

8988a565ca716d69305d7687a63debdd.ppt
- Количество слайдов: 47
 Management of Patients With Epilepsy
Management of Patients With Epilepsy
 Definition n Seizure n n Single provoked/unprovoked episode Epilepsy n Two or more unprovoked seizures
Definition n Seizure n n Single provoked/unprovoked episode Epilepsy n Two or more unprovoked seizures
 Numbers…. Numbers n Unprovoked seizure: n n Risk in US ~ 1/100 Epilepsy/Recurrent unprovoked seizures n n n 8 th leading cause of morbidity 50 million people worldwide, 2 million in US Age-adjusted prevalence 2. 7 -40/1000 Incidence and prevalence is much higher in under developed nations >50% of seizures are untreated Annual cost is $12. 5 billion
Numbers…. Numbers n Unprovoked seizure: n n Risk in US ~ 1/100 Epilepsy/Recurrent unprovoked seizures n n n 8 th leading cause of morbidity 50 million people worldwide, 2 million in US Age-adjusted prevalence 2. 7 -40/1000 Incidence and prevalence is much higher in under developed nations >50% of seizures are untreated Annual cost is $12. 5 billion
 Age Adjusted Incidence
Age Adjusted Incidence
 in 1981 § Based on Semiology/Ictal") Seizure Classification § International League Against Epilepsy (ILAE) in 1981 § Based on Semiology/Ictal behavior and EEG n Partial Seizures n Generalized Seizures n Simple Partial n GTC n Complex Partial n Absence n Secondarily GTC n Myoclonic n Clonic n Tonic n Atonic § Epilepsy Syndrome based classification
Seizure Classification § International League Against Epilepsy (ILAE) in 1981 § Based on Semiology/Ictal behavior and EEG n Partial Seizures n Generalized Seizures n Simple Partial n GTC n Complex Partial n Absence n Secondarily GTC n Myoclonic n Clonic n Tonic n Atonic § Epilepsy Syndrome based classification
 Complex Partial Seizure n n n Impaired consciousness Clinical manifestations vary with site of origin and degree of spread n Presence and nature of aura n Automatisms n Other motor activity Duration (15 sec. — 3 min. )
Complex Partial Seizure n n n Impaired consciousness Clinical manifestations vary with site of origin and degree of spread n Presence and nature of aura n Automatisms n Other motor activity Duration (15 sec. — 3 min. )
") Generalized Tonic Clonic Seizure n n Variable symmetry, intensity, and duration of tonic (stiffening) and clonic (jerking) phases Usual duration 30 -120 sec. Postictal confusion, somnolence, with or without transient focal deficit May be primary or secondarily generalized
Generalized Tonic Clonic Seizure n n Variable symmetry, intensity, and duration of tonic (stiffening) and clonic (jerking) phases Usual duration 30 -120 sec. Postictal confusion, somnolence, with or without transient focal deficit May be primary or secondarily generalized
 Proportion of Cases By Seizure Type Rochester, MN 1935 -1984
Proportion of Cases By Seizure Type Rochester, MN 1935 -1984
 Proportion of Cases By Etiology Rochester, MN 1935 -1984
Proportion of Cases By Etiology Rochester, MN 1935 -1984
 Consequences of Epilepsy n Morbidity n n Mortality n n n Accidents, Injuries Sudden unexpected death in epilepsy Status epilepticus, Suicide, Accidents, Cancer, Infections etc. Socioeconomic Outcome n n n School performance n 56% finish high school and 15% finish college Intellectual functioning (seizures vs. drugs) Social adjustment Employment Driving
Consequences of Epilepsy n Morbidity n n Mortality n n n Accidents, Injuries Sudden unexpected death in epilepsy Status epilepticus, Suicide, Accidents, Cancer, Infections etc. Socioeconomic Outcome n n n School performance n 56% finish high school and 15% finish college Intellectual functioning (seizures vs. drugs) Social adjustment Employment Driving
 Management n Important to establish diagnosis and etiology n n n Classify seizure type and syndrome Good history (from patient and spouse/friend) Labs EEG (sleep deprived vs. routine) Imaging (MRI is far superior to CT) n SPECT, PET
Management n Important to establish diagnosis and etiology n n n Classify seizure type and syndrome Good history (from patient and spouse/friend) Labs EEG (sleep deprived vs. routine) Imaging (MRI is far superior to CT) n SPECT, PET
 Everything that shakes is not a seizure!!! n n n Non-epileptic spells can be extremely hard to differentiate from seizures 30% of all patients Risk factors: n n n Epilepsy Family member with epilepsy Psychiatric problems Most have conversion disorder Need video EEG monitoring to confirm diagnosis
Everything that shakes is not a seizure!!! n n n Non-epileptic spells can be extremely hard to differentiate from seizures 30% of all patients Risk factors: n n n Epilepsy Family member with epilepsy Psychiatric problems Most have conversion disorder Need video EEG monitoring to confirm diagnosis
 Medical Management n n n Mid 1800’s: Bromides 1912: Phenobarbital 1938: Merritt and Putnam - Phenytoin
Medical Management n n n Mid 1800’s: Bromides 1912: Phenobarbital 1938: Merritt and Putnam - Phenytoin
 Year Introduced Phenobarbital 1912 Phenytoin 1938 Primidone 1954 Ethosuximide 1960 Carbamazepine 1974 Valproate 1978 Felbamate 1993 Gabapentin 1993 Lamotrigine 1994 Topiramate 1996 Tiagibine 1997 Levetiracetam 2000 Oxcarbazepine 2000 Zonisamide 2000 Other Available AEDs Diazepam, Lorazepam, Diastat, Depacon, ACTH……
Year Introduced Phenobarbital 1912 Phenytoin 1938 Primidone 1954 Ethosuximide 1960 Carbamazepine 1974 Valproate 1978 Felbamate 1993 Gabapentin 1993 Lamotrigine 1994 Topiramate 1996 Tiagibine 1997 Levetiracetam 2000 Oxcarbazepine 2000 Zonisamide 2000 Other Available AEDs Diazepam, Lorazepam, Diastat, Depacon, ACTH……
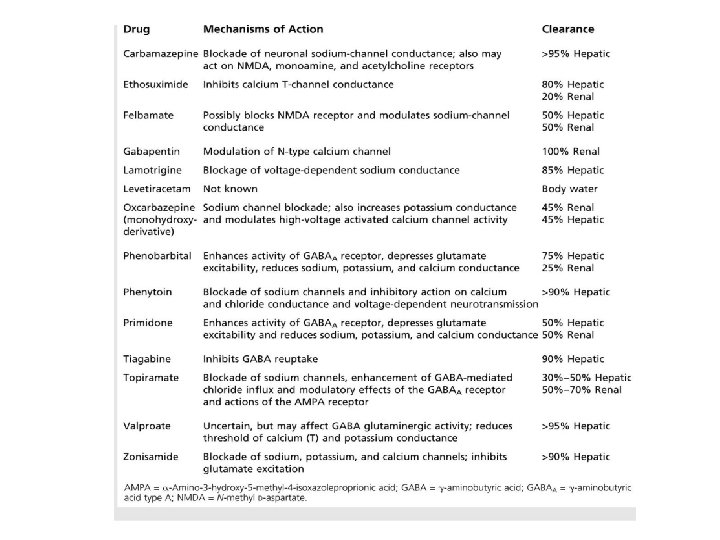
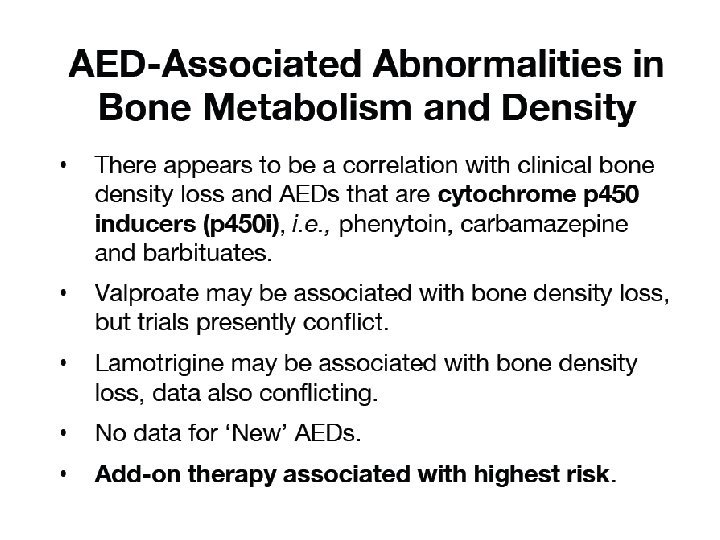
 Major Side Effects Phenobarbital Sedation, Hyperactivity, Rash, Osteomalacia Phenytoin Gingival hyperplasia, Hirsutism, Peripheral Neuropathy, Bone marrow suppression, Osteomalacia Primidone Sedation, Hyperactivity, Rash, Osteomalacia Ethosuximide Carbamazepine GI Upset, Mood changes, Lethargy, Hiccups, Headache Hyponatremia, Leucopoenia, Hepatitis, Rash Valproate Thrombocytopenia, Tremor, Hair loss, Weight gain, Hepatitis, Pancreatitis Felbamate Hepatic Failure, Aplastic Anemia Gabapentin Sleepiness, Weight gain Lamotrigine Rash (increased risk with VPA) Topiramate Cognitive slowing, Renal stones, Acute Glaucoma, Weight Loss Tiagibine Dizziness, Somnolence, Spike Wave Stupor Levetiracetam Sleepiness Oxcarbazepine Hyponatremia, Rash (No Leucopoenia) Zonisamide Rash, Renal stones
Major Side Effects Phenobarbital Sedation, Hyperactivity, Rash, Osteomalacia Phenytoin Gingival hyperplasia, Hirsutism, Peripheral Neuropathy, Bone marrow suppression, Osteomalacia Primidone Sedation, Hyperactivity, Rash, Osteomalacia Ethosuximide Carbamazepine GI Upset, Mood changes, Lethargy, Hiccups, Headache Hyponatremia, Leucopoenia, Hepatitis, Rash Valproate Thrombocytopenia, Tremor, Hair loss, Weight gain, Hepatitis, Pancreatitis Felbamate Hepatic Failure, Aplastic Anemia Gabapentin Sleepiness, Weight gain Lamotrigine Rash (increased risk with VPA) Topiramate Cognitive slowing, Renal stones, Acute Glaucoma, Weight Loss Tiagibine Dizziness, Somnolence, Spike Wave Stupor Levetiracetam Sleepiness Oxcarbazepine Hyponatremia, Rash (No Leucopoenia) Zonisamide Rash, Renal stones
 of Medications n dose-dependent side effects are") Epilepsy in the Elderly Adverse Effects (AE) of Medications n dose-dependent side effects are n drug-specific side effects are n n common: dizziness, somnolence, ataxia, diplopia common hyponatremia, tremor, cardiac effects, encephalopathy, cognitive suppression AE’s occur at lower serum concentrations AE’s more likely to result in noncompliance
Epilepsy in the Elderly Adverse Effects (AE) of Medications n dose-dependent side effects are n drug-specific side effects are n n common: dizziness, somnolence, ataxia, diplopia common hyponatremia, tremor, cardiac effects, encephalopathy, cognitive suppression AE’s occur at lower serum concentrations AE’s more likely to result in noncompliance
 Weight Gain/Loss n n Most medications are weight neutral Valproic Acid and Gabapentin typically associated with weight gain Felbamate, Topiramate and Zonisamide associated with weight loss Zonisamide n n Weight loss: 28. 9% of patients on ZNS compared to 8. 4% on placebo lost more than 5 lbs. Weight loss occurred in the first 3 months
Weight Gain/Loss n n Most medications are weight neutral Valproic Acid and Gabapentin typically associated with weight gain Felbamate, Topiramate and Zonisamide associated with weight loss Zonisamide n n Weight loss: 28. 9% of patients on ZNS compared to 8. 4% on placebo lost more than 5 lbs. Weight loss occurred in the first 3 months
 Hyponatremia n n Seen with carbamazepine and oxcarbazepine Clinically significant hyponatremia (sodium <125 m. Eq/L) has been observed in 2. 5% of OXC-treated patients in controlled clinical trials n Measurement of serum sodium levels should be considered for patients at risk for hyponatremia Most (79%) of these patients were receiving concomitant sodium-depleting medications including carbamazepine, antidepressants, diuretics, and cathartics The observed hyponatremia was usually asymptomatic and occurred within the first 90 days of treatment
Hyponatremia n n Seen with carbamazepine and oxcarbazepine Clinically significant hyponatremia (sodium <125 m. Eq/L) has been observed in 2. 5% of OXC-treated patients in controlled clinical trials n Measurement of serum sodium levels should be considered for patients at risk for hyponatremia Most (79%) of these patients were receiving concomitant sodium-depleting medications including carbamazepine, antidepressants, diuretics, and cathartics The observed hyponatremia was usually asymptomatic and occurred within the first 90 days of treatment
 Renal Stones n n Can occur with TPM, ZNS, Ketogenic Diet ~4% incidence of all clinically possible or confirmed kidney stones n n Less than 50% of calculi are symptomatic Analyzed stones are mostly composed of calcium or urate salts No increased risk of stone in patients on Ketogenic diet and ZNS or TPM History of calculi may not be absolute contraindication for use of the AED’s n Richards et al. , Neurology 2005
Renal Stones n n Can occur with TPM, ZNS, Ketogenic Diet ~4% incidence of all clinically possible or confirmed kidney stones n n Less than 50% of calculi are symptomatic Analyzed stones are mostly composed of calcium or urate salts No increased risk of stone in patients on Ketogenic diet and ZNS or TPM History of calculi may not be absolute contraindication for use of the AED’s n Richards et al. , Neurology 2005
 Choice of Therapy n Partial Seizure n n n Oxcarbazepine Lamotrigine Zonisamide Levetiracetam, Pregabalin, Phenytoin Generalized Seizures n n Topiramate Lamotrigine Valproic Acid Zonisamide
Choice of Therapy n Partial Seizure n n n Oxcarbazepine Lamotrigine Zonisamide Levetiracetam, Pregabalin, Phenytoin Generalized Seizures n n Topiramate Lamotrigine Valproic Acid Zonisamide
 New AED’s: FDA Approved Indications Seizure Type and Age Range Felbamate Gabapentin Lamotrigine Initial Monotherapy Partial with and without generalization in adults LSG: Pediatric and Adult Yes Partial with and without generalization above age 12 Partial from 3 -12 No Partial: Adults No (Approved for Conversion to Monotherapy) No LGS: Pediatric and Adult No No Topiramate Partial: Pediatric (>2) and adults Primary GTC LGS Yes (Adults and Children>10) Tiagibine Partial: Adults and Children (>12) No Levetiracetam Partial: Adults No Oxcarbazepine Partial: Adults and Children (>2) Yes (Children and Adults >4) Partial: Adults No Zonisamide
New AED’s: FDA Approved Indications Seizure Type and Age Range Felbamate Gabapentin Lamotrigine Initial Monotherapy Partial with and without generalization in adults LSG: Pediatric and Adult Yes Partial with and without generalization above age 12 Partial from 3 -12 No Partial: Adults No (Approved for Conversion to Monotherapy) No LGS: Pediatric and Adult No No Topiramate Partial: Pediatric (>2) and adults Primary GTC LGS Yes (Adults and Children>10) Tiagibine Partial: Adults and Children (>12) No Levetiracetam Partial: Adults No Oxcarbazepine Partial: Adults and Children (>2) Yes (Children and Adults >4) Partial: Adults No Zonisamide
 Issues To Discuss n n Driving Interaction with contraceptives n n n Pregnancy issues n n n >50μg ethinyl estradiol/mestranol if taking enzyme -inducing AED (phenobarbital, primidone, phenytoin, carbamazepine) OC’s do not alter seizure control, but they may accelerate metabolism of enzyme-inducing AED Decreased serum drug concentrations Birth defects Eventual outcome of treatment
Issues To Discuss n n Driving Interaction with contraceptives n n n Pregnancy issues n n n >50μg ethinyl estradiol/mestranol if taking enzyme -inducing AED (phenobarbital, primidone, phenytoin, carbamazepine) OC’s do not alter seizure control, but they may accelerate metabolism of enzyme-inducing AED Decreased serum drug concentrations Birth defects Eventual outcome of treatment
 Driving in Texas n n n Doctors not required to report patients Seizure-Free Period: 6 months, with doctor's recommendation Annual periodic medical updates required Doctors not liable for their opinions and recommendations Allowed to drive if: n Only nocturnal seizures n Breakthrough seizure due to a physician directed change in medication Intrastate License: The U. S. Department of Transportation (DOT) bars anyone with any history of epilepsy
Driving in Texas n n n Doctors not required to report patients Seizure-Free Period: 6 months, with doctor's recommendation Annual periodic medical updates required Doctors not liable for their opinions and recommendations Allowed to drive if: n Only nocturnal seizures n Breakthrough seizure due to a physician directed change in medication Intrastate License: The U. S. Department of Transportation (DOT) bars anyone with any history of epilepsy
 Interaction with Hormonal Contraception n Definite/Possible interaction n n n Carbamazepine Oxcarbazepine Phenobarbital Phenytoin Tiagabine *Topiramate **Lamotrigine (OCD’s reduce LTG levels) n No interaction n n Felbamate Gabapentin Levetiracetam Zonisamide
Interaction with Hormonal Contraception n Definite/Possible interaction n n n Carbamazepine Oxcarbazepine Phenobarbital Phenytoin Tiagabine *Topiramate **Lamotrigine (OCD’s reduce LTG levels) n No interaction n n Felbamate Gabapentin Levetiracetam Zonisamide
 Malformations") Pregnancy and Delivery n n Higher fetal death rate (~ 1. 3 -14%) Malformations of 2 main types: n n “Minor” malformations: Cleft lip, Cleft palate, digit and crease abnormalities n Fetal hydantoin syndrome n Fetal anticonvulsant syndrome “Major” malformations: Neural tube defects
Pregnancy and Delivery n n Higher fetal death rate (~ 1. 3 -14%) Malformations of 2 main types: n n “Minor” malformations: Cleft lip, Cleft palate, digit and crease abnormalities n Fetal hydantoin syndrome n Fetal anticonvulsant syndrome “Major” malformations: Neural tube defects
 Malformations n Risk factors: n n Polytherapy Uncontrolled seizures n n Both GTC and CPS Higher plasma levels of medications Neural tube defects: VPA Mechanism n ? Association with folate metabolism n n Enzyme-inducing AEDs accelerate folate metabolism VPA interferes with folate absorption
Malformations n Risk factors: n n Polytherapy Uncontrolled seizures n n Both GTC and CPS Higher plasma levels of medications Neural tube defects: VPA Mechanism n ? Association with folate metabolism n n Enzyme-inducing AEDs accelerate folate metabolism VPA interferes with folate absorption
 Pregnancy: Recommendations n Pre-Pregnancy n n n Limit risk factors Genetic counseling High risk Obstetrician Folic acid supplementation 400 micrograms/day (70% reduction in neural tube defect incidence) ENROLL IN PREGNANCY REGISTRY Level 2 ultrasound at 16 -18 weeks Amniocentesis if indicated Delivery n Vitamin K 10 mg/day, during last week to prevent Hemorrhagic Disease due to reduced activity of Vit K-dependent clotting factors (II, VII, IX, X) and protein S/C with enzyme-inducing AEDs
Pregnancy: Recommendations n Pre-Pregnancy n n n Limit risk factors Genetic counseling High risk Obstetrician Folic acid supplementation 400 micrograms/day (70% reduction in neural tube defect incidence) ENROLL IN PREGNANCY REGISTRY Level 2 ultrasound at 16 -18 weeks Amniocentesis if indicated Delivery n Vitamin K 10 mg/day, during last week to prevent Hemorrhagic Disease due to reduced activity of Vit K-dependent clotting factors (II, VII, IX, X) and protein S/C with enzyme-inducing AEDs
 Pregnancy: Recommendations n n VPA and PB seem to have highest risk for neural tube defects Monitor AED levels closely n n LTG levels will decrease by 50% by end of second trimester No AED is completely safe n Association of LTG with cleft lip/palate
Pregnancy: Recommendations n n VPA and PB seem to have highest risk for neural tube defects Monitor AED levels closely n n LTG levels will decrease by 50% by end of second trimester No AED is completely safe n Association of LTG with cleft lip/palate
 Outcome of Medical Management n Kwan and Brodie, NEJM 2000 n Prospective study n n 525 patients 9 -93 yrs of age Patients diagnosed, treated and followed at a single center for 13 years ~60% respond to the first to medications Significant number of patients have side effects
Outcome of Medical Management n Kwan and Brodie, NEJM 2000 n Prospective study n n 525 patients 9 -93 yrs of age Patients diagnosed, treated and followed at a single center for 13 years ~60% respond to the first to medications Significant number of patients have side effects
 Medical Intractability n n n Unacceptable control despite multiple drugs Acceptable control with unacceptable side effects Reasons for unsatisfactory control n n n Correct AED, but not working Incorrect AED Incorrect diagnosis n ~ 10 -20% of patients have “non-epileptic events”
Medical Intractability n n n Unacceptable control despite multiple drugs Acceptable control with unacceptable side effects Reasons for unsatisfactory control n n n Correct AED, but not working Incorrect AED Incorrect diagnosis n ~ 10 -20% of patients have “non-epileptic events”
 Options For Medically Intractable Patients n n Epilepsy Surgery Other: n Brain Stimulation n n Vagal Nerve Stimulation Cerebellar, Caudate, Thalamus, Hippocampus
Options For Medically Intractable Patients n n Epilepsy Surgery Other: n Brain Stimulation n n Vagal Nerve Stimulation Cerebellar, Caudate, Thalamus, Hippocampus
 Engel J. NEJM 1996 Outcomes,") Results of Surgical Treatment, Worldwide (1986 -1990; Retrospective Data) Engel J. NEJM 1996 Outcomes, % Surgical Procedure Patients Seizurefree Worthwhile improvemen t No Worthwhile improvement 3579 67. 9 24. 0 8. 1 Amygdalohippocampectomy 413 68. 8 22. 3 9. 0 Neocortical resection 605 45. 1 35. 2 19. 8 Lesionectomy 293 66. 6 21. 5 11. 9 Hemispherectomy 190 67. 4 21. 1 11. 6 Multilobar resection 166 45. 2 35. 5 19. 3 Callosotomy 563 7. 6 60. 9 31. 4 Temporal lobe resections - Anterior temporal lobectomy
Results of Surgical Treatment, Worldwide (1986 -1990; Retrospective Data) Engel J. NEJM 1996 Outcomes, % Surgical Procedure Patients Seizurefree Worthwhile improvemen t No Worthwhile improvement 3579 67. 9 24. 0 8. 1 Amygdalohippocampectomy 413 68. 8 22. 3 9. 0 Neocortical resection 605 45. 1 35. 2 19. 8 Lesionectomy 293 66. 6 21. 5 11. 9 Hemispherectomy 190 67. 4 21. 1 11. 6 Multilobar resection 166 45. 2 35. 5 19. 3 Callosotomy 563 7. 6 60. 9 31. 4 Temporal lobe resections - Anterior temporal lobectomy
 Risks of Epilepsy Surgery n Wiebe S et al, NEJM 2001 n n 10% complications in surgery group, 1 death (2. 5%) in medical management group Rydenhag and Silander, Neurosurgery 2000, 449 procedures n n Risk is higher with n n n Major complications 3. 1%, Minor 8. 9% Intracranial electrode placement Extra-temporal surgery especially in/around eloquent cortex Pre-operative w/u (Neuropsychological testing, Amobartbital test) provides assessment of post-operative memory problems Superior quadrantanopsia ~ 30% patients (assymptomatic) Post-operative depression/psychosis
Risks of Epilepsy Surgery n Wiebe S et al, NEJM 2001 n n 10% complications in surgery group, 1 death (2. 5%) in medical management group Rydenhag and Silander, Neurosurgery 2000, 449 procedures n n Risk is higher with n n n Major complications 3. 1%, Minor 8. 9% Intracranial electrode placement Extra-temporal surgery especially in/around eloquent cortex Pre-operative w/u (Neuropsychological testing, Amobartbital test) provides assessment of post-operative memory problems Superior quadrantanopsia ~ 30% patients (assymptomatic) Post-operative depression/psychosis
 Outpatient Management: Conclusions n n n Epilepsy is an extremely common condition ~60% of patients are well controlled on a single first appropriate medication Early identification of medically refractory patients Epilepsy surgery is an effective and safe treatment Goal is Seizure Freedom
Outpatient Management: Conclusions n n n Epilepsy is an extremely common condition ~60% of patients are well controlled on a single first appropriate medication Early identification of medically refractory patients Epilepsy surgery is an effective and safe treatment Goal is Seizure Freedom
 Status Epilepticus n Definition: n n Incidence: n n 2 or more seizures without full recovery or more or less continuous seizure activity lasting >30 minutes 50, 000 -150, 000 cases annually in the U. S. Most common in children and the elderly
Status Epilepticus n Definition: n n Incidence: n n 2 or more seizures without full recovery or more or less continuous seizure activity lasting >30 minutes 50, 000 -150, 000 cases annually in the U. S. Most common in children and the elderly
 Etiology n Prior history of seizures: n n Most common: Medication changes or non-compliance Breakthrough seizures because of stress, lack of sleep, menstrual cycles. Unknown New Onset: n n n Metabolic problems e. g. , electrolyte disturbances, renal failure, sepsis and hypoxia, especially in the hospitalized patient Head trauma, central nervous system infection and cerebral hemorrhage or infarction. Intracranial tumors, substance abuse or other drug toxicity/withdrawal and HIV.
Etiology n Prior history of seizures: n n Most common: Medication changes or non-compliance Breakthrough seizures because of stress, lack of sleep, menstrual cycles. Unknown New Onset: n n n Metabolic problems e. g. , electrolyte disturbances, renal failure, sepsis and hypoxia, especially in the hospitalized patient Head trauma, central nervous system infection and cerebral hemorrhage or infarction. Intracranial tumors, substance abuse or other drug toxicity/withdrawal and HIV.
 Generalized Convulsive SE n n n Most common type of SE ~70% of all cases of SE ~65, 000 -150, 000 new cases every year Responsible for considerable morbidity and mortality (~3 -53%) Prevalence of nonconvulsive status epilepticus in comatose patients: 8% (236 patients with no overt seizure activity) n Towne et al. , Neurology 2000
Generalized Convulsive SE n n n Most common type of SE ~70% of all cases of SE ~65, 000 -150, 000 new cases every year Responsible for considerable morbidity and mortality (~3 -53%) Prevalence of nonconvulsive status epilepticus in comatose patients: 8% (236 patients with no overt seizure activity) n Towne et al. , Neurology 2000
 Standard Treatment Algorithm: Initial Treatment n n n Assess and control airway (100% oxygen, intubation if needed) Monitor vital signs (including temperature)-hyperthermia occurs in 29 -78%, passive cooling or cooling blanket if needed (hyperpyrexia is an important cause of poor outcome) Conduct pulse oximetry and monitor cardiac function Perform finger-stick blood glucose Call EEG technician and begin EEG stat.
Standard Treatment Algorithm: Initial Treatment n n n Assess and control airway (100% oxygen, intubation if needed) Monitor vital signs (including temperature)-hyperthermia occurs in 29 -78%, passive cooling or cooling blanket if needed (hyperpyrexia is an important cause of poor outcome) Conduct pulse oximetry and monitor cardiac function Perform finger-stick blood glucose Call EEG technician and begin EEG stat.
 While you are treating…… n n n Begin focused history and examine patient Known seizure disorder or other illnesses? Trauma? Focal neurological signs? Signs of medical illnesses (e. g. infection, hepatic or renal disease, substance abuse? ) Throughout protocol: n Manage other medical problems n Determine and treat underlying etiology of status
While you are treating…… n n n Begin focused history and examine patient Known seizure disorder or other illnesses? Trauma? Focal neurological signs? Signs of medical illnesses (e. g. infection, hepatic or renal disease, substance abuse? ) Throughout protocol: n Manage other medical problems n Determine and treat underlying etiology of status
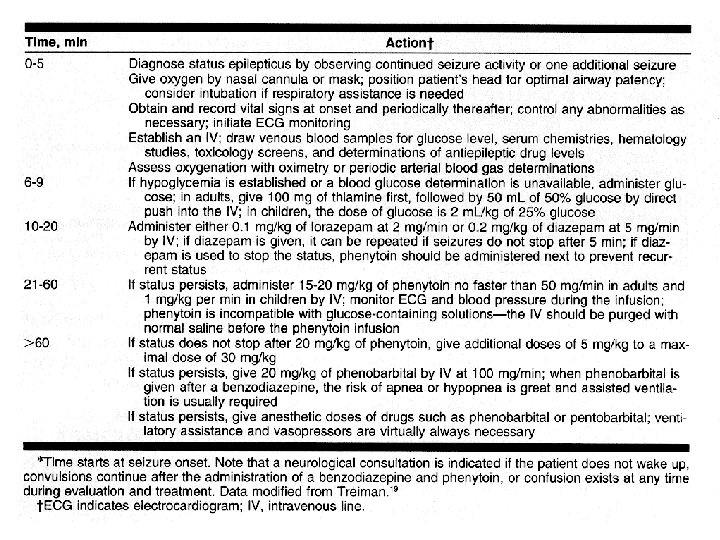
 VA cooperative trial of 384 patients with a diagnosis of overt generalized status epilepticus Treiman et al: NEJM 1998 Lorazepam is reasonable as the initial drug of choice in the treatment of GCSE.
VA cooperative trial of 384 patients with a diagnosis of overt generalized status epilepticus Treiman et al: NEJM 1998 Lorazepam is reasonable as the initial drug of choice in the treatment of GCSE.
 Midazolam n n Propofol n n") Other Medications n n Rectal Diazepam Gel (Diastat@) Midazolam n n Propofol n n 0. 1 -0. 3 mg/kg slow IVP followed by 0. 05 -0. 4 mg/kg/hr infusion 2 -2. 5 mg/kg IV (40 mg q 10 min) followed by 0. 1 -0. 2 mg/kg/min IV IV Valproate (Depacon@) n 15 -20 mg/kg IV followed by 250 -500 mg q 6 hrs
Other Medications n n Rectal Diazepam Gel (Diastat@) Midazolam n n Propofol n n 0. 1 -0. 3 mg/kg slow IVP followed by 0. 05 -0. 4 mg/kg/hr infusion 2 -2. 5 mg/kg IV (40 mg q 10 min) followed by 0. 1 -0. 2 mg/kg/min IV IV Valproate (Depacon@) n 15 -20 mg/kg IV followed by 250 -500 mg q 6 hrs
 Status Epilepticus: Goal n n Stop seizures as quickly and as aggressively as possible Duration of status correlates inversely with outcome
Status Epilepticus: Goal n n Stop seizures as quickly and as aggressively as possible Duration of status correlates inversely with outcome
 Additional Information…. . n Epilepsy Foundation of America n n www. efa. org National Institute of Neurological Disorders and Stroke (NINDS) n www. ninds. nih. gov
Additional Information…. . n Epilepsy Foundation of America n n www. efa. org National Institute of Neurological Disorders and Stroke (NINDS) n www. ninds. nih. gov