

d5180ea8398ead599ab69e7d34b12c08.ppt
- Количество слайдов: 43
 Making the Move to PACS Monte Clinton, CRA Dartmouth-Hitchcock Medical Center
Making the Move to PACS Monte Clinton, CRA Dartmouth-Hitchcock Medical Center
 with one") Disclaimer This presentation is about a PACS implementation at one facility (DHMC) with one vendor (IDX) and is being given as an example of a successful PACS implementation Other facilities and vendors can do a similar PACS implementation using this partnering program and methodology DHMC does not endorse IDX or any other vendor’s products and services
Disclaimer This presentation is about a PACS implementation at one facility (DHMC) with one vendor (IDX) and is being given as an example of a successful PACS implementation Other facilities and vendors can do a similar PACS implementation using this partnering program and methodology DHMC does not endorse IDX or any other vendor’s products and services
 Radiology Equipment 2004 Existing 3 MR + 1 Mobile 3 CT 3 VIR + 1 PICC 8 DX 3 R/F 5 US 3 NM + PET/CT 5 Mammo New in 2004 Replace in 2004 1 CT in new ED 1 CT/Angio 2 1 Angio OR compatible 3 6 DR-- 4 CR 4 1 DR/CR in ED + 1 CR trauma 5 1 DR/Fluoro 6 2 US in new building 7 1 NM + Fixed PET/CT 8 2 DR – Mammo new building
Radiology Equipment 2004 Existing 3 MR + 1 Mobile 3 CT 3 VIR + 1 PICC 8 DX 3 R/F 5 US 3 NM + PET/CT 5 Mammo New in 2004 Replace in 2004 1 CT in new ED 1 CT/Angio 2 1 Angio OR compatible 3 6 DR-- 4 CR 4 1 DR/CR in ED + 1 CR trauma 5 1 DR/Fluoro 6 2 US in new building 7 1 NM + Fixed PET/CT 8 2 DR – Mammo new building
 Why Install a PACS? • Expansion to Provide New Space for: • Mammography • Nuclear Medicine • Vascular Interventional • Offices and conference space • New Outpatient Clinical Building to: • Eliminate over crowding • Add new MDs and exam rooms • Bring imaging to the patient • Minimize radiologist travel
Why Install a PACS? • Expansion to Provide New Space for: • Mammography • Nuclear Medicine • Vascular Interventional • Offices and conference space • New Outpatient Clinical Building to: • Eliminate over crowding • Add new MDs and exam rooms • Bring imaging to the patient • Minimize radiologist travel
 Why Install a PACS? Save money – Increase reimbursement Reduce medico-legal risk • Eliminate Film and processing costs • Reduce Film Library staff and space • Improve billing collections • Reduce medico-legal exposure
Why Install a PACS? Save money – Increase reimbursement Reduce medico-legal risk • Eliminate Film and processing costs • Reduce Film Library staff and space • Improve billing collections • Reduce medico-legal exposure

 Why Install a PACS? Improve staff and imaging room productivity • Increased staff productivity • Reduction in the number of staff • Increased imaging room productivity • Eliminate imaging rooms
Why Install a PACS? Improve staff and imaging room productivity • Increased staff productivity • Reduction in the number of staff • Increased imaging room productivity • Eliminate imaging rooms

 Why Install a PACS? Improve service to your customers • Single set of film images limits collaboration • Minimize lost studies and revenue • Minimize treatment delays • Speed service to referring clinician and patient
Why Install a PACS? Improve service to your customers • Single set of film images limits collaboration • Minimize lost studies and revenue • Minimize treatment delays • Speed service to referring clinician and patient
 DHMC’s Steps to Justify PACS Internal justification – The major players • Large capital or operating cost impact requires multiple levels of approval – at DHMC this was: – Radiology – Information Systems
DHMC’s Steps to Justify PACS Internal justification – The major players • Large capital or operating cost impact requires multiple levels of approval – at DHMC this was: – Radiology – Information Systems
 DHMC’s Steps to Justify PACS Internal justification – Institutional leadership – Administrative leadership – Finance Committee – Board of Trustees – final go or no go
DHMC’s Steps to Justify PACS Internal justification – Institutional leadership – Administrative leadership – Finance Committee – Board of Trustees – final go or no go
 PACS: Getting Started Outside experts – PACS consultants Institutional experts • Radiology • Information Systems
PACS: Getting Started Outside experts – PACS consultants Institutional experts • Radiology • Information Systems
 PACS: Getting Started Educate yourself about PACS Ask your colleagues about their experiences Attend meetings such as this one Vendor discussions and demonstrations at trade shows - AHRA, RSNA, SCAR Understand your own environment and needs
PACS: Getting Started Educate yourself about PACS Ask your colleagues about their experiences Attend meetings such as this one Vendor discussions and demonstrations at trade shows - AHRA, RSNA, SCAR Understand your own environment and needs
 • Invite selected vendors to respond to") PACS: Getting Started Request for Information (RFI) • Invite selected vendors to respond to RFI • Get a list of their customers to contact • How would their system fit into your facility • RIS and PACS compatibility
PACS: Getting Started Request for Information (RFI) • Invite selected vendors to respond to RFI • Get a list of their customers to contact • How would their system fit into your facility • RIS and PACS compatibility
 Interface or Integrate The critical relationship between the RIS and the PACS Have the RIS and the PACS vendors worked together before? Which vendor has primary responsibility or are you expected to do problem triage?
Interface or Integrate The critical relationship between the RIS and the PACS Have the RIS and the PACS vendors worked together before? Which vendor has primary responsibility or are you expected to do problem triage?
 • Invite a limited number of vendors") PACS: Getting Started Request for proposal (RFP) • Invite a limited number of vendors to bid • Vendor clarification meetings • RFP review and analysis • Site visits at working clinical sites • Final negotiation – Purchasing and Vendors
PACS: Getting Started Request for proposal (RFP) • Invite a limited number of vendors to bid • Vendor clarification meetings • RFP review and analysis • Site visits at working clinical sites • Final negotiation – Purchasing and Vendors
 Paying for a PACS Capital Purchase or Operating Expense • Capital purchase – Major capital expense – compete for funding – Cost to upgrade and remain technologically current – Ongoing service and maintenance cost • Application Service Provider (ASP) – Costs are an operating expense – Always kept technologically current – All inclusive - charges fluctuate with activity
Paying for a PACS Capital Purchase or Operating Expense • Capital purchase – Major capital expense – compete for funding – Cost to upgrade and remain technologically current – Ongoing service and maintenance cost • Application Service Provider (ASP) – Costs are an operating expense – Always kept technologically current – All inclusive - charges fluctuate with activity
 The PACS Timeline Develop a realistic implementation timeline with buy-in from all affected stakeholders Radiology – all levels Information Systems Institutional Leadership Referring Clinicians PACS Vendor
The PACS Timeline Develop a realistic implementation timeline with buy-in from all affected stakeholders Radiology – all levels Information Systems Institutional Leadership Referring Clinicians PACS Vendor
 DHMC’s PACS Timeline • Phase 1 • 1 -2003 • 4 -2003 Archiving started in CT, MR, US Live in CT, MR and US – stop film • Phase 2 • 9 -2003 • 12 -2003 Archiving started in DX Live in DX – stop printing film • Phase 3 • 8 -2004 • 1 -2005 Archiving started in Angio and NM after IDXrad V 10
DHMC’s PACS Timeline • Phase 1 • 1 -2003 • 4 -2003 Archiving started in CT, MR, US Live in CT, MR and US – stop film • Phase 2 • 9 -2003 • 12 -2003 Archiving started in DX Live in DX – stop printing film • Phase 3 • 8 -2004 • 1 -2005 Archiving started in Angio and NM after IDXrad V 10
 Partnering with the PACS Vendor Agreement with the vendor on the timeline and implementation phases Appoint key staff from each stakeholder This must be a win – win endeavor
Partnering with the PACS Vendor Agreement with the vendor on the timeline and implementation phases Appoint key staff from each stakeholder This must be a win – win endeavor
 Planning the Implementation Weekly meetings of the PACS Working Group • • • Radiology Director Radiology PACS Administrator Radiology Clinical Operations Manager Radiology Asset Manager IS Director IS Liaison
Planning the Implementation Weekly meetings of the PACS Working Group • • • Radiology Director Radiology PACS Administrator Radiology Clinical Operations Manager Radiology Asset Manager IS Director IS Liaison
 Guiding the Implementation PACS Implementation Team bi-monthly meetings • Chairman of Radiology • Chief Information Officer • Vice President of Clinical Operations • The Six Working Group Members
Guiding the Implementation PACS Implementation Team bi-monthly meetings • Chairman of Radiology • Chief Information Officer • Vice President of Clinical Operations • The Six Working Group Members
 Before and After Implementation Ongoing follow-up • Weekly calls - Radiology and vendor • Updates to the clinical departments • Regular updates to the Board of Trustees • Monthly updates to the Radiology faculty • Weekly updates to the Radiology staff
Before and After Implementation Ongoing follow-up • Weekly calls - Radiology and vendor • Updates to the clinical departments • Regular updates to the Board of Trustees • Monthly updates to the Radiology faculty • Weekly updates to the Radiology staff
 Selecting the Hardware Involve the end user in equipment selection • Radiologists given a choice of monitors • Referring clinicians given a choice of monitors Specialty sections given choice of monitors • OR selected from 5 large flat panel monitors • ED selected the best monitor for their use
Selecting the Hardware Involve the end user in equipment selection • Radiologists given a choice of monitors • Referring clinicians given a choice of monitors Specialty sections given choice of monitors • OR selected from 5 large flat panel monitors • ED selected the best monitor for their use


 Reading Room Design Radiologists given a choice of layout • DHMC rejected the modular systems • Radiologists preferred two image monitors • Room lighting critical • Calculate room temperature requirements • Gradual phase out of alternators
Reading Room Design Radiologists given a choice of layout • DHMC rejected the modular systems • Radiologists preferred two image monitors • Room lighting critical • Calculate room temperature requirements • Gradual phase out of alternators

 Dealing with Prior Studies • DHMC chose not to digitize prior studies • Prior studies are available if needed • After six months there was very little need for prior studies • Some studies are digitized so they can be used for comparison – joint replacements
Dealing with Prior Studies • DHMC chose not to digitize prior studies • Prior studies are available if needed • After six months there was very little need for prior studies • Some studies are digitized so they can be used for comparison – joint replacements
 The Archive DHMC’s PACS Archive • In-house dual servers maintained and remotely monitored 24/7 by vendor • External archive backed up daily to vendor’s San Diego archive facility • DHMC’s failsafe back-up archive -- DVDs burned daily and stored at DHMC
The Archive DHMC’s PACS Archive • In-house dual servers maintained and remotely monitored 24/7 by vendor • External archive backed up daily to vendor’s San Diego archive facility • DHMC’s failsafe back-up archive -- DVDs burned daily and stored at DHMC
 Dartmouth Hitchcock Medical Center Imagecast™ RISv 9. 8/PACS CT Rad/Onc Fiber CT/Body Read Area (3) Image Archive CT GE - 3 10/100 MB Display Stations 100 MB Imagecast PACS database Imaging Suite Neuro Read Area (3) MR GE- 4 MR Mobile RF Siemens 3 DR Philips – 6 • Dual DICOM Processors (~3 weeks) U/S Read Area (2) • net. Cache (~6 months) • Persistent Store (scalable life) CR Philips - 3 DX Read Area (5) Connect. Rv 4. 0 IDXRad Offsite Disaster Recovery v 9. 8 ICU US – 7 HDI Acuson Film Digitizer 2 Onsite Disaster Recovery HC 5 10/100 MB Speare – Plymouth NH MR Mobile T-1 US – HDI 2 CT Picker 10 MB U/S Kodak Mini. PACS (priors only) 10/100 MB DVD Server Kodak Drylaser Printer - 5 T-1 Any Image, Anywhere, Anytime Enterprise Access via CIS LAN-10/100 Lebanon DHMC Campus WAN/DSL/Cable Dated 05/05/03
Dartmouth Hitchcock Medical Center Imagecast™ RISv 9. 8/PACS CT Rad/Onc Fiber CT/Body Read Area (3) Image Archive CT GE - 3 10/100 MB Display Stations 100 MB Imagecast PACS database Imaging Suite Neuro Read Area (3) MR GE- 4 MR Mobile RF Siemens 3 DR Philips – 6 • Dual DICOM Processors (~3 weeks) U/S Read Area (2) • net. Cache (~6 months) • Persistent Store (scalable life) CR Philips - 3 DX Read Area (5) Connect. Rv 4. 0 IDXRad Offsite Disaster Recovery v 9. 8 ICU US – 7 HDI Acuson Film Digitizer 2 Onsite Disaster Recovery HC 5 10/100 MB Speare – Plymouth NH MR Mobile T-1 US – HDI 2 CT Picker 10 MB U/S Kodak Mini. PACS (priors only) 10/100 MB DVD Server Kodak Drylaser Printer - 5 T-1 Any Image, Anywhere, Anytime Enterprise Access via CIS LAN-10/100 Lebanon DHMC Campus WAN/DSL/Cable Dated 05/05/03
 Training the Radiology Technologists and Support Staff • Modality integration in advance – Imaging Suite • Super users identified - trained in each section • On-line training with vendor for super users • Make the process exciting and rewarding
Training the Radiology Technologists and Support Staff • Modality integration in advance – Imaging Suite • Super users identified - trained in each section • On-line training with vendor for super users • Make the process exciting and rewarding
 Training of the Radiologists Vendor provided 1 to 2 hours of one on one training 2 to 3 days before activation • Return visits after activation for more training if needed • Give them all the time and training they want • Ask radiologists and residents to offer suggestions for enhancements
Training of the Radiologists Vendor provided 1 to 2 hours of one on one training 2 to 3 days before activation • Return visits after activation for more training if needed • Give them all the time and training they want • Ask radiologists and residents to offer suggestions for enhancements

 Keep Your Staff Informed • Being upfront about what is happening and when it will impact the lives of staff will head off rumors • Publish a PACS phase in plan – DHMC 1 year • Stop hiring permanent full time Film Library employees a year before implementation • Work with HR to find jobs for displaced staff
Keep Your Staff Informed • Being upfront about what is happening and when it will impact the lives of staff will head off rumors • Publish a PACS phase in plan – DHMC 1 year • Stop hiring permanent full time Film Library employees a year before implementation • Work with HR to find jobs for displaced staff
 Contingency Plans • Referring clinicians demanding film • Acceptance of CD copies by other facilities • Urgent results reporting • Special requests • System failure – power failure, virus, etc.
Contingency Plans • Referring clinicians demanding film • Acceptance of CD copies by other facilities • Urgent results reporting • Special requests • System failure – power failure, virus, etc.
 Partner With Your Vendor • Clear objectives spelled out in the contract • Agree on timeline, payment and penalties • Clearly define facility - vendor responsibilities • Track progress with regular reports Make the PACS implementation a win – win program for both your facility and the vendor
Partner With Your Vendor • Clear objectives spelled out in the contract • Agree on timeline, payment and penalties • Clearly define facility - vendor responsibilities • Track progress with regular reports Make the PACS implementation a win – win program for both your facility and the vendor
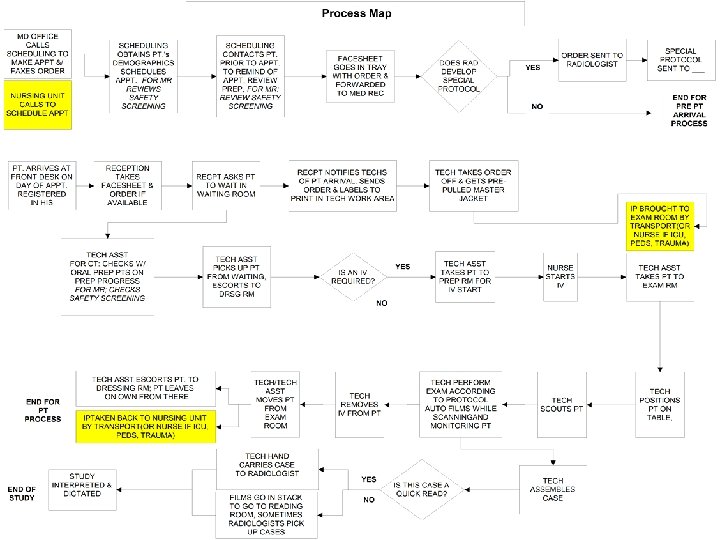
 What DHMC Did Right • Developed and used a workflow analysis • Piloted PACS with 15 referring clinicians • Had a close relationship with the PACS vendor • Integrated modalities in advance • Integrated RIS/PACS with electronic medical record
What DHMC Did Right • Developed and used a workflow analysis • Piloted PACS with 15 referring clinicians • Had a close relationship with the PACS vendor • Integrated modalities in advance • Integrated RIS/PACS with electronic medical record
 A Chairman’s Perspective “ Never in my 29 years as a chairman have I made a decision that has received such universal acceptance from both the radiologists and the referring clinicians” Peter Spiegel, MD Chairman – Radiology
A Chairman’s Perspective “ Never in my 29 years as a chairman have I made a decision that has received such universal acceptance from both the radiologists and the referring clinicians” Peter Spiegel, MD Chairman – Radiology
 A Director’s Perspective
A Director’s Perspective
 Contact Information Monte Clinton, CRA Dartmouth-Hitchcock Medical Center Monte. Clinton@Hitchcock. org www. dhmc. org/dept/radiology
Contact Information Monte Clinton, CRA Dartmouth-Hitchcock Medical Center Monte. Clinton@Hitchcock. org www. dhmc. org/dept/radiology