

Urgent surgical diseases.ppt
- Количество слайдов: 56
 Lecture on pediatric surgery for the 5 -th year students of medical department Theme: «Urgent surgical diseases of the abdominal cavity in children» Prof. O. Fofanov
Lecture on pediatric surgery for the 5 -th year students of medical department Theme: «Urgent surgical diseases of the abdominal cavity in children» Prof. O. Fofanov
 Lecture structure: 1. Acquired Intestinal Obstruction. Bowel Intussusception. 2. Inflammatory Diseases of the Abdominal Cavity. Acute Appendicitis. 3. Gastrointestinal Bleeding. 4. Portal Hypertension. 5. Closed Abdominal Trauma. 2
Lecture structure: 1. Acquired Intestinal Obstruction. Bowel Intussusception. 2. Inflammatory Diseases of the Abdominal Cavity. Acute Appendicitis. 3. Gastrointestinal Bleeding. 4. Portal Hypertension. 5. Closed Abdominal Trauma. 2
 Based on morphofunctional features: I. Mechanical Strangulated Obturative") Classification of acquired intestinal obstruction 1) Based on morphofunctional features: I. Mechanical Strangulated Obturative Mixed Volvulus Internal type Intussusception Node formation External type Adhesive Pinching II. Dynamic intestinal obstruction Spastic Paralytic
Classification of acquired intestinal obstruction 1) Based on morphofunctional features: I. Mechanical Strangulated Obturative Mixed Volvulus Internal type Intussusception Node formation External type Adhesive Pinching II. Dynamic intestinal obstruction Spastic Paralytic
 By the level of obstruction: 1) small intestinal obstruction A) High B) Low") 2) By the level of obstruction: 1) small intestinal obstruction A) High B) Low 2) colon obstruction 3) Based on the course of disease: 1) acute 2) chronic 3) relapsing 4) The degree of obstruction: A) complete B) partial 4
2) By the level of obstruction: 1) small intestinal obstruction A) High B) Low 2) colon obstruction 3) Based on the course of disease: 1) acute 2) chronic 3) relapsing 4) The degree of obstruction: A) complete B) partial 4
 There are 3 stages of intestinal obstruction: 1 – interruption in the passage of intestinal contents 2 – intestinal disorders of bowel hemocirculation 3 - peritonitis
There are 3 stages of intestinal obstruction: 1 – interruption in the passage of intestinal contents 2 – intestinal disorders of bowel hemocirculation 3 - peritonitis
 Causes of dynamic bowel obstruction: Paralytic Some medications Infections of the abdominal cavity Mesenteric ischemia Complications of abdominal surgery Diseases of kidney and thoracic organs Hypokalemia Traumatic brain injury Pneumonia, sepsis, meningitis Spastic Ascariasis Hysteria Poisoning by heavy metal compounds 6
Causes of dynamic bowel obstruction: Paralytic Some medications Infections of the abdominal cavity Mesenteric ischemia Complications of abdominal surgery Diseases of kidney and thoracic organs Hypokalemia Traumatic brain injury Pneumonia, sepsis, meningitis Spastic Ascariasis Hysteria Poisoning by heavy metal compounds 6
") Causes of mechanical bowel obstruction: Obturative Tumors Lump of helminths Adhesive obstruction (plane reunions) Koprostasis Obturation by food masses Strangulated Volvulus of the intestine Pinched hernia Node formation Adhesive obstruction (like-cord reunions) Mixed Intussusception Adhesive obstruction 7
Causes of mechanical bowel obstruction: Obturative Tumors Lump of helminths Adhesive obstruction (plane reunions) Koprostasis Obturation by food masses Strangulated Volvulus of the intestine Pinched hernia Node formation Adhesive obstruction (like-cord reunions) Mixed Intussusception Adhesive obstruction 7
 Intussusception Immersion of one segment of bowel into another Frequency: 1 -4 from 1000 babies The majority (80 -90%) of cases is observed from 4 to 10 months The most often localization is in the region of the ileocecal angle (about 92 -94%)
Intussusception Immersion of one segment of bowel into another Frequency: 1 -4 from 1000 babies The majority (80 -90%) of cases is observed from 4 to 10 months The most often localization is in the region of the ileocecal angle (about 92 -94%)
 Hystory For the first time the disease was documented by Paul Barbet from Amsterdam in 1674. The first successful surgery on intussusception in a 2 -year child was performed by Jonathan Hitchynson in 1871. In 1871 Hirschsprung described conservative treatment of intussusception by applying hydrostatic pressure on the intestine.
Hystory For the first time the disease was documented by Paul Barbet from Amsterdam in 1674. The first successful surgery on intussusception in a 2 -year child was performed by Jonathan Hitchynson in 1871. In 1871 Hirschsprung described conservative treatment of intussusception by applying hydrostatic pressure on the intestine.
 Classification by H. I. Feldman: Small intestine intussusception - occurs in 3. 5% of patients. Large intestine intussusception - 2. 8% of patients. Ileocecal intussusception - 94% of patients. A) ileum-colon – immersion of ileum into ileum and then into the colon with frequency rate of about 41%-with strangulation prevailing. B) cecum-colon - cecum is involved in colon and iliac colon and appendix stretch for it - found in 53% of patients. Rare forms of intussusception: isolated intussusception of the appendix, retrograde intussusception and multiple. By the course of intussusception: acute, chronic and relapsing. By the structure: simple and complex
Classification by H. I. Feldman: Small intestine intussusception - occurs in 3. 5% of patients. Large intestine intussusception - 2. 8% of patients. Ileocecal intussusception - 94% of patients. A) ileum-colon – immersion of ileum into ileum and then into the colon with frequency rate of about 41%-with strangulation prevailing. B) cecum-colon - cecum is involved in colon and iliac colon and appendix stretch for it - found in 53% of patients. Rare forms of intussusception: isolated intussusception of the appendix, retrograde intussusception and multiple. By the course of intussusception: acute, chronic and relapsing. By the structure: simple and complex
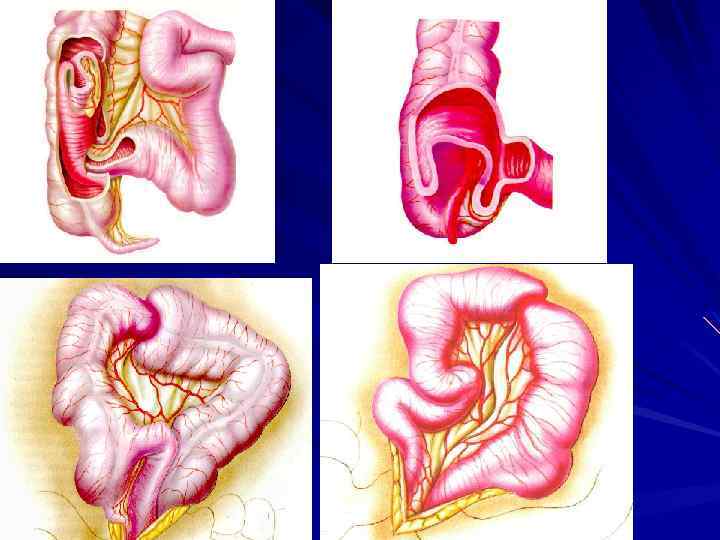
 mutual long mesentery") Aetiology and pathogenesis Anatomical and physiological features in infants: 1) mutual long mesentery of small and large intestine and therefore increased mobility of the intestine; 2) unequal development of the longitudinal and circular layers of muscles of the intestinal wall with a predominance of circulatory muscles 3) non-differentiated nervous apparatus of the intestine, non-coordinated peristalsis. Changing of the regime and the nature of feeding – gradual weaning (which occurs in 4 -5 months) and especially its improper administration. Some anatomical formations: Meckel`s diverticulum, polyps, tumors of intestinal wall, enlarged mesenteric lymph nodes, bowel wall hematoma (e. g. , disease Schonlein - Henoch), hyperplasia of Peyer patches and helminthes. Enterocolitis - due to a significant increase peristalsis.
Aetiology and pathogenesis Anatomical and physiological features in infants: 1) mutual long mesentery of small and large intestine and therefore increased mobility of the intestine; 2) unequal development of the longitudinal and circular layers of muscles of the intestinal wall with a predominance of circulatory muscles 3) non-differentiated nervous apparatus of the intestine, non-coordinated peristalsis. Changing of the regime and the nature of feeding – gradual weaning (which occurs in 4 -5 months) and especially its improper administration. Some anatomical formations: Meckel`s diverticulum, polyps, tumors of intestinal wall, enlarged mesenteric lymph nodes, bowel wall hematoma (e. g. , disease Schonlein - Henoch), hyperplasia of Peyer patches and helminthes. Enterocolitis - due to a significant increase peristalsis.
 Typical clinical picture : Sudden onset of the background full health; Strong pain with light intervals; Symptom "monkey" ("ladder"); Vomiting; Bloody discharge from the rectum (symptom "raspberry jelly"); Definition invaginate palpation; Symptom Dansye; Symptom "Obukhov Hospital“; Palpation of the intussusceptum.
Typical clinical picture : Sudden onset of the background full health; Strong pain with light intervals; Symptom "monkey" ("ladder"); Vomiting; Bloody discharge from the rectum (symptom "raspberry jelly"); Definition invaginate palpation; Symptom Dansye; Symptom "Obukhov Hospital“; Palpation of the intussusceptum.
 Diagnosis of intussusception Sonography : symptoms of "target“, "pseudo kidney" Colour Doppler : used to confirm the viability of the intestine and as a prognostic sign of the success of conservative treatment Pneumocolonography : symptoms of “shape of the sickle ”, “a crab claw ”, “bow”
Diagnosis of intussusception Sonography : symptoms of "target“, "pseudo kidney" Colour Doppler : used to confirm the viability of the intestine and as a prognostic sign of the success of conservative treatment Pneumocolonography : symptoms of “shape of the sickle ”, “a crab claw ”, “bow”
 ULTRASOUND. Ileocecal intussusception Symptom of "pseudo kidney"
ULTRASOUND. Ileocecal intussusception Symptom of "pseudo kidney"
 ULTRASOUND. Ileocecal intussusception symptom of "target"
ULTRASOUND. Ileocecal intussusception symptom of "target"
 X-ray examination
X-ray examination
 Pneumocolonography Air comes to the head of intussusceptum Intussusceptum shadow Symptom of the ``bow``.
Pneumocolonography Air comes to the head of intussusceptum Intussusceptum shadow Symptom of the ``bow``.
 X-ray symptoms: “shape of the sickle ” “a crab claw ”
X-ray symptoms: “shape of the sickle ” “a crab claw ”
 Conservative treatment: the method of throughout retrograde air insufflation suggested by Gritsenko
Conservative treatment: the method of throughout retrograde air insufflation suggested by Gritsenko
 Contraindications to conservative disinvagination : duration of the illness more than 24 hours; signs of peritonitis; recurrent intussusception; loss invaginate through the rectum; age of children - over 1 year.
Contraindications to conservative disinvagination : duration of the illness more than 24 hours; signs of peritonitis; recurrent intussusception; loss invaginate through the rectum; age of children - over 1 year.
 Surgical treatment
Surgical treatment
 Letality Adequate treatment – recovery after 24 h. Letality 1 -3%. Without treatment disease is fatal in 2 -5 days. Recurrent in 3 -11% cases, mainly after conservative treatment. Complications Intestinal bleeding Necrosis and perforation of the colon Sepsis, shock
Letality Adequate treatment – recovery after 24 h. Letality 1 -3%. Without treatment disease is fatal in 2 -5 days. Recurrent in 3 -11% cases, mainly after conservative treatment. Complications Intestinal bleeding Necrosis and perforation of the colon Sepsis, shock
 Acute appendicitis
Acute appendicitis
 Hystory In 1886, a Harvard pathologist Reginald Fitz described the inflammation of the appendix with perforation, its diagnosis and treatment. Fitz proposed the term "appendicitis". In 1887, Morton from Philadelphia conducted the first successful appendectomy for perforated appendix. Subsequently, the operation of appendicitis became quite common. In 1889, Charles Mc-Burnham described the place of greatest pain in acute appendicitis
Hystory In 1886, a Harvard pathologist Reginald Fitz described the inflammation of the appendix with perforation, its diagnosis and treatment. Fitz proposed the term "appendicitis". In 1887, Morton from Philadelphia conducted the first successful appendectomy for perforated appendix. Subsequently, the operation of appendicitis became quite common. In 1889, Charles Mc-Burnham described the place of greatest pain in acute appendicitis
 Appears") Clinical anatomy The average length of 10. 8 cm (range 2 -20 cm) Appears on the 5 -th month of gestation Bloodv supply: a. appendicularis (from a. ileocolica) Venous outflow: v. mesenterica superior Place ascent teniae coli helps to determine the base of the appendix
Clinical anatomy The average length of 10. 8 cm (range 2 -20 cm) Appears on the 5 -th month of gestation Bloodv supply: a. appendicularis (from a. ileocolica) Venous outflow: v. mesenterica superior Place ascent teniae coli helps to determine the base of the appendix
 Anatomical and physiological features Mobile ileocecal angle The high placement of the cecum Nerve plexus are embryonic in nature, their differentiation ends up to 14 years Newborn appendix has a conical shape with no clear boundary of the cecum. Appendiceal flap (flap Gerlach) are often absent Low plastic properties of the peritoneum High suction capacity of the peritoneum
Anatomical and physiological features Mobile ileocecal angle The high placement of the cecum Nerve plexus are embryonic in nature, their differentiation ends up to 14 years Newborn appendix has a conical shape with no clear boundary of the cecum. Appendiceal flap (flap Gerlach) are often absent Low plastic properties of the peritoneum High suction capacity of the peritoneum
 -High hydrophilicity of appendix tissue - Intensive blood flow in the appendix - Omentum majus in infants is short, thin and of little barrier capacity.
-High hydrophilicity of appendix tissue - Intensive blood flow in the appendix - Omentum majus in infants is short, thin and of little barrier capacity.
 Aetiology and pathogenesis. Infectious theory. Most important in the pathogenesis of appendicitis are: Bacteroides fragilis, Escherichia coli, Streptococcus, Pseudomonas, Klebsiella, Clostridium. Chance of hematogenous and lymphogenous pathways of infection. Mechanical factors: obstruction of the appendix lumen by fecal stones, worms, congenital anomalies of the appendix (torsion, bends, membranes). Nutritional factors (promotes the use of meat and fatty foods).
Aetiology and pathogenesis. Infectious theory. Most important in the pathogenesis of appendicitis are: Bacteroides fragilis, Escherichia coli, Streptococcus, Pseudomonas, Klebsiella, Clostridium. Chance of hematogenous and lymphogenous pathways of infection. Mechanical factors: obstruction of the appendix lumen by fecal stones, worms, congenital anomalies of the appendix (torsion, bends, membranes). Nutritional factors (promotes the use of meat and fatty foods).
. Simple (catarrhal) appendicitis Phlegmonous appendicitis Gangrenous appendicitis Perforative appendicitis") Clinical and morphological classification (Sprengel). Simple (catarrhal) appendicitis Phlegmonous appendicitis Gangrenous appendicitis Perforative appendicitis Appendicular infiltrate is often identified as a separate form. Infiltrated appendix, small bowel loops, omentum and cecum form a dense, painful conglomerate.
Clinical and morphological classification (Sprengel). Simple (catarrhal) appendicitis Phlegmonous appendicitis Gangrenous appendicitis Perforative appendicitis Appendicular infiltrate is often identified as a separate form. Infiltrated appendix, small bowel loops, omentum and cecum form a dense, painful conglomerate.
 appendicitis Appendix looks normal or slightly hyperemic and swollen. The serous membrane") Simple (catarrhal) appendicitis Appendix looks normal or slightly hyperemic and swollen. The serous membrane presents no exudate. The mucous membrane may covered with be focal hemorrhages and ulcerations.
Simple (catarrhal) appendicitis Appendix looks normal or slightly hyperemic and swollen. The serous membrane presents no exudate. The mucous membrane may covered with be focal hemorrhages and ulcerations.
 Phlegmonous appendicitis Appendix, is swollen, reddened, tense, thickened, compacted, sometimes covered with fibre-like depositions. Sometimes the appendix is inflated, fluctuations are observed, inside there may be some pus (empyema of the appendix). In the abdominal cavity serous, seropurulent or purulent exudate is found.
Phlegmonous appendicitis Appendix, is swollen, reddened, tense, thickened, compacted, sometimes covered with fibre-like depositions. Sometimes the appendix is inflated, fluctuations are observed, inside there may be some pus (empyema of the appendix). In the abdominal cavity serous, seropurulent or purulent exudate is found.
 Gangrenous appendicitis Is characterized by destructive changes of the entire wall of the appendix. Appendix is thickened, earthy-grey, with purulent and fibre-like depositions. Its wall is flabby and can be easily perforated. Parietal peritoneum is often altered: edematous, infiltrated, covered by fibrin.
Gangrenous appendicitis Is characterized by destructive changes of the entire wall of the appendix. Appendix is thickened, earthy-grey, with purulent and fibre-like depositions. Its wall is flabby and can be easily perforated. Parietal peritoneum is often altered: edematous, infiltrated, covered by fibrin.
 Perforative appendicitis The wall of the appendix is perforated in place of necrosis. Abdominal cavity contains purulent exudate with fecal odour. Perforation hole is often located near the top on the side opposite to mesentery where blood supply is scarce. Perforation of the appendix in young children causes widespread peritonitis. Parietal peritoneum is edematous, hyperemic, thickened and can be easily torn.
Perforative appendicitis The wall of the appendix is perforated in place of necrosis. Abdominal cavity contains purulent exudate with fecal odour. Perforation hole is often located near the top on the side opposite to mesentery where blood supply is scarce. Perforation of the appendix in young children causes widespread peritonitis. Parietal peritoneum is edematous, hyperemic, thickened and can be easily torn.
 Location of the appendix: Typical: point Mc. Burney (2/3 of the distance between the navel and spina iliaca anterior superior) Atypical localization: Retrocecal Pelvic Retroperitoneal Subhepatic Leftside
Location of the appendix: Typical: point Mc. Burney (2/3 of the distance between the navel and spina iliaca anterior superior) Atypical localization: Retrocecal Pelvic Retroperitoneal Subhepatic Leftside
 Pain in the periumbilical or") The classic clinical symptoms of appendicitis (in older children) Pain in the periumbilical or epigastric region, which moves in the right iliac area Nausea, vomiting (1 -2 fold), anorexia Delayed bowel movements or diarrhea Low-grade fever Symptom of "scissors" Palpation: Filatov symptom, passive muscle tension, Schetkin-Blumberg symptom Reducing of bowel noises Pain in the right side in rectal examination
The classic clinical symptoms of appendicitis (in older children) Pain in the periumbilical or epigastric region, which moves in the right iliac area Nausea, vomiting (1 -2 fold), anorexia Delayed bowel movements or diarrhea Low-grade fever Symptom of "scissors" Palpation: Filatov symptom, passive muscle tension, Schetkin-Blumberg symptom Reducing of bowel noises Pain in the right side in rectal examination
 Rectal digital examination Performed in all cases, the most informative is by pelvic placement process
Rectal digital examination Performed in all cases, the most informative is by pelvic placement process
 Features of clinic in infants Prevalence of common symptoms over the local; Worries of child, behavior change, anorexia; Febrile body temperature; Repeated vomiting, diarrhea; Bloating; Filatov Symptom, Shurynok symptom Tensions of anterior abdominal wall muscles expressed in all departments; Requires review in a dream
Features of clinic in infants Prevalence of common symptoms over the local; Worries of child, behavior change, anorexia; Febrile body temperature; Repeated vomiting, diarrhea; Bloating; Filatov Symptom, Shurynok symptom Tensions of anterior abdominal wall muscles expressed in all departments; Requires review in a dream
 Features of clinic in atypical placement of appendix Retroperitoneal - pain appeared in the right lumbar region, may radiate to the genitals or the course of the ureter, causing frequent and painful urination. The abdomen is involved in breathing, palpation soft, painless throughout, Schetkin symptom is negative. There is a positive Kocher symptom. Palpation in the right lumbar region marked tenderness, muscle tension, positive Pasternatsky symptom.
Features of clinic in atypical placement of appendix Retroperitoneal - pain appeared in the right lumbar region, may radiate to the genitals or the course of the ureter, causing frequent and painful urination. The abdomen is involved in breathing, palpation soft, painless throughout, Schetkin symptom is negative. There is a positive Kocher symptom. Palpation in the right lumbar region marked tenderness, muscle tension, positive Pasternatsky symptom.
 Pelvic - characterized by abdominal pain, above the pubis, which irradiate the course of the urethra, in the testis (right sexual lip), rectum. In patients there diarrhea or frequent painful urination. Palpation abdominal pain and muscle tension showing above the pubis. Great help in the diagnosis gives digital rectal examination, which show a sharp pain, sagging or infiltrate into the pelvis. In the urine sample is often defined proteins, leukocytes, epithelium, erythrocytes.
Pelvic - characterized by abdominal pain, above the pubis, which irradiate the course of the urethra, in the testis (right sexual lip), rectum. In patients there diarrhea or frequent painful urination. Palpation abdominal pain and muscle tension showing above the pubis. Great help in the diagnosis gives digital rectal examination, which show a sharp pain, sagging or infiltrate into the pelvis. In the urine sample is often defined proteins, leukocytes, epithelium, erythrocytes.
 Subhepatic - the clinical picture resembles a destructive cholecystitis: repeated vomiting, pain in the right pidrebir'yi, local pain and muscle tension here, positive symptom Ortner. Sometimes there is a mild hysteria skin. The lower abdomen is painful, soft on palpation. Leftside - caused by mobile cecum, incomplete rotation "midgut" reverse arrangement of internal organs. Clinical manifestations localized left. Retrocecal - severe intoxication with mild local symptoms. Local pain and muscle tension of the abdominal wall is much less pronounced. Later, there are peritoneal signs.
Subhepatic - the clinical picture resembles a destructive cholecystitis: repeated vomiting, pain in the right pidrebir'yi, local pain and muscle tension here, positive symptom Ortner. Sometimes there is a mild hysteria skin. The lower abdomen is painful, soft on palpation. Leftside - caused by mobile cecum, incomplete rotation "midgut" reverse arrangement of internal organs. Clinical manifestations localized left. Retrocecal - severe intoxication with mild local symptoms. Local pain and muscle tension of the abdominal wall is much less pronounced. Later, there are peritoneal signs.
 and leukocyte shift") Additional methods of research Blood tests: leukocytosis (15 to 20 thousand) and leukocyte shift to the left (to the young forms and myelocytes) Urinalysis Thermometry aksillaris and rectal: the difference is more than 0. 6 ° C Ultrasound: The diameter of the appendix over 6 mm; Infiltration of the appendix wall; absence of peristalsis; presence of free fluid around appendix Laparoscopy
Additional methods of research Blood tests: leukocytosis (15 to 20 thousand) and leukocyte shift to the left (to the young forms and myelocytes) Urinalysis Thermometry aksillaris and rectal: the difference is more than 0. 6 ° C Ultrasound: The diameter of the appendix over 6 mm; Infiltration of the appendix wall; absence of peristalsis; presence of free fluid around appendix Laparoscopy
 Differential diagnosis Inflammatory and infectious diseases: acute nonspecific mesadenitis, acute respiratory tract infection, pneumonia, acute otitis; intestinal infection, pseudotuberculosis, acute hepatitis, children's infectious diseases (measles, scarlet fever, chickenpox, mumps) Surgical diseases of the abdominal cavity: coprostasis, functional spastic ileus (intestinal colic), obstructive ileus, intussusception, acute cholecystitis, peptic ulcer, acute pancreatitis, abdominal tumors, Crohn's disease, incomplete turning of "midgut“ Urologic Diseases: urolithiasis; nephroptosis, hydronephrosis, acute pyelonephritis, acute cystitis Gynecological diseases: primary pelviperitonitis; premenstrual cramps; hematokolpos, hematosalpinx; apoplexy of ovary, ovarian cysts Systemic diseases: rheumatic fever, hemorrhagic vasculitis, diabetes.
Differential diagnosis Inflammatory and infectious diseases: acute nonspecific mesadenitis, acute respiratory tract infection, pneumonia, acute otitis; intestinal infection, pseudotuberculosis, acute hepatitis, children's infectious diseases (measles, scarlet fever, chickenpox, mumps) Surgical diseases of the abdominal cavity: coprostasis, functional spastic ileus (intestinal colic), obstructive ileus, intussusception, acute cholecystitis, peptic ulcer, acute pancreatitis, abdominal tumors, Crohn's disease, incomplete turning of "midgut“ Urologic Diseases: urolithiasis; nephroptosis, hydronephrosis, acute pyelonephritis, acute cystitis Gynecological diseases: primary pelviperitonitis; premenstrual cramps; hematokolpos, hematosalpinx; apoplexy of ovary, ovarian cysts Systemic diseases: rheumatic fever, hemorrhagic vasculitis, diabetes.
 Treatment of appendicitis: "Open" or laparoscopic appendectomy
Treatment of appendicitis: "Open" or laparoscopic appendectomy
 Complications of acute appendicitis Complications of abdominal cavity: Preoperative complications: peritonitis, periappendicular abscess. Postoperative complications : adhesive intestinal obstruction, paralytic ileus, failure appendix stump, postoperative peritonitis, intestinal fistula, postoperative infiltrates and abscesses of the abdominal cavity. Complications during surgery: bleeding, perforation of the intestine.
Complications of acute appendicitis Complications of abdominal cavity: Preoperative complications: peritonitis, periappendicular abscess. Postoperative complications : adhesive intestinal obstruction, paralytic ileus, failure appendix stump, postoperative peritonitis, intestinal fistula, postoperative infiltrates and abscesses of the abdominal cavity. Complications during surgery: bleeding, perforation of the intestine.
 Complications of acute appendicitis Complications of wounds: bleeding, suppuration, infiltration, fistula, failure of stitches, bowel eventration, ventral hernia, kelloid scars. Complications of other organs and systems: pneumonia, sepsis, liver failure, renal failure, cerebral edema, toxic encephalopathy.
Complications of acute appendicitis Complications of wounds: bleeding, suppuration, infiltration, fistula, failure of stitches, bowel eventration, ventral hernia, kelloid scars. Complications of other organs and systems: pneumonia, sepsis, liver failure, renal failure, cerebral edema, toxic encephalopathy.
 Diseases which can cause bleeding from the digestive tract: I Somatic and infectious diseases: salmonellosis, dysentery, hemorrhagic diathesis, acute leukemia, intestinal parasites, metabolic reticulosis, lymphogranulomatosis, intestinal sepsis. II Borderline disorders: peptic ulcer and duodenal ulcer, ulcerative colitis, thrombocytopenia, coagulopathy of newborns, Turner syndrome, typhoid fever, regional enteritis.
Diseases which can cause bleeding from the digestive tract: I Somatic and infectious diseases: salmonellosis, dysentery, hemorrhagic diathesis, acute leukemia, intestinal parasites, metabolic reticulosis, lymphogranulomatosis, intestinal sepsis. II Borderline disorders: peptic ulcer and duodenal ulcer, ulcerative colitis, thrombocytopenia, coagulopathy of newborns, Turner syndrome, typhoid fever, regional enteritis.
 Diseases which can cause bleeding from the digestive tract: III Surgical diseases: varicose veins of the esophagus and stomach cardia, hernia of esophageal aperture of diaphragm, intussusception, Meckel`s diverticulum, intestinal duplication, Peytts. Yehers syndrome, intestinal tumors, colon and rectal polyps, fissures of anal ring, varicose hemorrhoidal veins.
Diseases which can cause bleeding from the digestive tract: III Surgical diseases: varicose veins of the esophagus and stomach cardia, hernia of esophageal aperture of diaphragm, intussusception, Meckel`s diverticulum, intestinal duplication, Peytts. Yehers syndrome, intestinal tumors, colon and rectal polyps, fissures of anal ring, varicose hemorrhoidal veins.
 There is a link between age of children and pathological processes In newborns - coagulopathy of newborns In infants - hernia of the esophageal aperture of diaphragm, intussusception, intestinal duplication, Meckel diverticulum ulcer In children 3 -7 years - esophageal varices due to portal hypertension, colon polyps, fissures of anal ring In children 10 -14 years - peptic stomach and duodenal ulcer, gastrointestinal polyps, hemorrhoids varicose veins, intestinal tumors (lymphoma, hemangioma)
There is a link between age of children and pathological processes In newborns - coagulopathy of newborns In infants - hernia of the esophageal aperture of diaphragm, intussusception, intestinal duplication, Meckel diverticulum ulcer In children 3 -7 years - esophageal varices due to portal hypertension, colon polyps, fissures of anal ring In children 10 -14 years - peptic stomach and duodenal ulcer, gastrointestinal polyps, hemorrhoids varicose veins, intestinal tumors (lymphoma, hemangioma)
 - congenital stenosis of the portal") Portal hypertension Classification Prehepatic block (80% in children) - congenital stenosis of the portal vein, portal vein thrombosis, compression of the portal vein by scars, infiltrates Intrahepatic block (1 -3% in children) - cirrhosis, intrahepatic arteriovenous anastomoses Posthepatic block - hepatic vein phlebitis (syndrome Budd-Chiari) Mixed (15 -20% in children) - pre-and intrahepatic block
Portal hypertension Classification Prehepatic block (80% in children) - congenital stenosis of the portal vein, portal vein thrombosis, compression of the portal vein by scars, infiltrates Intrahepatic block (1 -3% in children) - cirrhosis, intrahepatic arteriovenous anastomoses Posthepatic block - hepatic vein phlebitis (syndrome Budd-Chiari) Mixed (15 -20% in children) - pre-and intrahepatic block
 Symptoms of portal hypertension bleeding Vomiting blood, often as "a coffee grounds", rapidly progressing hemorrhagic shock After 6 -8 hours a resin-like stool is present Common symptoms of blood loss (pale skin, hypotension, tachycardia, weakness, systolic murmur over the apex of the heart) Enlarged spleen Sometimes ascitis
Symptoms of portal hypertension bleeding Vomiting blood, often as "a coffee grounds", rapidly progressing hemorrhagic shock After 6 -8 hours a resin-like stool is present Common symptoms of blood loss (pale skin, hypotension, tachycardia, weakness, systolic murmur over the apex of the heart) Enlarged spleen Sometimes ascitis
 Diagnosis of portal hypertension bleeding General analysis of blood - signs of anemia (decreased hematocrit, hemoglobin, erythrocyte count) Ultrasound examination reveals "cavity" in the area of portal vein, slow and sometimes reverse flow. In case of liver cirrhosis the structure of the liver is changed. Enlarged spleen Fibrogastroscopy shows varicose veins of the esophagus and stomach cardia
Diagnosis of portal hypertension bleeding General analysis of blood - signs of anemia (decreased hematocrit, hemoglobin, erythrocyte count) Ultrasound examination reveals "cavity" in the area of portal vein, slow and sometimes reverse flow. In case of liver cirrhosis the structure of the liver is changed. Enlarged spleen Fibrogastroscopy shows varicose veins of the esophagus and stomach cardia
 Treatment of portal hypertension bleeding Conservative measures: bed rest, cold - locally, medication hemostatic agents (cryoprecipitate, etamzylat, vikasol, calcium chloride, aminocaproic acid, fresh frozen plasma, sandostatin), replacement therapy. Probe - stoppers Blackmore. Endoscopic sclerotherapy or klipsing veins of the esophagus. Surgery - gastrotomy, suturing veins.
Treatment of portal hypertension bleeding Conservative measures: bed rest, cold - locally, medication hemostatic agents (cryoprecipitate, etamzylat, vikasol, calcium chloride, aminocaproic acid, fresh frozen plasma, sandostatin), replacement therapy. Probe - stoppers Blackmore. Endoscopic sclerotherapy or klipsing veins of the esophagus. Surgery - gastrotomy, suturing veins.
 Traumatic injury of the abdomen Among all types of damage abdominal trauma is 20%. They cause disorders of vital functions and high mortality ( 22%) Damage to the abdominal cavity leads to posttraumatic peritonitis. 75% of patients with traumatic injury of the abdomen develop signs of post-traumatic shock. Closed abdominal trauma injuries are divided into the trauma of hollow and parenchymatous organs
Traumatic injury of the abdomen Among all types of damage abdominal trauma is 20%. They cause disorders of vital functions and high mortality ( 22%) Damage to the abdominal cavity leads to posttraumatic peritonitis. 75% of patients with traumatic injury of the abdomen develop signs of post-traumatic shock. Closed abdominal trauma injuries are divided into the trauma of hollow and parenchymatous organs
 Symptom "sickle"
Symptom "sickle"
 Thank you! 56
Thank you! 56