

b82ce4b3b6afe59fcc31e97f6b98d8a6.ppt
- Количество слайдов: 30
 Leading System Change MMA: Launching High Impact Health Care Teams Virginia Mohl, MD, Ph. D, DIO and Medical Director Health Care, Education and Research www. billingsclinic. com
Leading System Change MMA: Launching High Impact Health Care Teams Virginia Mohl, MD, Ph. D, DIO and Medical Director Health Care, Education and Research www. billingsclinic. com
 Objectives 1. Understand why we need Physician Leaders capable of System-level leadership. 2. Start to identify new tools for facilitating change at the system level. 3. Identify key issues in building teams who work in systems and implications for Health Care workforce development.
Objectives 1. Understand why we need Physician Leaders capable of System-level leadership. 2. Start to identify new tools for facilitating change at the system level. 3. Identify key issues in building teams who work in systems and implications for Health Care workforce development.
 Outline 1. Introduction: 1. Why physician leadership? 2. What new competencies are needed? 3. How to think at the system level? 2. One organization’s Journey 1. Methicillin-Resistant Staph aureus 2. Hypertension 3. Referral Communication 4. Medical Education 3. Summary and questions
Outline 1. Introduction: 1. Why physician leadership? 2. What new competencies are needed? 3. How to think at the system level? 2. One organization’s Journey 1. Methicillin-Resistant Staph aureus 2. Hypertension 3. Referral Communication 4. Medical Education 3. Summary and questions
 System Thinking 1. 2. 3. 4. Who am I and how do I think? What is my culture and how resilient is it? What are the outside forces? Where do we want to be in 5 years? What can I do now to create my preferred future?
System Thinking 1. 2. 3. 4. Who am I and how do I think? What is my culture and how resilient is it? What are the outside forces? Where do we want to be in 5 years? What can I do now to create my preferred future?
 Why? Because Wicked Problems in Healthcare not solved by traditional problem solving
Why? Because Wicked Problems in Healthcare not solved by traditional problem solving
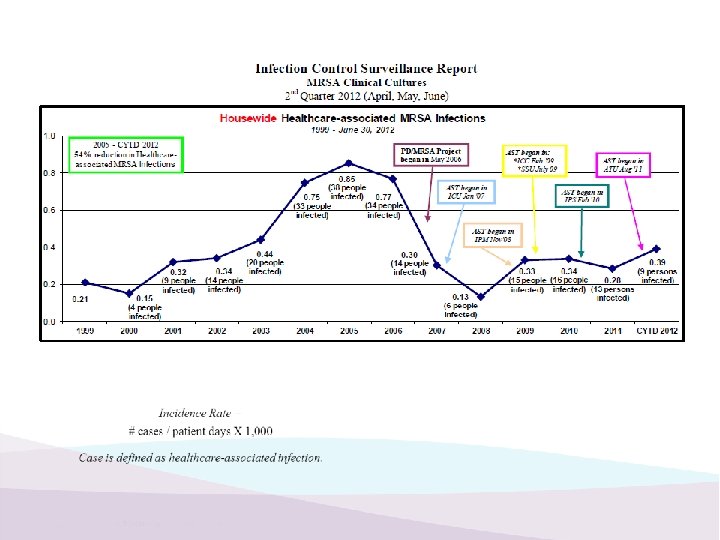
") Example 1: Adaptive change, Inpatient Eliminating the Transmission of Methicillin Resistant Staph aureus (MRSA) by Using the Positive Deviance (PD) Approach to Behavior and Social Change
Example 1: Adaptive change, Inpatient Eliminating the Transmission of Methicillin Resistant Staph aureus (MRSA) by Using the Positive Deviance (PD) Approach to Behavior and Social Change
 Key Interventions ~ The “Science” Bundle Ø Hand hygiene Ø Decontamination of the environment and equipment Ø Active surveillance cultures (ASCs) Ø Contact precautions (isolation) for infected and colonized patients
Key Interventions ~ The “Science” Bundle Ø Hand hygiene Ø Decontamination of the environment and equipment Ø Active surveillance cultures (ASCs) Ø Contact precautions (isolation) for infected and colonized patients
 WHAT IS POSITIVE DEVIANCE? A TOOL FOR LEADERS Solutions before our very eyes The Premise: In every community there are certain individuals whose uncommon practices/behaviors enable them to find better solutions to problems than their neighbors who have access to the same resources
WHAT IS POSITIVE DEVIANCE? A TOOL FOR LEADERS Solutions before our very eyes The Premise: In every community there are certain individuals whose uncommon practices/behaviors enable them to find better solutions to problems than their neighbors who have access to the same resources
 Theatre In the Round A diverse audience, from many units across the clinic, assembles in the conference room… now an inpatient medical room. For the next 60 minutes, no one knows what to expect.
Theatre In the Round A diverse audience, from many units across the clinic, assembles in the conference room… now an inpatient medical room. For the next 60 minutes, no one knows what to expect.
 The “Cultural” Bundle • Make the invisible, visible ~ chocolate pudding to simulate contamination ~ • Reinforce with Feedback • Solutions that are co-created and owned ~ ownership vs. buy-in ~ discovery & action dialogues • Act your way to a new way of thinking ~ create experiences that allow self-discovery
The “Cultural” Bundle • Make the invisible, visible ~ chocolate pudding to simulate contamination ~ • Reinforce with Feedback • Solutions that are co-created and owned ~ ownership vs. buy-in ~ discovery & action dialogues • Act your way to a new way of thinking ~ create experiences that allow self-discovery
 Example 2 : Population Health, Outpatient Improving the Management of Hypertension Using a Positive Deviance Approach
Example 2 : Population Health, Outpatient Improving the Management of Hypertension Using a Positive Deviance Approach
 PD’s Discovery & Action Dialogues • How do you know whether your patient has hypertension? • In your own practices, how do you know you have an accurate BP? • What prevents you from doing this all the time? • In your own practices, how do you decide when to treat? What prevents you from doing this all the time? • Is there anyone who has a way that helps them overcome these barriers? (the positive deviants) • Do you have any ideas? How can we apply? Amplify? • What can we do now? Any volunteers?
PD’s Discovery & Action Dialogues • How do you know whether your patient has hypertension? • In your own practices, how do you know you have an accurate BP? • What prevents you from doing this all the time? • In your own practices, how do you decide when to treat? What prevents you from doing this all the time? • Is there anyone who has a way that helps them overcome these barriers? (the positive deviants) • Do you have any ideas? How can we apply? Amplify? • What can we do now? Any volunteers?
 Results
Results
 Example 3: Regional Quality/Safety Improving the communication between referring and receiving Clinicians using Operational Excellence
Example 3: Regional Quality/Safety Improving the communication between referring and receiving Clinicians using Operational Excellence
 Operational Excellence: Lean and Six Sigma Billings Clinic Referral Communication Improvement Plan
Operational Excellence: Lean and Six Sigma Billings Clinic Referral Communication Improvement Plan
 Diagram The fishbone diagram helped the team to identify the") Cause & Effect (Fishbone) Diagram The fishbone diagram helped the team to identify the key inputs that lead to dissatisfaction with the current process for both referring and receiving providers.
Cause & Effect (Fishbone) Diagram The fishbone diagram helped the team to identify the key inputs that lead to dissatisfaction with the current process for both referring and receiving providers.
 The Team
The Team
 Need Both Technical Science Bundle Adaptive Cultural Bundle
Need Both Technical Science Bundle Adaptive Cultural Bundle
 Verify - Transfer & Clinic Referral Data The top chart shows the number of transfers from outside Yellowstone County pre and post the Kaizen event in June 2012. The increase in average monthly transfers from outside Yellowstone county is approximately 13%. Statistically this increase is significant. The bottom chart shows the number of clinic appts. from outside Yellowstone County pre and post the Kaizen event in June 2012. This shows a decrease of approximately 1. 5%; however, this change in appts. is not statistically significant and thus we would conclude that there has been no change.
Verify - Transfer & Clinic Referral Data The top chart shows the number of transfers from outside Yellowstone County pre and post the Kaizen event in June 2012. The increase in average monthly transfers from outside Yellowstone county is approximately 13%. Statistically this increase is significant. The bottom chart shows the number of clinic appts. from outside Yellowstone County pre and post the Kaizen event in June 2012. This shows a decrease of approximately 1. 5%; however, this change in appts. is not statistically significant and thus we would conclude that there has been no change.
 Example 3: National Medical Education Becoming an Independent Academic Medical Center
Example 3: National Medical Education Becoming an Independent Academic Medical Center
 What are the key forces driving Medical Education? 2016 estimate 44, 000
What are the key forces driving Medical Education? 2016 estimate 44, 000
 UGME Medical Student Rotations 2009 to Current 248% increase since 2009
UGME Medical Student Rotations 2009 to Current 248% increase since 2009
 15% solution Medical Education Month January 2016
15% solution Medical Education Month January 2016
 – Internal Medicine Residency –") Office of Medical Education • Graduate Medical Education (GME) – Internal Medicine Residency – Family Medicine Residency – Exploring/preparing for Psychiatric Residency and 4 th year General Surgery • Undergraduate Medical Education (UGME) – Medical Students – Nurse Practitioners – Physician Assistants • Continuing Medical Education (CME) – Conferences – Lecture series – Case conferences
Office of Medical Education • Graduate Medical Education (GME) – Internal Medicine Residency – Family Medicine Residency – Exploring/preparing for Psychiatric Residency and 4 th year General Surgery • Undergraduate Medical Education (UGME) – Medical Students – Nurse Practitioners – Physician Assistants • Continuing Medical Education (CME) – Conferences – Lecture series – Case conferences

 System Leadership is Different • Co-creation of desired future, one conversation at a time • Align change initiatives with stakeholders’ needs and values • Help others tolerate fears and losses that accompany change • Pay attention to environment • Courage, honesty, respect for others
System Leadership is Different • Co-creation of desired future, one conversation at a time • Align change initiatives with stakeholders’ needs and values • Help others tolerate fears and losses that accompany change • Pay attention to environment • Courage, honesty, respect for others
 A different model
A different model
 From Teamwork to Team of Teams: Thank you! Primary Care Team Administrative Team
From Teamwork to Team of Teams: Thank you! Primary Care Team Administrative Team
 You Must Learn to EMBRACE failure.
You Must Learn to EMBRACE failure.