assistance in the Healthcare Setting Health and Legal Institutions Practice Transformation Policy Change mlpp
 How the Collaboration Works o Clinicians: n n n See the patients Identify the issues Address the needs Call in intervention Collaborate Advocate o Attorneys n n n mlpp On-site availability Provide consultation Provide representation Education Policy initiatives & systemic reform Team partner
How the Collaboration Works o Clinicians: n n n See the patients Identify the issues Address the needs Call in intervention Collaborate Advocate o Attorneys n n n mlpp On-site availability Provide consultation Provide representation Education Policy initiatives & systemic reform Team partner
 mlpp
mlpp
 Connecticut’s Medical-Legal Partnership Project mlpp
Connecticut’s Medical-Legal Partnership Project mlpp
 The Connecticut MLPP: 15 Years of Multidisciplinary Advocacy o Three part strategy: n n n Direct representation Education and Training Systemic Advocacy o Financial Criteria – poverty based program = no fees charged o Direct Institutional contributions and grants provide funding for program o Mission – improve health outcomes mlpp
The Connecticut MLPP: 15 Years of Multidisciplinary Advocacy o Three part strategy: n n n Direct representation Education and Training Systemic Advocacy o Financial Criteria – poverty based program = no fees charged o Direct Institutional contributions and grants provide funding for program o Mission – improve health outcomes mlpp
 The Connecticut MLPP: 15 Years of Multidisciplinary Advocacy o Families Represented = +/- 1, 500 n 2, 500 children o Consultations = > 8, 000 o Trainings = > 1, 000 n Residency curricula n Statewide & National presentations o Systemic Reform – legislative & policy changes mlpp
The Connecticut MLPP: 15 Years of Multidisciplinary Advocacy o Families Represented = +/- 1, 500 n 2, 500 children o Consultations = > 8, 000 o Trainings = > 1, 000 n Residency curricula n Statewide & National presentations o Systemic Reform – legislative & policy changes mlpp
 The Hartford MLPP: What Have We Accomplished in 15 Years? o From one office to five sites o Publication of nationally recognized book on adolescent health & confidentiality o Publication of article on Medical-Legal Partnerships (JLME): n How Bioethics Can Enrich Medical-Legal Collaborations mlpp
The Hartford MLPP: What Have We Accomplished in 15 Years? o From one office to five sites o Publication of nationally recognized book on adolescent health & confidentiality o Publication of article on Medical-Legal Partnerships (JLME): n How Bioethics Can Enrich Medical-Legal Collaborations mlpp
 The Hartford MLPP: What Have We Accomplished in 15 Years? o o o Obtained RWJ grant for IRNAAP Full Institutional funding - YNHH Systemic Accomplishments: n Policy change to provide Medicaid coverage for nutritional supplements n Neuro. Psychological testing to students in HPS (delays up to two years) n Provision of PT, OT & S&L services to children outside the home in daycare or school aftercare programs n Mental Health Screening Compliance mlpp
The Hartford MLPP: What Have We Accomplished in 15 Years? o o o Obtained RWJ grant for IRNAAP Full Institutional funding - YNHH Systemic Accomplishments: n Policy change to provide Medicaid coverage for nutritional supplements n Neuro. Psychological testing to students in HPS (delays up to two years) n Provision of PT, OT & S&L services to children outside the home in daycare or school aftercare programs n Mental Health Screening Compliance mlpp
 MLPP’s “Six Questions” 1. 2. 3. 4. 5. 6. mlpp Do you Have Enough Food? Are your housing conditions safe/Is your housing stable? Do you have enough money in the house to pay for basic necessities (food, clothing, shelter, hygiene items)? Have you had any problems with your HUSKY/medical insurance ( eligibility, denials, rejections, bills, etc) Is your child being properly educated? Are there any mental health concerns that you would like to discuss …
MLPP’s “Six Questions” 1. 2. 3. 4. 5. 6. mlpp Do you Have Enough Food? Are your housing conditions safe/Is your housing stable? Do you have enough money in the house to pay for basic necessities (food, clothing, shelter, hygiene items)? Have you had any problems with your HUSKY/medical insurance ( eligibility, denials, rejections, bills, etc) Is your child being properly educated? Are there any mental health concerns that you would like to discuss …
 Observational Studies: Focusing on Impact o Three types of studies n Financial impact on patients and partners n Patient health and wellbeing n Knowledge and training of health providers mlpp
Observational Studies: Focusing on Impact o Three types of studies n Financial impact on patients and partners n Patient health and wellbeing n Knowledge and training of health providers mlpp
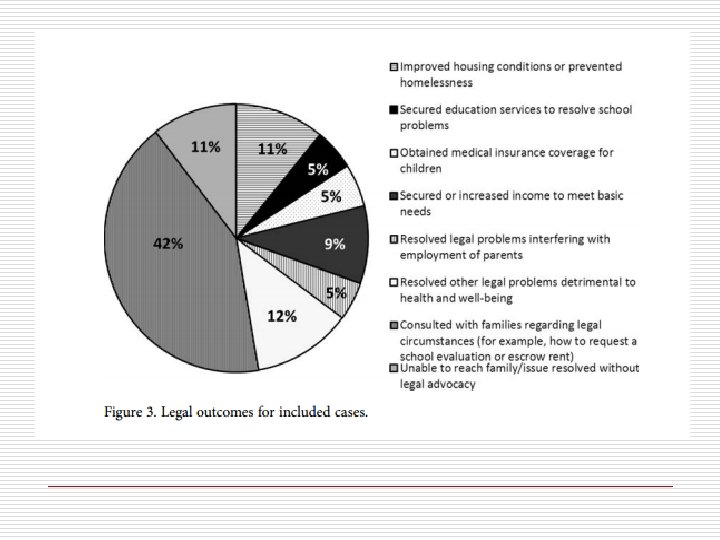
 Cincinnati Children’s Experience – Child He. LP o Doctors and Lawyers Collaborating to He. LP Children – Outcomes from a Successful Partnership Between Professions n Klein et al, Journal of Health Care for the Poor and Underserved 24 (2013): 10631073 mlpp
Cincinnati Children’s Experience – Child He. LP o Doctors and Lawyers Collaborating to He. LP Children – Outcomes from a Successful Partnership Between Professions n Klein et al, Journal of Health Care for the Poor and Underserved 24 (2013): 10631073 mlpp
 mlpp
mlpp
 mlpp
mlpp
 Impact on Patient Health and Wellbeing o Pilot Study of Impact of MLP Services on Patients’ Perceived Stress and Wellbeing n Ryan et. al, Journal of Health Care for the Poor and Underserved 23 (2012): 1536 -1546 mlpp
Impact on Patient Health and Wellbeing o Pilot Study of Impact of MLP Services on Patients’ Perceived Stress and Wellbeing n Ryan et. al, Journal of Health Care for the Poor and Underserved 23 (2012): 1536 -1546 mlpp
 MYCa. W mlpp
MYCa. W mlpp
 mlpp
mlpp
 mlpp
mlpp
 mlpp
mlpp
 Peninsula Family Advocacy Program Lucile Packard Children’s Hospital o Pilot Study of Medical-Legal Partnership to Address Social and Legal Needs of Patients n Weintraub et al. Journal of Health Care for the Poor and Underserved 21 (2010): 157 -168 mlpp
Peninsula Family Advocacy Program Lucile Packard Children’s Hospital o Pilot Study of Medical-Legal Partnership to Address Social and Legal Needs of Patients n Weintraub et al. Journal of Health Care for the Poor and Underserved 21 (2010): 157 -168 mlpp
 mlpp
mlpp
 Results o WCC and imm status: no difference o Statistically significant change in avoidance of health care d/t n Worry about cost of health care n Did not have health insurance o No difference in numbers of acute care visits, ER visits, or missed school days o Participants were very satisfied with services mlpp
Results o WCC and imm status: no difference o Statistically significant change in avoidance of health care d/t n Worry about cost of health care n Did not have health insurance o No difference in numbers of acute care visits, ER visits, or missed school days o Participants were very satisfied with services mlpp
 What about medical outcomes? o Environmental Improvements Brought by the Legal Interventions in the Homes of Poorly Controlled Inner-city Adult Asthmatic Patients: A Proof-of. Concept Study n Sullivan et al. Journal of Asthma, 2012; 49 (9): 911 -917 mlpp
What about medical outcomes? o Environmental Improvements Brought by the Legal Interventions in the Homes of Poorly Controlled Inner-city Adult Asthmatic Patients: A Proof-of. Concept Study n Sullivan et al. Journal of Asthma, 2012; 49 (9): 911 -917 mlpp
 mlpp
mlpp
 Back to the Cases… Case #1: Asthma o Apartment with roaches and mold an unresponsive landlord o PCP obtains consent from parent to refer to MLPP n Provides relevant information to MLPP attorney, perhaps reviewing chart together (e. g. , asthma diagnosis, treatment plan, adherence to regimen, triggers, frequency/timeline of return to care) mlpp
Back to the Cases… Case #1: Asthma o Apartment with roaches and mold an unresponsive landlord o PCP obtains consent from parent to refer to MLPP n Provides relevant information to MLPP attorney, perhaps reviewing chart together (e. g. , asthma diagnosis, treatment plan, adherence to regimen, triggers, frequency/timeline of return to care) mlpp
 Back to the Cases… Case #1: Asthma o MLPP attorney n Meets with family for intake to obtain detailed history n Conducts investigative home visit (including taking pictures) n Meets with housing inspector n Contacts landlord with request to remediate environmental issues n If landlord refuses, reviews options with family, which includes possibility of taking legal action in court mlpp
Back to the Cases… Case #1: Asthma o MLPP attorney n Meets with family for intake to obtain detailed history n Conducts investigative home visit (including taking pictures) n Meets with housing inspector n Contacts landlord with request to remediate environmental issues n If landlord refuses, reviews options with family, which includes possibility of taking legal action in court mlpp
 Back to the Cases… Case #2: Expulsion o In-home tutoring until child is “in control” of behavior o PCP obtains consent from parent to refer to MLPP n Provides relevant information to MLPP attorney, perhaps reviewing chart together (e. g. , disabilities impairing education, academic supports needed and outcomes of interventions attempted [Special Education], history of suspensions/expulsions) mlpp
Back to the Cases… Case #2: Expulsion o In-home tutoring until child is “in control” of behavior o PCP obtains consent from parent to refer to MLPP n Provides relevant information to MLPP attorney, perhaps reviewing chart together (e. g. , disabilities impairing education, academic supports needed and outcomes of interventions attempted [Special Education], history of suspensions/expulsions) mlpp
 Back to the Cases… Case #2: Expulsion o MLPP attorney n Meets with family for intake to obtain detailed history and consent to communicate with school n Collects and reviews educational documents (e. g. , evaluation reports, behavior plan, Individualized Education Plan, attendance) n Interviews school staff n May invoke support of educational consultant n Checks compliance of school provisions for child’s education AND suggests appropriate remedies (may require legal action) mlpp
Back to the Cases… Case #2: Expulsion o MLPP attorney n Meets with family for intake to obtain detailed history and consent to communicate with school n Collects and reviews educational documents (e. g. , evaluation reports, behavior plan, Individualized Education Plan, attendance) n Interviews school staff n May invoke support of educational consultant n Checks compliance of school provisions for child’s education AND suggests appropriate remedies (may require legal action) mlpp
 New Venue – New Partners: New Ideas? o Multidisciplinary team approach to obesity intervention – legal, medical & social work. n Medicaid support n Innovative approach (Endocrine, Primary Care, Behavioral health, MLPP) o Improving primary care access to mental health services – a team approach (Medicaid/Primary Care/MLPP)
New Venue – New Partners: New Ideas? o Multidisciplinary team approach to obesity intervention – legal, medical & social work. n Medicaid support n Innovative approach (Endocrine, Primary Care, Behavioral health, MLPP) o Improving primary care access to mental health services – a team approach (Medicaid/Primary Care/MLPP)
 References o Zuckerman & Parker, Preventive Pediatrics- New Models of Expanded Health Services, 95 Pediatrics 5 (1995) o Zuckerman, Sandel, Smith, Lawton, Why Pediatricians Need Lawyers to Keep Children Healthy, 114 Pediatrics 1 (July 2004) o Parker, Greer, et al, Double Jeopardy: The Impact of Poverty on Early Childhood Development. 35 Pediatric Clin. North Am. (1988) o Askew, Wise, The Neighborhood: Poverty, Affluence, Geographic mobility & Violence in Levine, et al, Developmental-Behavioral Pediatrics (1999). o Wood, Valdez, et al, Health of Homeless and Housed Poor Children. 86 Pediatrics (1990) mlpp
References o Zuckerman & Parker, Preventive Pediatrics- New Models of Expanded Health Services, 95 Pediatrics 5 (1995) o Zuckerman, Sandel, Smith, Lawton, Why Pediatricians Need Lawyers to Keep Children Healthy, 114 Pediatrics 1 (July 2004) o Parker, Greer, et al, Double Jeopardy: The Impact of Poverty on Early Childhood Development. 35 Pediatric Clin. North Am. (1988) o Askew, Wise, The Neighborhood: Poverty, Affluence, Geographic mobility & Violence in Levine, et al, Developmental-Behavioral Pediatrics (1999). o Wood, Valdez, et al, Health of Homeless and Housed Poor Children. 86 Pediatrics (1990) mlpp
") References o M. Tebo, Just What the Doctor Ordered. American Bar Association Journal (2001) o Ellwood, Ku, Welfare and Immigration Reforms: Unintended Side Effects for Medicaid. 17 Health Affairs (1988) o Marmot, Acting on Evidence to Reduce Inequalities in Health. 18 Health Affairs 3 (1999) o Amy T. Campbell, Jay Sicklick, Paula Galowitz, Randye Retkin & Stewart B. Fleishman (2010). How Bioethics Can Enrich Medical-Legal Collaborations. Journal of Law, Medicine and Ethics 38 (4): 847 -862. mlpp
References o M. Tebo, Just What the Doctor Ordered. American Bar Association Journal (2001) o Ellwood, Ku, Welfare and Immigration Reforms: Unintended Side Effects for Medicaid. 17 Health Affairs (1988) o Marmot, Acting on Evidence to Reduce Inequalities in Health. 18 Health Affairs 3 (1999) o Amy T. Campbell, Jay Sicklick, Paula Galowitz, Randye Retkin & Stewart B. Fleishman (2010). How Bioethics Can Enrich Medical-Legal Collaborations. Journal of Law, Medicine and Ethics 38 (4): 847 -862. mlpp
 570 -5327, jsicklick@kidscounsel. org n") Resources o Connecticut MLPP: n Attorney Jay Sicklick (860) 570 -5327, jsicklick@kidscounsel. org n Attorney Bonnie Roswig (CCMC) (860) 5458581, bonnie. roswig@connecticutchildrens. org n Attorney Alice Rosenthal (YNHH) (203), Alice. Rosenthal@YNHH. org n Center for Children’s Advocacy, www. kidscounsel. org (860) 570 -5327
Resources o Connecticut MLPP: n Attorney Jay Sicklick (860) 570 -5327, jsicklick@kidscounsel. org n Attorney Bonnie Roswig (CCMC) (860) 5458581, bonnie. roswig@connecticutchildrens. org n Attorney Alice Rosenthal (YNHH) (203), Alice. Rosenthal@YNHH. org n Center for Children’s Advocacy, www. kidscounsel. org (860) 570 -5327