

d67ec6bbea69bb7051c89da30ee1a614.ppt
- Количество слайдов: 88
 Maternal Risk Factors Fetal Assessment
Maternal Risk Factors Fetal Assessment
 High Risk Pregnancy n The life or health of the mother or fetus is jeopardized n Examples include: – GDM – Previous loss – AMA – HTN – Abnormalities with the neonate
High Risk Pregnancy n The life or health of the mother or fetus is jeopardized n Examples include: – GDM – Previous loss – AMA – HTN – Abnormalities with the neonate
 Perinatal Mortality n Overall maternal deaths are small n Many deaths a preventable n Education and prenatal care very important
Perinatal Mortality n Overall maternal deaths are small n Many deaths a preventable n Education and prenatal care very important
 Antepartum Testing FKCs BID n UTZ n – – – – – FHR Gestation age Abnormalities IUGR Placental location and quality AFI Position BPP Doppler flow Fetal growth
Antepartum Testing FKCs BID n UTZ n – – – – – FHR Gestation age Abnormalities IUGR Placental location and quality AFI Position BPP Doppler flow Fetal growth
 Ultrasound n Can be done abdominally or transvaginally n 1 st trimester done to detect viability, calculate EDC n 2 nd trimester done to detect anomalies, calculate EDC n 3 rd trimester done to do BPP, fetal growth and well-being, AFI
Ultrasound n Can be done abdominally or transvaginally n 1 st trimester done to detect viability, calculate EDC n 2 nd trimester done to detect anomalies, calculate EDC n 3 rd trimester done to do BPP, fetal growth and well-being, AFI
 Doppler Flow Analysis via UTZ n Study blood blow in the fetus and placenta n Done on high risk mothers: – IUGR – HTN – DM – Multiple gestation
Doppler Flow Analysis via UTZ n Study blood blow in the fetus and placenta n Done on high risk mothers: – IUGR – HTN – DM – Multiple gestation
 AFI n Polyhydramnios – too much amniotic fluid n Oligohydramnios – too little amniotic fluid
AFI n Polyhydramnios – too much amniotic fluid n Oligohydramnios – too little amniotic fluid
 Biophysical Profile n Includes 5 components: – Fetal breathing movements – Gross body movements – Fetal tone – AFI – NST - reactive
Biophysical Profile n Includes 5 components: – Fetal breathing movements – Gross body movements – Fetal tone – AFI – NST - reactive
 Amniocentesis n Used with direct ultrasound n Less than 1% result in complications – Complications include: § Fetal death, miscarriage § Maternal hemorrhage § Infection to fetus § Preterm labor § Leakage of amniotic fluid
Amniocentesis n Used with direct ultrasound n Less than 1% result in complications – Complications include: § Fetal death, miscarriage § Maternal hemorrhage § Infection to fetus § Preterm labor § Leakage of amniotic fluid
 Meconium n Visual inspection of amniotic fluid n Meconium is defined as thin and thick and particulate n Associated with fetal stress: hypoxia, umbilical cord compression
Meconium n Visual inspection of amniotic fluid n Meconium is defined as thin and thick and particulate n Associated with fetal stress: hypoxia, umbilical cord compression
 CVS n Done between 9 -12 weeks n Genetic studies n Removal of small amount of tissue from the fetal portion of the placenta n Complications: vaginal spotting, miscarriage, ROM, chorioamnionitis n If done prior to 10 weeks, increased risk of limb anomalies
CVS n Done between 9 -12 weeks n Genetic studies n Removal of small amount of tissue from the fetal portion of the placenta n Complications: vaginal spotting, miscarriage, ROM, chorioamnionitis n If done prior to 10 weeks, increased risk of limb anomalies
 AFP n Genetic test n Done with mothers blood n 16 -20 weeks gestation n Mandated by state of California
AFP n Genetic test n Done with mothers blood n 16 -20 weeks gestation n Mandated by state of California
 EFM n Third trimester goal is to continue to observe the fetus within the intrauterine environment n Goal: dx uteroplacental insufficiency n NST vs. CST
EFM n Third trimester goal is to continue to observe the fetus within the intrauterine environment n Goal: dx uteroplacental insufficiency n NST vs. CST
 NST n 90% of gross fetal body movements are associated with accelerations of the FHR n Can be performed outpatient n Not as sensitive n User friendly but must interpret strip n Fetus may be in a sleep state or affected by maternal medications, glucose etc.
NST n 90% of gross fetal body movements are associated with accelerations of the FHR n Can be performed outpatient n Not as sensitive n User friendly but must interpret strip n Fetus may be in a sleep state or affected by maternal medications, glucose etc.
 NST n To be reactive must meet criteria n Must be at least 20 minutes in length n Must have 2 or more accelerations that meet the ’ 15 X 15’ criteria n Must have a normal baseline n Must have LTV
NST n To be reactive must meet criteria n Must be at least 20 minutes in length n Must have 2 or more accelerations that meet the ’ 15 X 15’ criteria n Must have a normal baseline n Must have LTV
 NST n To stimulate a fetus that is not meeting criteria: – Change positions of the mother – LS, RS – Increase fluids – Acoustic stimulator
NST n To stimulate a fetus that is not meeting criteria: – Change positions of the mother – LS, RS – Increase fluids – Acoustic stimulator
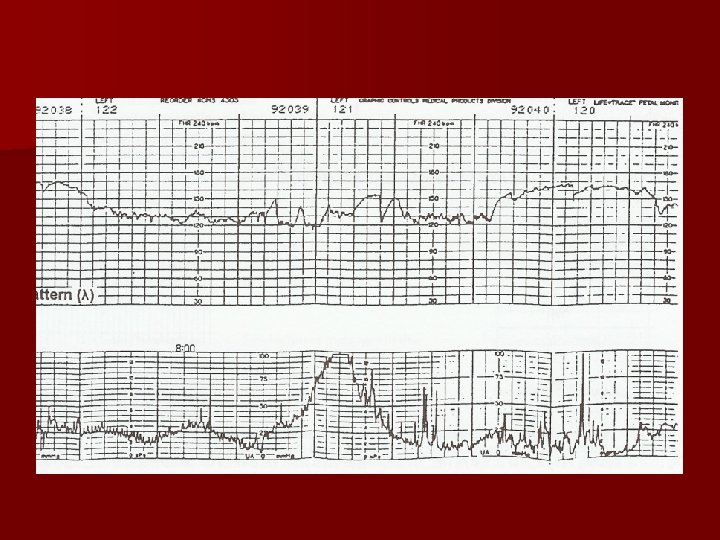
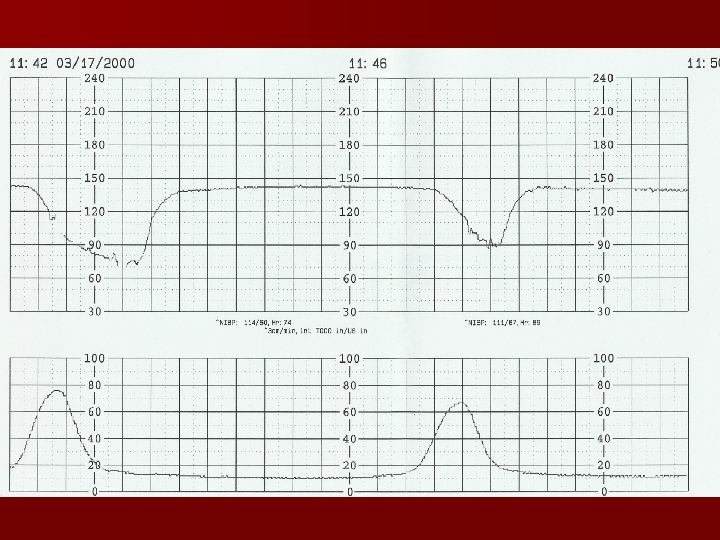
 CST n Done in the inpatient setting only! n Has contraindications n May be expensive if meds/IV needed n Monitored for 10 minutes first n Then may use nipple stimulation or oxytocin stimulation n No late decelerations than negative CST
CST n Done in the inpatient setting only! n Has contraindications n May be expensive if meds/IV needed n Monitored for 10 minutes first n Then may use nipple stimulation or oxytocin stimulation n No late decelerations than negative CST
 CST
CST
 Endocrine and Metabolic Disorders n #1 Diabetes Mellitus n Disorders of the thyroid n Hyperemesis
Endocrine and Metabolic Disorders n #1 Diabetes Mellitus n Disorders of the thyroid n Hyperemesis
 Diabetes n Hyperglycemia n May be due to inadequate insulin action or due to impaired insulin secretion n Type 1 – insulin deficiency n Type 2 – insulin resistance n GDM – glucose intolerance during pregnancy
Diabetes n Hyperglycemia n May be due to inadequate insulin action or due to impaired insulin secretion n Type 1 – insulin deficiency n Type 2 – insulin resistance n GDM – glucose intolerance during pregnancy
 DM n 10 th week fetus produces it own insulin n Insulin does not cross the placental barrier n Glucose levels in the fetus and directly proportional to the mother n 2 nd and 3 rd trimesters – decreased tolerance to glucose, increased insulin resistance, increased hepatic function of glucose
DM n 10 th week fetus produces it own insulin n Insulin does not cross the placental barrier n Glucose levels in the fetus and directly proportional to the mother n 2 nd and 3 rd trimesters – decreased tolerance to glucose, increased insulin resistance, increased hepatic function of glucose
 Diabetic Nephropathy n Increased risks for: – Preeclampsia – IUGR – PTL – Fetal distress – IUFD – Neonatal death
Diabetic Nephropathy n Increased risks for: – Preeclampsia – IUGR – PTL – Fetal distress – IUFD – Neonatal death
 DM n Poor glycemic control is associated with increased risks of miscarriage at time of conception n Poor glycemic control in later part of pregnancy is assoc. with fetal macrosomia and polyhydramnios
DM n Poor glycemic control is associated with increased risks of miscarriage at time of conception n Poor glycemic control in later part of pregnancy is assoc. with fetal macrosomia and polyhydramnios
 Polyhydramnios n May compress on the vena cava and aorta causing hypotension, PROM, PP hemorrhage, maternal dyspnea
Polyhydramnios n May compress on the vena cava and aorta causing hypotension, PROM, PP hemorrhage, maternal dyspnea
 Macrosomia n Disproportionate increase in shoulder and trunk size n 4000 -4500 gms or greater n Fetus will have excess stores of glycogen n Increased risks of – Shoulder dystocia – C/S – Assisted deliveries
Macrosomia n Disproportionate increase in shoulder and trunk size n 4000 -4500 gms or greater n Fetus will have excess stores of glycogen n Increased risks of – Shoulder dystocia – C/S – Assisted deliveries
 IUGR n Compromised uteroplacental insufficiency n 02 available to the fetus is decreased
IUGR n Compromised uteroplacental insufficiency n 02 available to the fetus is decreased
 RDS n Increased RDS due to high glucose levels n Delays pulmonary maturity
RDS n Increased RDS due to high glucose levels n Delays pulmonary maturity
 Neonatal Hypoglycemia n Usually 30 -60 minutes after birth n Due to high glucose levels during pregnancy and rapid use of glucose after birth n Related to mothers level of glucose control
Neonatal Hypoglycemia n Usually 30 -60 minutes after birth n Due to high glucose levels during pregnancy and rapid use of glucose after birth n Related to mothers level of glucose control
 Labs with DM n HBA 1 c n 1 hour PP n FBS
Labs with DM n HBA 1 c n 1 hour PP n FBS
 Diet n Sweet success diet n Well balanced diet n 6 small meals / day n Have snack at HS n Never skip meals n Avoid simple sugars
Diet n Sweet success diet n Well balanced diet n 6 small meals / day n Have snack at HS n Never skip meals n Avoid simple sugars
 Insulin n Regular/Lispro and NPH n 2/3 dose in am and 1/3 dose in pm
Insulin n Regular/Lispro and NPH n 2/3 dose in am and 1/3 dose in pm
 Monitoring Glucose Levels n FBS n 1 hour PP n HS n 5 checks / day
Monitoring Glucose Levels n FBS n 1 hour PP n HS n 5 checks / day
 Fetal Surveillance n NSTs n At done around 26 weeks, weekly 32 weeks done biweekly with NST/BPP
Fetal Surveillance n NSTs n At done around 26 weeks, weekly 32 weeks done biweekly with NST/BPP
 Infections and DM n Infections are increased: – Candidiasis – UTIs – PP infections
Infections and DM n Infections are increased: – Candidiasis – UTIs – PP infections
 DM n Increased risk of IUFD after 36 weeks n Increased congenital anomalies – Cardiac defects – CNS defects § Spina bifida § anencephaly – Skeletal defects
DM n Increased risk of IUFD after 36 weeks n Increased congenital anomalies – Cardiac defects – CNS defects § Spina bifida § anencephaly – Skeletal defects
 DM and labor n Continuous fetal monitoring n Blood glucose levels in tight control n Be prepared for CPD
DM and labor n Continuous fetal monitoring n Blood glucose levels in tight control n Be prepared for CPD
 GDM n Women with GDM at risk of developing DM later on in life n NSTs around 28 weeks
GDM n Women with GDM at risk of developing DM later on in life n NSTs around 28 weeks
 Hyperthyroidism n Typically caused by Grave’s disease n S/S: – Fatigue – Heat intolerance – Warm skin – Diaphoresis – Weight loss
Hyperthyroidism n Typically caused by Grave’s disease n S/S: – Fatigue – Heat intolerance – Warm skin – Diaphoresis – Weight loss
 n Should be treated in pregnancy n Tx with PTU n Beta blockers n May lead to thyroid storm if untreated
n Should be treated in pregnancy n Tx with PTU n Beta blockers n May lead to thyroid storm if untreated
 Hypothyroidism n Usually caused by Hashimoto’s n S/S: – Weight gain – Cold intolerance – Fatigue – Hair loss – Constipation – Dry skin
Hypothyroidism n Usually caused by Hashimoto’s n S/S: – Weight gain – Cold intolerance – Fatigue – Hair loss – Constipation – Dry skin
 n Tx with thyroid hormones such as synthroid or levothyroxine n Maintain TSH wnl n Checked periodically throughout the pregnancy
n Tx with thyroid hormones such as synthroid or levothyroxine n Maintain TSH wnl n Checked periodically throughout the pregnancy
 Cardiovascular Disorders n The heart must compensate for the increased workload n If the cardiac changes are not well tolerated than cardiac failure can develop n 1% of pregnancies are complicated by heart disease
Cardiovascular Disorders n The heart must compensate for the increased workload n If the cardiac changes are not well tolerated than cardiac failure can develop n 1% of pregnancies are complicated by heart disease
 NY Heart Association Classes n Class III n Class IV
NY Heart Association Classes n Class III n Class IV
 n Cardiac output is increased n Peak of the increase 20 -24 weeks gestation n Cardiac problems should be managed with cardiologist n Mortality with pulmonary hypertension and pregnancy is more than 50% n Diet: low sodium
n Cardiac output is increased n Peak of the increase 20 -24 weeks gestation n Cardiac problems should be managed with cardiologist n Mortality with pulmonary hypertension and pregnancy is more than 50% n Diet: low sodium
 Nursing Care n Avoiding anemia n Avoid strenuous activity n Monitor for: cardiac failure and pulmonary congestion
Nursing Care n Avoiding anemia n Avoid strenuous activity n Monitor for: cardiac failure and pulmonary congestion
 During Labor n Side lying position n Prophylactic antibiotic n Epidural n Attempt vaginal delivery n If anticoagulant therapy is needed: – Heparin – Lovenox
During Labor n Side lying position n Prophylactic antibiotic n Epidural n Attempt vaginal delivery n If anticoagulant therapy is needed: – Heparin – Lovenox
 MVP n Common and usually benign n May experience syncope, palpitations and dyspnea n Prophylactic antibiotics given before invasive procedure or birth
MVP n Common and usually benign n May experience syncope, palpitations and dyspnea n Prophylactic antibiotics given before invasive procedure or birth
 n") Anemia n Most common iron deficiency n Hgb falls below 12 (most labs) n Typically seen in the end of 2 nd trimester n Iron supplementation
Anemia n Most common iron deficiency n Hgb falls below 12 (most labs) n Typically seen in the end of 2 nd trimester n Iron supplementation
 Folic Acid Deficiency Anemia n Increases risk of NTD, cleft lip n Recommended dose 400 mcg/day n Supplemented in cereal and many other foods
Folic Acid Deficiency Anemia n Increases risk of NTD, cleft lip n Recommended dose 400 mcg/day n Supplemented in cereal and many other foods
 Sickle Cell Anemia n Abnormal hemoglobin SS types in the blood n People have recurrent attacks of fever and pain in the abdomen and extremities n Caused from tissue hypoxia, edema n African-Americans
Sickle Cell Anemia n Abnormal hemoglobin SS types in the blood n People have recurrent attacks of fever and pain in the abdomen and extremities n Caused from tissue hypoxia, edema n African-Americans
 Sickle Cell Trait n Typically asymptomatic n Sickling of the RBCs but with a normal RBC life span
Sickle Cell Trait n Typically asymptomatic n Sickling of the RBCs but with a normal RBC life span
 Thalassemia n Common anemia n Insufficient amount of Hgb is produced to fill the RBCs n Mediterranean region n Genetic disorder n May be associated with LBW babies and increased fetal death
Thalassemia n Common anemia n Insufficient amount of Hgb is produced to fill the RBCs n Mediterranean region n Genetic disorder n May be associated with LBW babies and increased fetal death
 Asthma n Common with FH n 1 -4% of pregnant women have Asthma n Possible adverse events associated with asthma: – LBW – Perinatal mortality – Preeclampsia – Complicated labor – Hyperemesis
Asthma n Common with FH n 1 -4% of pregnant women have Asthma n Possible adverse events associated with asthma: – LBW – Perinatal mortality – Preeclampsia – Complicated labor – Hyperemesis
 Asthma Continued n Goal is to relieve the attack, prevent the asthma attack, and maintain 02 n Should be managed with OB and ENT n May require tx: albuterol, steroids, O 2
Asthma Continued n Goal is to relieve the attack, prevent the asthma attack, and maintain 02 n Should be managed with OB and ENT n May require tx: albuterol, steroids, O 2
 Epilepsy n Seizure disorder n May result from developmental abnormalities or injury n 20% have an increase in seizure activity during pregnancy n Risks: more seizures, risk of vaginal bleeding, abruptio placentae, fetus may experience seizures
Epilepsy n Seizure disorder n May result from developmental abnormalities or injury n 20% have an increase in seizure activity during pregnancy n Risks: more seizures, risk of vaginal bleeding, abruptio placentae, fetus may experience seizures
 Epilepsy Continued n Use of antiepeleptic meds during pregnancy has been linked to risks for the fetus n Smallest therapeutic dose to be given n Daily folic acid supplementation n Managed with OB and neurologist
Epilepsy Continued n Use of antiepeleptic meds during pregnancy has been linked to risks for the fetus n Smallest therapeutic dose to be given n Daily folic acid supplementation n Managed with OB and neurologist
 RA n Chronic arthritis n Pain upon movement and swelling in joint spaces n More often in women n 2/3 of women with RA find the severity of symptoms decrease during pregnancy n Typically give baby ASA
RA n Chronic arthritis n Pain upon movement and swelling in joint spaces n More often in women n 2/3 of women with RA find the severity of symptoms decrease during pregnancy n Typically give baby ASA
 SLE n Inflammatory disease, autoimmune antibody production n Advised to wait until in remission for 6 months to become pregnant n 15 -60% of women will develop exacerbation of SLE during pregnancy or postpartum n Tx: ASA and steroids
SLE n Inflammatory disease, autoimmune antibody production n Advised to wait until in remission for 6 months to become pregnant n 15 -60% of women will develop exacerbation of SLE during pregnancy or postpartum n Tx: ASA and steroids
 Cholelithiasis n More often in women n Pregnancy makes women more vulnerable n Surgery often delayed until after delivery
Cholelithiasis n More often in women n Pregnancy makes women more vulnerable n Surgery often delayed until after delivery
 Appendicitis n Dx may take more time to find n Sxs: abdominal pain, nausea, vomiting, loss of appetite n Increases incidence of PTL or SAB
Appendicitis n Dx may take more time to find n Sxs: abdominal pain, nausea, vomiting, loss of appetite n Increases incidence of PTL or SAB
 Maternal Infections
Maternal Infections
 TORCH n Toxoplasmosis – protozoan infection, neonatal effects – jaundice, hydrocephalus, microcephaly n Other- Heb A or B, Group B, Varicella, HIV n Rubella (German measles) – if contracted in 1 st Trimester fetus may have congenital deformities
TORCH n Toxoplasmosis – protozoan infection, neonatal effects – jaundice, hydrocephalus, microcephaly n Other- Heb A or B, Group B, Varicella, HIV n Rubella (German measles) – if contracted in 1 st Trimester fetus may have congenital deformities
 TORCH n CMV- transmitted person to person, may cause CNS damage to fetus n Herpes Simplex (HSV 2) – if initial infection occurs in pregnancy, higher incidence of perinatal loss. Fetus may pick up virus if present in the vagina during labor
TORCH n CMV- transmitted person to person, may cause CNS damage to fetus n Herpes Simplex (HSV 2) – if initial infection occurs in pregnancy, higher incidence of perinatal loss. Fetus may pick up virus if present in the vagina during labor
 Mental Health Disorders
Mental Health Disorders
 Anxiety Disorders n Most common mental disorders n Include: phobias, panic disorders, OCD, PTSD n Tx: relaxation techniques, breathing exercises, imagery
Anxiety Disorders n Most common mental disorders n Include: phobias, panic disorders, OCD, PTSD n Tx: relaxation techniques, breathing exercises, imagery
 Depression in Pregnancy n 6% of women develop depression for the 1 st time during pregnancy n Tx: counseling and tx with SSRIs n Wellbutrin only med named as Category B n Many women opt to DC meds during pregnancy
Depression in Pregnancy n 6% of women develop depression for the 1 st time during pregnancy n Tx: counseling and tx with SSRIs n Wellbutrin only med named as Category B n Many women opt to DC meds during pregnancy
 Substance Abuse in Pregnancy
Substance Abuse in Pregnancy
 Substance Abuse n Damaging effects well documented in research to fetus n Any use of ETOH or illicit drugs during pregnancy is considered abuse n 31% of women had used one or more substances during pregnancy (as compared to 62% during prepregnancy)
Substance Abuse n Damaging effects well documented in research to fetus n Any use of ETOH or illicit drugs during pregnancy is considered abuse n 31% of women had used one or more substances during pregnancy (as compared to 62% during prepregnancy)
 Smoking n Risks of any amount of smoking include: – SAB – SGA – Bleeding – IUFD – Prematurity – SIDS
Smoking n Risks of any amount of smoking include: – SAB – SGA – Bleeding – IUFD – Prematurity – SIDS
 Alcohol n Many women reluctant to tell health care provider n Risks: – LBW – Mental retardation – Learning and physical deficits – With FAS – severe facial deformities
Alcohol n Many women reluctant to tell health care provider n Risks: – LBW – Mental retardation – Learning and physical deficits – With FAS – severe facial deformities
 Alcohol during Pregnancy n Risks to mother: – HTN – Anemia – Nutritional deficits – Pancreatitis – Cirrhosis – Alcoholic hepatitis
Alcohol during Pregnancy n Risks to mother: – HTN – Anemia – Nutritional deficits – Pancreatitis – Cirrhosis – Alcoholic hepatitis
 Marijuana n Crosses the placenta and causes increased carbon monoxide levels in mother’s blood n May cause fetal abnormalities
Marijuana n Crosses the placenta and causes increased carbon monoxide levels in mother’s blood n May cause fetal abnormalities
 Cocaine n In the US, 10 -15% of all pregnant women use cocaine n Problems associated with use: polydrug use, poor health, poor nutrition, STIs, infections, HIV n Poverty big issue
Cocaine n In the US, 10 -15% of all pregnant women use cocaine n Problems associated with use: polydrug use, poor health, poor nutrition, STIs, infections, HIV n Poverty big issue
 Cocaine in Pregnancy n Maternal effects: – – – – – Cardiovascular stress Tachycardia HTN Dysrhythmias MI Liver damage Sz Pulmonary disease Death n Fetal Complications: – – Abruptio placentae PTL Precipitous labor Risks for abdominal pregnancy – Fetal complications after delivery
Cocaine in Pregnancy n Maternal effects: – – – – – Cardiovascular stress Tachycardia HTN Dysrhythmias MI Liver damage Sz Pulmonary disease Death n Fetal Complications: – – Abruptio placentae PTL Precipitous labor Risks for abdominal pregnancy – Fetal complications after delivery
 Opiates in Pregnancy n Drugs include: heroin, Demerol, morphine, codeine, methadone n Methadone is used to treat addiction to other opiates n Possible effects on pregnancy and heroin use are: Preeclampsia, PROM, infections, PTL n Tx: Methadone and psychotherapy n Goal: prevent withdrawal symptoms
Opiates in Pregnancy n Drugs include: heroin, Demerol, morphine, codeine, methadone n Methadone is used to treat addiction to other opiates n Possible effects on pregnancy and heroin use are: Preeclampsia, PROM, infections, PTL n Tx: Methadone and psychotherapy n Goal: prevent withdrawal symptoms
 Methamphetamine n CNS stimulant n Most common use n the 18 -30 yr old range n Neonatal complications include: – IUGR – PRL/PTB
Methamphetamine n CNS stimulant n Most common use n the 18 -30 yr old range n Neonatal complications include: – IUGR – PRL/PTB
 Postpartum Psychologic Complications
Postpartum Psychologic Complications
 Baby Blues n Usually within 4 weeks of childbirth n Many experience this
Baby Blues n Usually within 4 weeks of childbirth n Many experience this
 PPD n Intense sadness, crying all the time, mood swings, fears, anger, anxiety, irritability n Incidence of PPD at 8 weeks – 12% and 8% at 12 weeks n Many women feel guilty n May need tx but usually resolves on own
PPD n Intense sadness, crying all the time, mood swings, fears, anger, anxiety, irritability n Incidence of PPD at 8 weeks – 12% and 8% at 12 weeks n Many women feel guilty n May need tx but usually resolves on own
 Postpartum Psychosis n Delusions, hurting self or the infant, emotional lability, insomnia, suspiciousness, confusion, obsessive concerns regarding the baby n 1 -2/1000 births n 35 -60% recurrence with each subsequent birth n Usually symptoms appear within 8 weeks of birth
Postpartum Psychosis n Delusions, hurting self or the infant, emotional lability, insomnia, suspiciousness, confusion, obsessive concerns regarding the baby n 1 -2/1000 births n 35 -60% recurrence with each subsequent birth n Usually symptoms appear within 8 weeks of birth
 Medical Management n Supportive family n Intense psychotherapy n Emergency n Tx: SSRIs n SSRIs contraindicated while breastfeeding
Medical Management n Supportive family n Intense psychotherapy n Emergency n Tx: SSRIs n SSRIs contraindicated while breastfeeding
 n 1. A client asks the nurse to again explain the purpose of the amniocentesis test. The nurse responds that one purpose of this test is to indicate the: – A. – B. – C. – D. – E. Accurate age of the fetus Presence of certain congenital anomalies Biparietal diameter of the skull Hormone content of the amniotic fluid Mainly the presence of Down’s syndrome
n 1. A client asks the nurse to again explain the purpose of the amniocentesis test. The nurse responds that one purpose of this test is to indicate the: – A. – B. – C. – D. – E. Accurate age of the fetus Presence of certain congenital anomalies Biparietal diameter of the skull Hormone content of the amniotic fluid Mainly the presence of Down’s syndrome
 n 2. The nurse explains to a new mother that the condition of SGA is caused by: – A. – B. – C. – D. Placental insufficiency Maternal obesity Primipara Genetic predisposition
n 2. The nurse explains to a new mother that the condition of SGA is caused by: – A. – B. – C. – D. Placental insufficiency Maternal obesity Primipara Genetic predisposition
 n 3. A pregnant client with diabetes is controlled by insulin. When she asks the nurse what will happen to her insulin requirements during pregnancy, the correct response is: – A. “Because your case is so mild, you are likely not to need much insulin during your pregnancy” – B. “It’s likely that as the pregnancy progresses you will need increased insulin” – C. “Every case is individual so there is really no way to know” – D. “If you follow the diet closely and don’t gain too much weight, your insulin needs should stay the same”
n 3. A pregnant client with diabetes is controlled by insulin. When she asks the nurse what will happen to her insulin requirements during pregnancy, the correct response is: – A. “Because your case is so mild, you are likely not to need much insulin during your pregnancy” – B. “It’s likely that as the pregnancy progresses you will need increased insulin” – C. “Every case is individual so there is really no way to know” – D. “If you follow the diet closely and don’t gain too much weight, your insulin needs should stay the same”
 n 4. The nurse in the newborn nursery understands that assessing a newborn with a diabetic mother, initially the insulin level would be: – A. – B. – C. – D. Higher than in normal infants Lower than in normal infants The same as in normal infants Varied from baby to baby
n 4. The nurse in the newborn nursery understands that assessing a newborn with a diabetic mother, initially the insulin level would be: – A. – B. – C. – D. Higher than in normal infants Lower than in normal infants The same as in normal infants Varied from baby to baby
 n 5. A client is admitted to L&D, at 38 weeks gestation. She is there for evaluation because she is experiencing polyhydramnios. The nurse understands that this diagnosis means that: – A. There is the normal amount of amniotic fluid, thinner in volume – B. A less-than-normal amount of amniotic fluid is present – C. An excessive amount of amniotic fluid is present – D. A leak is causing the fluid to accumulate outside the amniotic sac
n 5. A client is admitted to L&D, at 38 weeks gestation. She is there for evaluation because she is experiencing polyhydramnios. The nurse understands that this diagnosis means that: – A. There is the normal amount of amniotic fluid, thinner in volume – B. A less-than-normal amount of amniotic fluid is present – C. An excessive amount of amniotic fluid is present – D. A leak is causing the fluid to accumulate outside the amniotic sac