1b1bcf95d52a72c191a6007f77f509a4.ppt
- Количество слайдов: 34



Malaria Infectious Diseases - A challenge to global health: clinical, social and preventive aspects

Overview of the lecture § § § § Introduction and overview of the field - 30 min Break - 15 min Group discussions I – 35 min Group discussions II - 35 min Break 15 min Group presentations – 30 min Summary– 20 min

Why learn about malaria? § Life-threatening disease caused by parasites transmitted through mosquito bites § In 2012 caused an estimated 627 000 deaths § In 2012 an estimated 207 million malaria cases § Every minute a child dies from malaria § BUT MALARIA CAN BE TREATED!

Source: RBM Info sheet Morbidity and mortality Loss of productivity or education

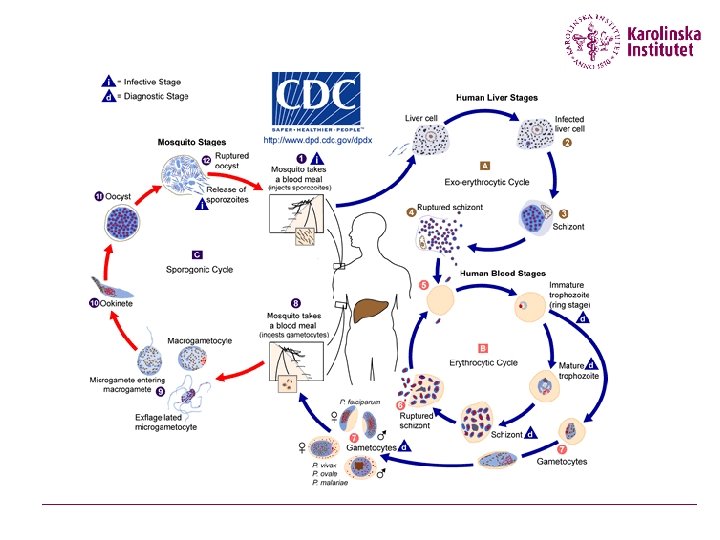
Malaria – what is it? § Plasmodium parasite à Falciparum à Vivax à Malariae à Ovale à Knowlesi § Transmitted by Anopheles mosquitoes § Transmission depends on parasite , vector, human host and the environment

Namn Efternamn 3/16/2018 7

Symptoms § Acute febrile illness § Symptoms 7 days of more after infective bite § Fever, headache, chills § Severe malaria – within 24 hrs à Severe anemia à Cerebral malaria à Respiratory distress (acidosis)

Malaria – who is affected? § Half of the world’s population! § § Young children Pregnant women People with HIV/AIDS International travellers

How to diagnose Malaria? § Syndromic à based on presence/history of fever § Microscopy à Needs skilled technician, microscope, slides, staining material etc à Time consuming but relatively cheep à Detection limit under field conditions 50 parasites/microlitre blood § Rapid Diagnostic Tests (RDT) à Relatively expensive à Minimum training needed à Can not quantify parasites à Remains positive after treatment – not monitor treatment outcome § LIVER STAGE OF P. VIVAX – no tests! 16 March 2018 10

Microscopy 16 March 2018 11

RDT 16 March 2018 12

How to treat malaria? § Two outstanding antimalarial drugs are based on herbal remedies à Quinine (2 nd line for severe malaria) à Artemisinin-derivatives WHO advocates combination therapy to à Improve efficiacy à Delay development of resistance Non severe malaria: Artemisinin-based combination therapy (ACT) Severe malaria: Artesunat (IV or IM) 16 March 2018 13

Artemisinin-based combination therapy § A majority of malaria endemic countries have adopted ACTs as treatment of choice for uncomplicated malaria’ § Positive: à Rapid reduction of parasite biomass à Rapid resolution of clinical symptoms (fever) à Effective action against multi-drug resistant P. Falciparum à Probably delay the development of resistance à Few reported adverse effects § Negative à Much more expensive à increased need for rational use à and improved diagnostics 16 March 2018 14
 § Artesunate+amodiaquine (Arsucam. R,")
Few ACT combinations available. . . § Artemether-lumefantrine (Coartem. R) § Artesunate+amodiaquine (Arsucam. R, Coarsucam. R) § Artesunate+mefloquine § Artesunate+sulfadoxine-pyrimethamine § Dihydroartemisinin-piperaquine (Artekin. R) § MONOTHERAPY may increase resistance devlopment!! 16 March 2018 15

4 months up to 5 -15 Kg 3 years 16

3 years up to 15 -25 Kg 7 years 17

Millenium Development Goals 1. 2. 3. 4. Eradicate Extreme Poverty and Hunger Achieve Universal Primary Education Promote Gender Equality and Empower Women Reduce Child Mortality Reduce by two-thirds, between 1990 and 2015, the under-five mortality rate 5. Improve Maternal Health 6. Combat HIV/AIDS, Malaria and other Diseases Halt and begin to reverse the incidence of malaria and other major diseases 7. Ensure Environmental Sustainability 8. Develop a Global Partnership for Development 16 March 2018 18

Group work § Discuss with people who have read the SAME article as you § Decide on the key messages from the article you have read à methods to control malaria? à problems related to malaria control? § Why are these the most important messages? § Write down your key messages – you will present you key messages to the class in five minutes

Group work II § Discuss with people who have read ANOTHER article than you - you are now the expert! § Each one present the key messages from your “expert group” § How does your different messages fit together?

The “E” words……. . 16 March 2018 21

The continuum from control to elimination/eradication Ref: WHO 2007 16 March 2018 22

”The Three-Part Strategy” 16 March 2018 23

Where is elimination possible? Elimination is most appropriate in countries: àthat meet epidemiological criteria for low burden; àwhere the potential for reintroduction via porous borders is being managed; àwhose leaders are politically and financially committed to elimination; àwhose health systems and surveillance capacity are sufficient to manage an elimination program àwhere parasite and vector species and technical factors make elimination feasible.
 § IPTp: At least two separate doses of sulfadoxine-pyrimethamine (SP)")
Intermittent preventive treatment (IPT) § IPTp: At least two separate doses of sulfadoxine-pyrimethamine (SP) in second and third trimester given as a single dose under observation of a health worker. § First dose when fetal movements are felt (18 -20 weeks gestation) and the second a month later. § HIV-positive women should receive three doses or all women if HIV prevalence exceeds 10% and HIV testing is not available § IPTi one dose of SP with DPT 2, DPT 3, measles vaccination § SMC. Full treatment course at monthly intervals in U 5 s in Sahel region during transmission season 16 March 2018 25

Bednets § Untreated Nets à Protective barrier around persons using them à Mosquitoes can feed on people through the nets or holes à Efficacy data scarce, but probably effective § ITNs – enhanced efficacy à Knock-down/lethal effect on insects à Repellent à Need retreatment after 6 -12 months § Long lasting insecticidal nets (LLINs) with an effect up to 5 years are available and recommended § Both additive effect on other night biting insect 16 March 2018 26

IRS § Primary vector control intervention for reducing and interrupting malaria transmission § Coordinated, timely spraying of the interior walls of homes with insecticides § Mosquitoes are killed when they rest on those walls § Substantially reduces infant and child mortality § Sprayed houses are protected for about 4 to 10 months, depending on the insecticide used and the housing construction § WHO has approved 12 insecticides it considers effective and safe for use in IRS, including DDT 16 March 2018 27

Today’s malaria control tools NOT SEEKING CARE § Early diagnosis § RDTs § Effective treatment ILLNESS RECOGNITION INTERPRETATION OF ILLNESS à ACTs COMPLIANCE § Intermittent preventive treatment (IPT pregnancy/infants/SMC) § Integrated vector control à Insecticide treated nets (ITN) / long lasting (LLIN) à Indoor residual spraying (IRS) DRUG/INSECTICIDE RESISTANCE WEAK HEALTH SYSTEMS COSTS NON MALARIA FEVERS 16 March 2018 28

Remember the Ears of the Hippo…. . Breman 2001 16 March 2018 29

What is CCM? § A care delivery strategy to increase access to effective treatment for uncomplicated malaria as a way for reducing mortality in children àWhere the health care system is far/weak àWhere self-treatment is common àWhere self-treatment is often inappropriate 30

Symptom overlap Recognition of the need to address comorbidities Fever 70% Cough + ‘Difficult/R apid Breathing’ 12% Diarrhoea 36% 28% n=3715 health facility consultations Källander et al. 2009
 § Many children with malaria do not")
Need antimalarials (but may not receive them) § Many children with malaria do not reach formal health care facilities § Many children who access care in the private sector are not prescribed antimalarials § Even if antimalarials are available in public facilities, children may not receive them àIn Zambia after policy change, AL available in 51% of HCF, but only 22% of children received AL (Zurovac, BMJ 2005; 331: 734)
 § Presumptive treatment of fever with antimalarials")
Receive antimalarials (but may not need them) § Presumptive treatment of fever with antimalarials widely advocated (HBMF) § Overdiagnosis of malaria is very common àUp to 78% overestimation by clinical diagnosis (Amexo, Lancet 2004; 364: 1896) § Even when microscopy is available → often not utilized or results are ignored àIn TZ, 48% of cases with negative BS treated with antimalarials (Reyburn, Malaria J 2006; 5: 4) § Bacterial illnesses requiring antibiotics may be missed (Berkley, BMJ 2005; 330: 995)

THANK YOU!
1b1bcf95d52a72c191a6007f77f509a4.ppt