8ef3c3f15f44745ef270f40c3d2cff0e.ppt
- Количество слайдов: 19



M+M 25/07/2017 Dr. Patrick Abbott Recognition and Management of Sepsis and Shock

KC – 62 yo female Background of Hypertension Cholelithiasis Obesity Breast cancer and axillary clearance 2006 Bilateral TKRs KC RK 336011

3/52 hx of post-prandial upper abdominal pain and subjective fevers Gallstones on USS Treated with doxycycline and metronidazole by GP KC RK 336011

Acute increase in pain, waking pt from sleep late 10/05: RUQ/epigastric radiating to back Initial presentation at Biloela Hospital at 0100 hrs 11/05, c/o 10/10 pain Seen by NS who called GP-SMO on call and got a phone order for S/C morphine, IM metoclopramide, and PO hyoscine Permission to repeat morphine Q 2 H PRN KC RK 336011

No documentation from treating clinician are present in EDIS or in Progress Notes Based on nursing notes, pt cannulated by a different doctor ~1300 hrs, i. Stat bloods done KC RK 336011

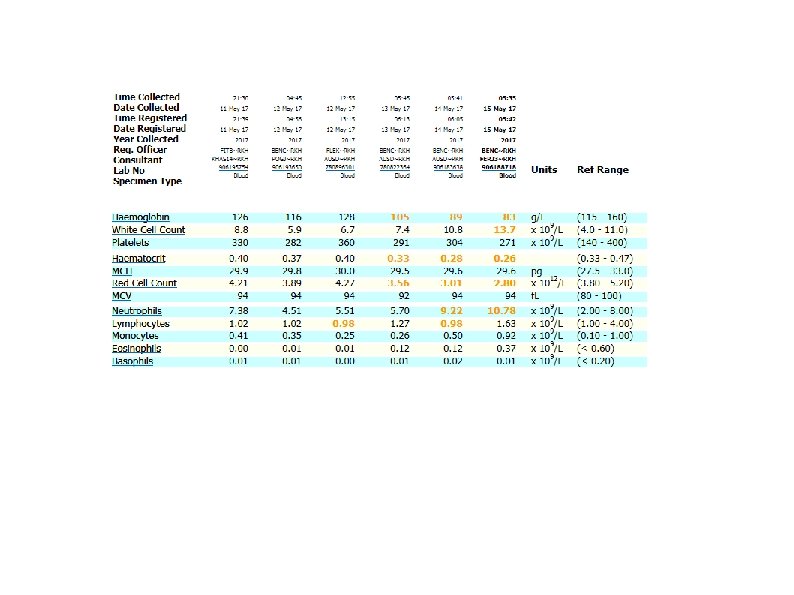
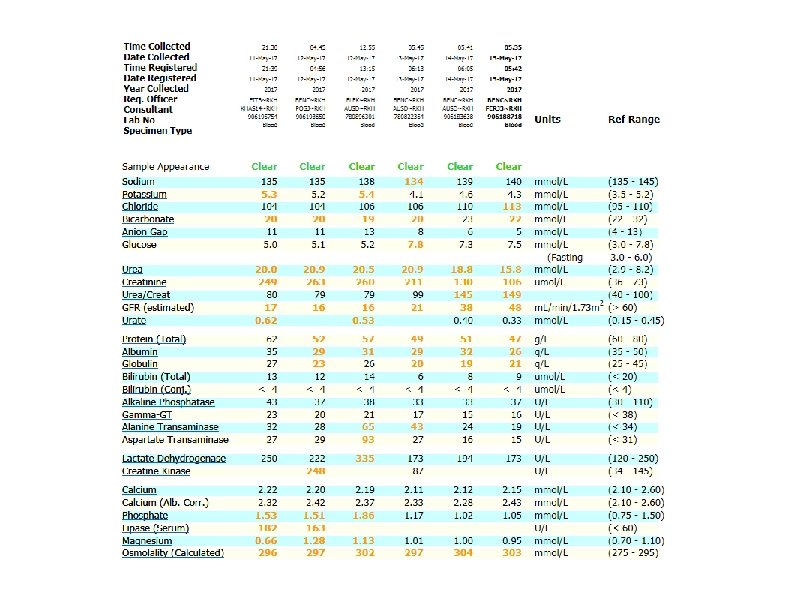
Chem 8: Cr 163, Ur 16. 7, Hb 160 CG 4: p. H 7. 19, PCO 2 62, HCO 3 23. 8 Lactate 2. 93 At NS request, treating clinician attended at 1600 hrs KC RK 336011

0100 hrs BP 128/87 HR 77 RR 20 0300 hrs BP 112/60 HR --- RR 18 0600 hrs BP 108/60 HR 60 RR 18 1000 hrs BP 99/64 HR 95 RR 18 1400 hrs BP 124/70 HR 114 RR 18 1515 hrs BP 138/74 HR 122 RR 18 1600 hrs BP 126/68 HR 102 RR 18 On O 2 1850 hrs BP ---- HR 93 RR 18 On O 2 KC RK 336011

KC RK 336011

Arrived at Hillcrest Sp. O 2 93% on 3 L via NP BP 93/60 HR 100 Ongoing pain Afebrile Referred to Rockhampton Hospital KC RK 336011

Dx with perforated ulcer and AKI Admitted HDU/ICU Laparoscopy + omental patch 12/05 Leak, laprarotomy and repatch 16/5 Washout of subphrenic collection 23/5 Trachy 25/5 for ongoing vent dependence Decannulated 6/6, to ward 7/6 KC RK 336011
: A failure of adequate oxygen delivery to tissue, most")
Shock (BMJ Best Practice): A failure of adequate oxygen delivery to tissue, most commonly recognized as hypotension with organ dysfunction Sepsis (Surviving Sepsis Campaign): Lifethreatening organ dysfunction caused by a dysregulated host response to infection Septic Shock (SSC): sepsis with circulatory and cellular/metabolic dysfunction Definitions

Best Practices

Recognition based on population, patterns, obs, clinical suspicion and at the same time commence treatment 30 m. L/kg IV crystalloid within first 3/24 Further fluids based on haemodynamics BP, HR, RR, T, Pa. O 2, UO, . . . Aim to normalize lactate through good resus http: //journals. lww. com/ccmjournal/Fulltext/2017/03000/Surviving_Sepsis_Campaign___International. 15. aspx Recognition and Resus

Two sets of blood cultures Does not have to coincide with fever Can be taken at same time (from different sites) B/C should not delay antibiotics Should be completed within 45 min Diagnosis

Broad spectrum Abx coverage within 1 hr of recognition and preferably sooner Can be given IO or IM if vascular access cannot be established Drug choice as per local guidelines Antibiotics

Surgical source control Target recommendation is 6 -12 hrs Removal and replacement of infected devices (IDCs, IVCs, CVCs) Source Control

Discussion & Questions
8ef3c3f15f44745ef270f40c3d2cff0e.ppt