db076555b4b69d7331952801d7f5ebdd.ppt
- Количество слайдов: 75
 Laws and Rules Related to CNM practice in Ohio Jeanne Bauer, CNM, MSN February 7, 2016
Laws and Rules Related to CNM practice in Ohio Jeanne Bauer, CNM, MSN February 7, 2016
 AKA: How to avoid a midwife crisis
AKA: How to avoid a midwife crisis
 Mission is to safeguard public health Issues, renews, revokes") Ohio Board of Nursing (BON) Mission is to safeguard public health Issues, renews, revokes licenses Enforces law/rules regulating nursing practice Assures basic requirements for practice are met
Ohio Board of Nursing (BON) Mission is to safeguard public health Issues, renews, revokes licenses Enforces law/rules regulating nursing practice Assures basic requirements for practice are met
 Ohio APRN statistics 13, 847 RNs with Certificate of Authority 2, 884 CRNA 351 CNM 9, 302 CNP 1, 509 CNS 7, 645 with Certificate to Prescribe 1, 698 with Ct. PExternship
Ohio APRN statistics 13, 847 RNs with Certificate of Authority 2, 884 CRNA 351 CNM 9, 302 CNP 1, 509 CNS 7, 645 with Certificate to Prescribe 1, 698 with Ct. PExternship
 Includes") Where can I find Ohio’s Laws on Nursing Practice? ORC (Ohio Revised Code) Includes all Ohio laws Enacted by the Ohio legislature Nurse Practice Act - section 4723 OAC (Ohio Administrative Code) Rules that define the law Written by the regulatory boards (like BON) Must be consistent with the law Typically more specific than the law
Where can I find Ohio’s Laws on Nursing Practice? ORC (Ohio Revised Code) Includes all Ohio laws Enacted by the Ohio legislature Nurse Practice Act - section 4723 OAC (Ohio Administrative Code) Rules that define the law Written by the regulatory boards (like BON) Must be consistent with the law Typically more specific than the law
 How Do I Find the Laws and Rules Pertaining to APRNs? Ohio Board of Nursing Home Page ohio. nursing. gov Ohio Law ORC Chapter 4723 (“Nurse Practice Act”) Administrative Rules Chapter 4723 -8: Certification, Registration of Nurse. Midwife and Other Specialties Chapter 4723 -9: Course of Study in Advanced Pharmacology
How Do I Find the Laws and Rules Pertaining to APRNs? Ohio Board of Nursing Home Page ohio. nursing. gov Ohio Law ORC Chapter 4723 (“Nurse Practice Act”) Administrative Rules Chapter 4723 -8: Certification, Registration of Nurse. Midwife and Other Specialties Chapter 4723 -9: Course of Study in Advanced Pharmacology
 Current") Which licenses does an APRN need to practice in Ohio? Registered Nurse (RN) Current National Specialty Certification (CNP, CNS, CNM, CRNA) Certificate of Authority (COA)
Which licenses does an APRN need to practice in Ohio? Registered Nurse (RN) Current National Specialty Certification (CNP, CNS, CNM, CRNA) Certificate of Authority (COA)
 Continuing Education Requirements 24 contact hours for RN Includes 1 Category A contact hour r/t Nurse Practice Act Future: Cultural Competency 12 hours for COA Can apply the same CE hours used for specialty certification Renew by October 31 of odd years (new)
Continuing Education Requirements 24 contact hours for RN Includes 1 Category A contact hour r/t Nurse Practice Act Future: Cultural Competency 12 hours for COA Can apply the same CE hours used for specialty certification Renew by October 31 of odd years (new)
 Specialty Certification Your COA is only valid if your national specialty certification is current The BON requires Primary Source Verification of current specialty certification Practicing on a lapsed (or inactive) COA is a criminal offense
Specialty Certification Your COA is only valid if your national specialty certification is current The BON requires Primary Source Verification of current specialty certification Practicing on a lapsed (or inactive) COA is a criminal offense
 5 -year certification cycle: Complete 3 AMCB modules AP,") American Midwifery Certification Board (AMCB) 5 -year certification cycle: Complete 3 AMCB modules AP, primary care of pregnant women IP, PP, NB Gyn, primary care of well-women 20 hours of CE Approved by ACNM or ACCME
American Midwifery Certification Board (AMCB) 5 -year certification cycle: Complete 3 AMCB modules AP, primary care of pregnant women IP, PP, NB Gyn, primary care of well-women 20 hours of CE Approved by ACNM or ACCME
 annual maintenance fee: $55 5") AMCB National Certification Exam: $500 Certificate Maintenance Program (CMP) annual maintenance fee: $55 5 -year pre-pay option: $247. 50 CMP article set: $65 Primary verification letter: $35
AMCB National Certification Exam: $500 Certificate Maintenance Program (CMP) annual maintenance fee: $55 5 -year pre-pay option: $247. 50 CMP article set: $65 Primary verification letter: $35
 National Certification Council Three-year certification cycle Complete a specialty assessment Obtain individualized education plan Earn CE based on your IEP Maintenance fee: $100 Reduced if CE purchased through NCC
National Certification Council Three-year certification cycle Complete a specialty assessment Obtain individualized education plan Earn CE based on your IEP Maintenance fee: $100 Reduced if CE purchased through NCC
 What is title protection? Use of the professional title restricted to individuals who have achieved specific requirements. Only formally trained and licensed individuals may use a protected title No title protection in Ohio law for midwives who are not CNMs
What is title protection? Use of the professional title restricted to individuals who have achieved specific requirements. Only formally trained and licensed individuals may use a protected title No title protection in Ohio law for midwives who are not CNMs
 What is physician / APRN collaboration? Physician / APRN relationship is specified in Ohio law APRN has independent practice within his/her scope Consult / collaborate as needed Notify the BON within thirty days of the identity of collaborating physician(s) and any changes in collaborators apn@nursing. ohio. gov
What is physician / APRN collaboration? Physician / APRN relationship is specified in Ohio law APRN has independent practice within his/her scope Consult / collaborate as needed Notify the BON within thirty days of the identity of collaborating physician(s) and any changes in collaborators apn@nursing. ohio. gov
 Direct physician supervision? For CRNAs: Directly supervised while administering anesthesia For other APRNs: Only during 500 of the 1500 supervised hours of prescribing functions during externship (CTP-E) Law does not require supervision in any other situation Hospital policy may require CNM supervision at births
Direct physician supervision? For CRNAs: Directly supervised while administering anesthesia For other APRNs: Only during 500 of the 1500 supervised hours of prescribing functions during externship (CTP-E) Law does not require supervision in any other situation Hospital policy may require CNM supervision at births
 Physician must be “available “ In person Or by telecommunications No “on site” requirement in ORC Need a plan for emergency coverage if regular collaborator is away (in SCA)
Physician must be “available “ In person Or by telecommunications No “on site” requirement in ORC Need a plan for emergency coverage if regular collaborator is away (in SCA)
 Physician co-signature Ohio law does not require collaborating physicians to co-sign charts or orders However, your employing agency may have a policy requiring physician co-signatures
Physician co-signature Ohio law does not require collaborating physicians to co-sign charts or orders However, your employing agency may have a policy requiring physician co-signatures
 What is Scope of Practice? Parameters of professional performance, responsibility, accountability In ORC, the parameters for each APRN group are consistent with national certifying organizations No “laundry list” in Ohio law
What is Scope of Practice? Parameters of professional performance, responsibility, accountability In ORC, the parameters for each APRN group are consistent with national certifying organizations No “laundry list” in Ohio law
 Is this in my scope of practice? Is the procedure consistent with Ohio law? Is it consistent with practice guidelines of your national certifying body? Do you have the knowledge, skills and clinical competence to perform this procedure safely and to respond appropriately to complications? Is this an accepted standard of care? Would a reasonable, prudent APRN perform this activity? If YES to all: this is within your scope of practice!
Is this in my scope of practice? Is the procedure consistent with Ohio law? Is it consistent with practice guidelines of your national certifying body? Do you have the knowledge, skills and clinical competence to perform this procedure safely and to respond appropriately to complications? Is this an accepted standard of care? Would a reasonable, prudent APRN perform this activity? If YES to all: this is within your scope of practice!
 CNP Scope “…may provide preventive and primary care services, provide services for acute illnesses, and evaluate and promote patient wellness within the nurse’s nursing specialty, consistent with the nurse’s education and certification…”
CNP Scope “…may provide preventive and primary care services, provide services for acute illnesses, and evaluate and promote patient wellness within the nurse’s nursing specialty, consistent with the nurse’s education and certification…”
 CNM Scope “…may provide the management of preventive services and those primary care services necessary to provide health care to women antepartally, intrapartally, postpartally, and gynecologically…”
CNM Scope “…may provide the management of preventive services and those primary care services necessary to provide health care to women antepartally, intrapartally, postpartally, and gynecologically…”
 CNM Prohibition “No certified nurse-midwife may perform version, deliver breech or face presentation, use forceps, do any obstetric operation, or treat any other abnormal condition, except in emergencies. ” No other APRN group has prohibitions written in law
CNM Prohibition “No certified nurse-midwife may perform version, deliver breech or face presentation, use forceps, do any obstetric operation, or treat any other abnormal condition, except in emergencies. ” No other APRN group has prohibitions written in law
 CNM Scope “…may provide the management of preventive services and those primary care services necessary to provide health care to women antepartally, intrapartally, postpartally, and gynecologically…”
CNM Scope “…may provide the management of preventive services and those primary care services necessary to provide health care to women antepartally, intrapartally, postpartally, and gynecologically…”
 Finally… Expedited Partner Therapy! AKA HB 124
Finally… Expedited Partner Therapy! AKA HB 124
 Expedited Partner Therapy Precedent-setting Permits CNMs to provide care to males Changes Nursing/Medical/Pharmacy law Required interprofessional collaboration to pass law
Expedited Partner Therapy Precedent-setting Permits CNMs to provide care to males Changes Nursing/Medical/Pharmacy law Required interprofessional collaboration to pass law
 EPT Effective February 20 Chlamydia, Gonorrhea, Trichomonas Limited to two sexual partners of your patient Partner(s) unable or unlikely to seek treatment Name and address if available, “EPT” Grants immunity to prescriber/pharmacist acting in good faith Summary to come in next Momentum
EPT Effective February 20 Chlamydia, Gonorrhea, Trichomonas Limited to two sexual partners of your patient Partner(s) unable or unlikely to seek treatment Name and address if available, “EPT” Grants immunity to prescriber/pharmacist acting in good faith Summary to come in next Momentum
 More Legislative Successes
More Legislative Successes
 Hospital Admitting Bill – effective 2014 Patients could previously be admitted to hospital only by doctors, dentists, podiatrists HB 139 added APRNs/PAs
Hospital Admitting Bill – effective 2014 Patients could previously be admitted to hospital only by doctors, dentists, podiatrists HB 139 added APRNs/PAs
 Hospital Admitting Bill – effective 2014 Must be credentialed by the hospital to admit Have a collaborative arrangement with physician on the Medical Staff Notify the physician prior to admitting patient Prior authorization not required
Hospital Admitting Bill – effective 2014 Must be credentialed by the hospital to admit Have a collaborative arrangement with physician on the Medical Staff Notify the physician prior to admitting patient Prior authorization not required
 The “physician") Signing birth certificates – effective 2014 Changed Vital Statistics law (ORC 3705) The “physician in attendance shall…certify to the facts of birth within seventy-two hours” Most of us were signing anyway HB 95 added “or nurse-midwife” after “physician”
Signing birth certificates – effective 2014 Changed Vital Statistics law (ORC 3705) The “physician in attendance shall…certify to the facts of birth within seventy-two hours” Most of us were signing anyway HB 95 added “or nurse-midwife” after “physician”
 Delegation of medication administration to unlicensed personnel – effective 2015 Only physicians could delegate administration of non-controlled substances in outpatient setting SB 110 added APRNs/PAs
Delegation of medication administration to unlicensed personnel – effective 2015 Only physicians could delegate administration of non-controlled substances in outpatient setting SB 110 added APRNs/PAs
 Delegation CTP holder must be on location Cannot be a controlled substance nor prohibited by the Formulary or SCA Patient must be assessed and determined to be an appropriate candidate The unlicensed person must have documentation of education in med administration and demonstrates ability to safely administer the drug
Delegation CTP holder must be on location Cannot be a controlled substance nor prohibited by the Formulary or SCA Patient must be assessed and determined to be an appropriate candidate The unlicensed person must have documentation of education in med administration and demonstrates ability to safely administer the drug
 HB 216 – Modernizing the Nurse Practice Act Pending legislation Currently in House Health Committee If passed as written, it would: Remove the SCA Remove the drug formulary Remove physician-supervision requirement CRNAs Modernize CRNA prescriptive authority for
HB 216 – Modernizing the Nurse Practice Act Pending legislation Currently in House Health Committee If passed as written, it would: Remove the SCA Remove the drug formulary Remove physician-supervision requirement CRNAs Modernize CRNA prescriptive authority for
? Formal document of collaborative relationship between the") What is the Standard Care Arrangement (SCA)? Formal document of collaborative relationship between the APRN and physician Required by law for all APRNs ORC 4723. 431 OAC 4723 -8 -04, 4723 -8 -05 Except for Psych CNSs who are not prescribing medication and for CRNAs Template available: cohcaonline. org
What is the Standard Care Arrangement (SCA)? Formal document of collaborative relationship between the APRN and physician Required by law for all APRNs ORC 4723. 431 OAC 4723 -8 -04, 4723 -8 -05 Except for Psych CNSs who are not prescribing medication and for CRNAs Template available: cohcaonline. org
 SCA – new rules SCA review and reapproval every 2 years Document review of collaborating physician(s) medical license every 2 years Keep old SCAs for 3 years
SCA – new rules SCA review and reapproval every 2 years Document review of collaborating physician(s) medical license every 2 years Keep old SCAs for 3 years
 What goes in the SCA? Statement of services offered, including scope prescriptive practice Plan for incorporation of new technology or procedures Plan for coverage of patients during APRN absences Process to resolve disagreements re: patient management of
What goes in the SCA? Statement of services offered, including scope prescriptive practice Plan for incorporation of new technology or procedures Plan for coverage of patients during APRN absences Process to resolve disagreements re: patient management of
 What goes in the SCA? Quality assurance provisions: Criteria for referral to collaborating physician Process to obtain consultation with collaborating physician Process for regular review of referrals to other health care professionals Process for chart review Including twice-yearly review of prescribing practices
What goes in the SCA? Quality assurance provisions: Criteria for referral to collaborating physician Process to obtain consultation with collaborating physician Process for regular review of referrals to other health care professionals Process for chart review Including twice-yearly review of prescribing practices
 What goes in the SCA? For CTP holders, include these provisions: Ensure the patient will be personally evaluated by the physician when indicated Use of drugs with non-FDA approved indications “off-label” uses Use of new FDA-approved drugs
What goes in the SCA? For CTP holders, include these provisions: Ensure the patient will be personally evaluated by the physician when indicated Use of drugs with non-FDA approved indications “off-label” uses Use of new FDA-approved drugs
 Cervical ripening for IUD") Off-label examples Oral contraceptives Dysmenorrhea Irregular menses Acne Cytotec (misoprostol) Cervical ripening for IUD or IOL Reglan Nausea/vomiting of pregnancy
Off-label examples Oral contraceptives Dysmenorrhea Irregular menses Acne Cytotec (misoprostol) Cervical ripening for IUD or IOL Reglan Nausea/vomiting of pregnancy
 What do I do with my SCA? Keep a copy on file at practice location(s) Signed by each APN and collaborating physician Department chair can sign Include date of initial execution and the most recent review Need a new SCA if employment changes to a different setting and with different collaborating physicians
What do I do with my SCA? Keep a copy on file at practice location(s) Signed by each APN and collaborating physician Department chair can sign Include date of initial execution and the most recent review Need a new SCA if employment changes to a different setting and with different collaborating physicians
 Laws regarding APRN prescribing Nursing law Pharmacy law ORC/OAC 4729 Ohio State Board of Pharmacy pharmacy. ohio. gov Medical law ORC/OAC 4731 State Medical Board of Ohio med. ohio. gov
Laws regarding APRN prescribing Nursing law Pharmacy law ORC/OAC 4729 Ohio State Board of Pharmacy pharmacy. ohio. gov Medical law ORC/OAC 4731 State Medical Board of Ohio med. ohio. gov
 Certificate to Prescribe Course of study in advanced pharmacology Minimum 45 hrs of classroom and clinical study 6 hrs specific to Schedule 2 controlled substances, including prevention of abuse, addiction and diversion Current prescribers obtaining new Ohio COA/CTP “Classroom”requirement for Schedule 2 education has been removed
Certificate to Prescribe Course of study in advanced pharmacology Minimum 45 hrs of classroom and clinical study 6 hrs specific to Schedule 2 controlled substances, including prevention of abuse, addiction and diversion Current prescribers obtaining new Ohio COA/CTP “Classroom”requirement for Schedule 2 education has been removed
 Externship Time during which the nurse's prescribing activities are reviewed and evaluated by a supervising professional Purpose: ongoing improvement of the nurse's competence, knowledge, and skill in pharmacokinetic principles application of these principles to the nurse's area of practice.
Externship Time during which the nurse's prescribing activities are reviewed and evaluated by a supervising professional Purpose: ongoing improvement of the nurse's competence, knowledge, and skill in pharmacokinetic principles application of these principles to the nurse's area of practice.
 Initial prescribing license until APRN meets criteria of") Certificate to Prescribe Externship (Ct. P-E) Initial prescribing license until APRN meets criteria of supervised hours of prescribing Must be “supervised” for prescribing component of practice 500 hours direct supervision (on site) An APRN with Ct. P can supervise 200 of these hours 1000 hours indirect supervision (physician can be off site) Timely review of prescriptions written
Certificate to Prescribe Externship (Ct. P-E) Initial prescribing license until APRN meets criteria of supervised hours of prescribing Must be “supervised” for prescribing component of practice 500 hours direct supervision (on site) An APRN with Ct. P can supervise 200 of these hours 1000 hours indirect supervision (physician can be off site) Timely review of prescriptions written
 Certificate to Prescribe Externship Ct. PE “Consultation" - the discussion or communication between a Ct. P-E holder and a physician or APRN prior to prescribing a drug Document the consultation in the patient's record
Certificate to Prescribe Externship Ct. PE “Consultation" - the discussion or communication between a Ct. P-E holder and a physician or APRN prior to prescribing a drug Document the consultation in the patient's record
 Samples and Stock Meds May supply non-controlled samples with a 72 -hour limit Or smallest available package Stock drug dispensing limited to specific sites Health departments, federally-funded clinics, free clinics, similar non-profits And specific types of drugs Prenatal vitamins, contraceptives, antibiotics, antifungals Drugs to treat asthma, diabetes, high cholesterol, hypertension, scabies
Samples and Stock Meds May supply non-controlled samples with a 72 -hour limit Or smallest available package Stock drug dispensing limited to specific sites Health departments, federally-funded clinics, free clinics, similar non-profits And specific types of drugs Prenatal vitamins, contraceptives, antibiotics, antifungals Drugs to treat asthma, diabetes, high cholesterol, hypertension, scabies
 Committee for Prescriptive Governance Tasked by law to develop recommendations regarding prescribing of drugs and therapeutic devices by CTP holders Considers requests for Formulary revisions Reviews new FDA-approved drugs Meetings held Jan/May/Oct. at the BON Anyone may attend
Committee for Prescriptive Governance Tasked by law to develop recommendations regarding prescribing of drugs and therapeutic devices by CTP holders Considers requests for Formulary revisions Reviews new FDA-approved drugs Meetings held Jan/May/Oct. at the BON Anyone may attend
 2 pharmacists (1") CPG Members 4 nurses (1 CNS, 1 CNP, 1 BON member) 2 pharmacists (1 in clinical practice, 1 BOP member) 4 physicians (2 who work w/ APRNs, 1 in family practice, 1 BOM member)
CPG Members 4 nurses (1 CNS, 1 CNP, 1 BON member) 2 pharmacists (1 in clinical practice, 1 BOP member) 4 physicians (2 who work w/ APRNs, 1 in family practice, 1 BOM member)
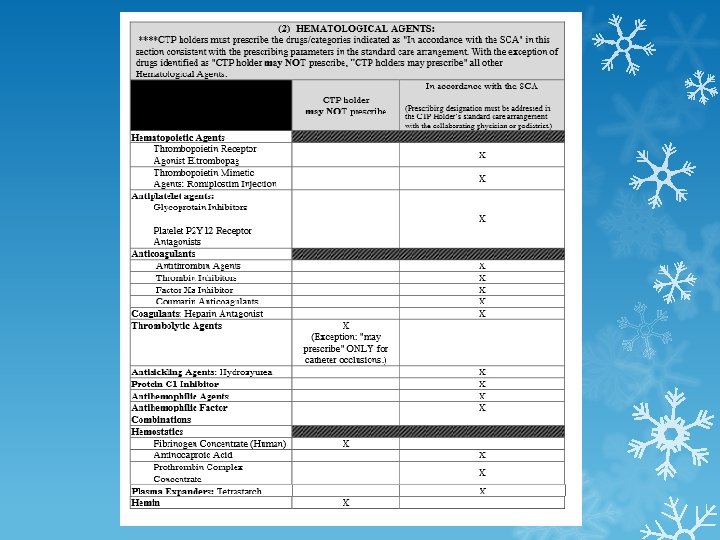
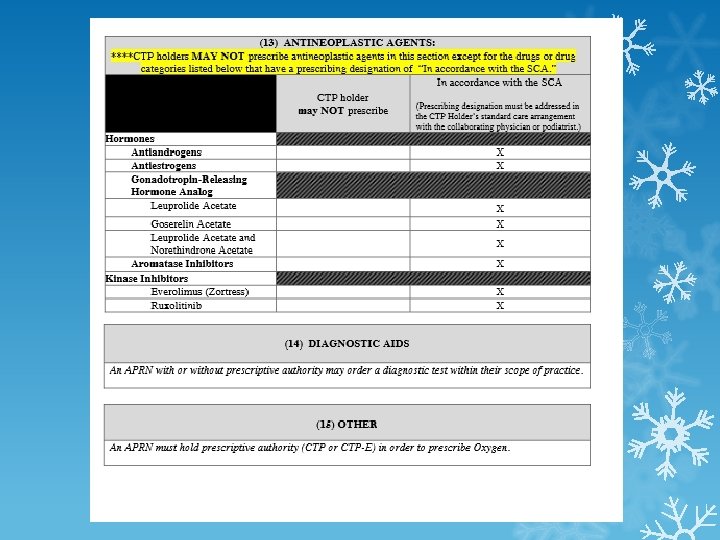
 Formulary Inclusionary Categories May NOT prescribe May prescribe in accordance with SCA All other drugs are considered to be “may prescribe”
Formulary Inclusionary Categories May NOT prescribe May prescribe in accordance with SCA All other drugs are considered to be “may prescribe”
 How can I ask the CPG to change a prescribing designation? Download the “Formulary Review and Revision Request” form www. nursing. ohio. gov Under “Prescriptive Authority Resources” link Include rationale for request, relevant literature, documented support from collaborator Submit to BON at least 30 days prior to next CPG meeting
How can I ask the CPG to change a prescribing designation? Download the “Formulary Review and Revision Request” form www. nursing. ohio. gov Under “Prescriptive Authority Resources” link Include rationale for request, relevant literature, documented support from collaborator Submit to BON at least 30 days prior to next CPG meeting
 Can I prescribe a new drug not yet reviewed by the CPG? Within the APRNs scope of practice to prescribe The formulary lists the drug type as “may prescribe” or “may prescribe per SCA” SCA includes a statement that APRN may prescribe FDA-approved drugs not yet approved by the CPG 4723 -9 -10
Can I prescribe a new drug not yet reviewed by the CPG? Within the APRNs scope of practice to prescribe The formulary lists the drug type as “may prescribe” or “may prescribe per SCA” SCA includes a statement that APRN may prescribe FDA-approved drugs not yet approved by the CPG 4723 -9 -10
 Can I prescribe to a family member? If drug is within the APRNs scope of practice to prescribe Able to exercise detached professional judgement Documented in the medical record APRN cannot prescribe controlled substances to a family member 4723 -9 -09
Can I prescribe to a family member? If drug is within the APRNs scope of practice to prescribe Able to exercise detached professional judgement Documented in the medical record APRN cannot prescribe controlled substances to a family member 4723 -9 -09
 Writing prescriptions Must be for legitimate medical purpose within usual course of practice Pharmacists are required to watch for and deal with prescribing problems
Writing prescriptions Must be for legitimate medical purpose within usual course of practice Pharmacists are required to watch for and deal with prescribing problems
 Writing prescriptions Name and address of both patient and prescriber Drug name and strength Quantity to be issued i. e. : #30 (thirty) Instructions for use Number of refills “Dispense as Written” prn
Writing prescriptions Name and address of both patient and prescriber Drug name and strength Quantity to be issued i. e. : #30 (thirty) Instructions for use Number of refills “Dispense as Written” prn
 Writing Prescriptions Dated and manually signed Ct. P license number required on all Rx’s NPI number optional DEA number required for controlled substances DEA numbers for APRNs begin with “M” DEA license $731 every 3 years deadiversion. usdoj. gov
Writing Prescriptions Dated and manually signed Ct. P license number required on all Rx’s NPI number optional DEA number required for controlled substances DEA numbers for APRNs begin with “M” DEA license $731 every 3 years deadiversion. usdoj. gov
 Transmitting prescriptions By fax or electronic transmission from the prescriber to the pharmacy Patient cannot fax their own prescription Telephone orders may be transmitted by the prescriber’s agent
Transmitting prescriptions By fax or electronic transmission from the prescriber to the pharmacy Patient cannot fax their own prescription Telephone orders may be transmitted by the prescriber’s agent
 Prescribing controlled substances Schedule 2 prescriptions must be written No refills Cannot be prescribed by APRN in "convenience care" clinic Schedule 3 -5 prescriptions may be called in or transmitted electronically to pharmacy No refills beyond 6 months Many opioid addicts were first exposed to narcotics through rx’s for legitimate pain issues
Prescribing controlled substances Schedule 2 prescriptions must be written No refills Cannot be prescribed by APRN in "convenience care" clinic Schedule 3 -5 prescriptions may be called in or transmitted electronically to pharmacy No refills beyond 6 months Many opioid addicts were first exposed to narcotics through rx’s for legitimate pain issues
 Oral Opiate Changes Combo products cannot include more than 325 mg acetaminophen Hydrocodone, Oxycodone, Butalbital FDA has reclassified all combo drugs to Schedule 2 (except acetaminophen w/ codeine) Example: write rx as hydrocodone/acetaminophen 5/325
Oral Opiate Changes Combo products cannot include more than 325 mg acetaminophen Hydrocodone, Oxycodone, Butalbital FDA has reclassified all combo drugs to Schedule 2 (except acetaminophen w/ codeine) Example: write rx as hydrocodone/acetaminophen 5/325
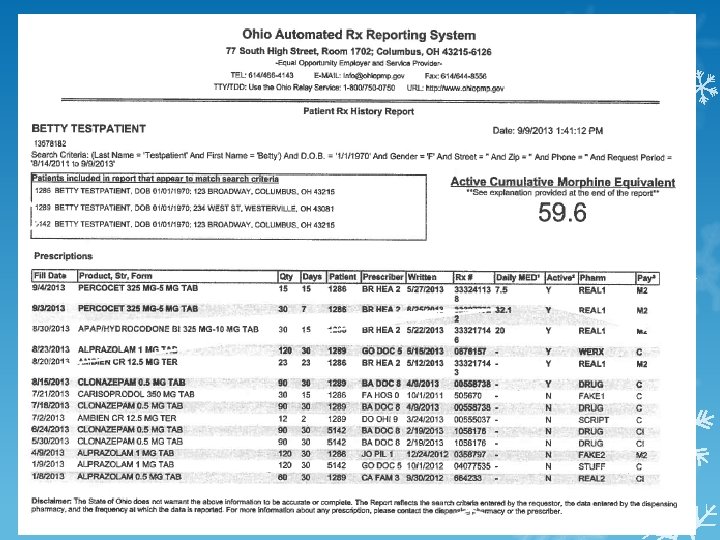
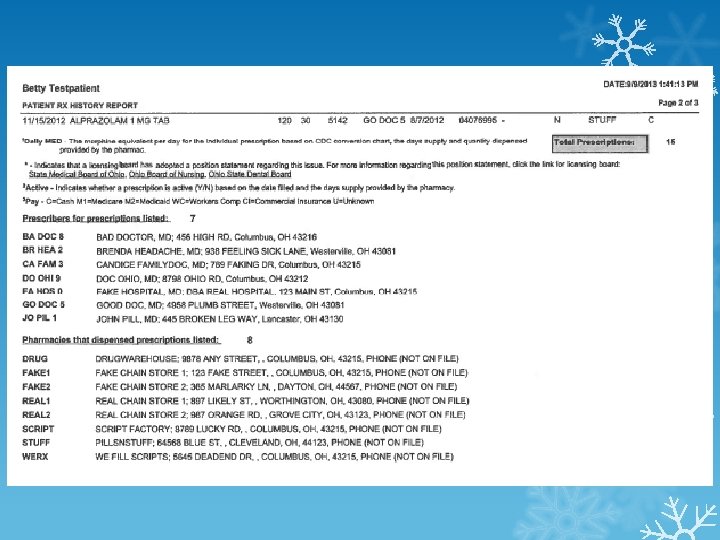
 System Database for controlled substances Authorizes BOP to Collect") Ohio Automated Rx Reporting (OARRS) System Database for controlled substances Authorizes BOP to Collect Rx data Analyze Rx data Distribute Rx data Purpose is to monitor prescriber practices and/or abuse by prescribers or patients
Ohio Automated Rx Reporting (OARRS) System Database for controlled substances Authorizes BOP to Collect Rx data Analyze Rx data Distribute Rx data Purpose is to monitor prescriber practices and/or abuse by prescribers or patients
 OARRS All controlled substances Data not available to public No liability to prescribers who use data Patients NOT included: Inpatients Physician-dispensed ER dispensed for < 24 hours Schedule 5 OTC sales
OARRS All controlled substances Data not available to public No liability to prescribers who use data Patients NOT included: Inpatients Physician-dispensed ER dispensed for < 24 hours Schedule 5 OTC sales
 How do I register for OARRS?
How do I register for OARRS?
 What red flags should trigger an OARRS review? Actual or potential signs of drug abuse or diversion:
What red flags should trigger an OARRS review? Actual or potential signs of drug abuse or diversion:
 Prescribing precautions If misuse of controlled drugs is suspected, APRN must consult with collaboration physician prior to prescribing Document review of the OARRS report and physician consultation 4723 -9 -12
Prescribing precautions If misuse of controlled drugs is suspected, APRN must consult with collaboration physician prior to prescribing Document review of the OARRS report and physician consultation 4723 -9 -12
 Opiate Initiatives opioidprescribing. ohio. gov “Guidelines for Prescribing Opioids for the Treatment of Chronic, Non-Terminal Pain” 1 -hour CE video OARRS information
Opiate Initiatives opioidprescribing. ohio. gov “Guidelines for Prescribing Opioids for the Treatment of Chronic, Non-Terminal Pain” 1 -hour CE video OARRS information
 OARRS in the news “Study: Doctors prescribing opioids post-overdose” 1/15/16 Gannett Ohio OARRS doesn’t include Naloxone given in ER “Drug theft reports now get extra scrutiny: Many theft reports are fraudulent ones filed by drug abusers and dealers, police say. ” 8/30/15 Hamilton Journal-News “Prescription drug database reduces ‘doctor shopping’” 10/26/13 Dayton Daily-News
OARRS in the news “Study: Doctors prescribing opioids post-overdose” 1/15/16 Gannett Ohio OARRS doesn’t include Naloxone given in ER “Drug theft reports now get extra scrutiny: Many theft reports are fraudulent ones filed by drug abusers and dealers, police say. ” 8/30/15 Hamilton Journal-News “Prescription drug database reduces ‘doctor shopping’” 10/26/13 Dayton Daily-News
 Avoid the midwife crisis!
Avoid the midwife crisis!
 current Notify BON if you change practice site") To-Do List Keep licenses and certification(s) current Notify BON if you change practice site or collaborator(s) Regular review of SCA, charts, prescribing practices Prescribe in compliance with the formulary Check OARRS reports
To-Do List Keep licenses and certification(s) current Notify BON if you change practice site or collaborator(s) Regular review of SCA, charts, prescribing practices Prescribe in compliance with the formulary Check OARRS reports
 Want a copy of the slides? jeanne. bauer@yahoo. com
Want a copy of the slides? jeanne. bauer@yahoo. com
 Council for Ohio Health Care Advocacy Only interprofessional health policy organization in Ohio Links APRNs, PAs, pharmacists, physicians and others Works for legislative change to improve the quality, safety and affordability of health care Jobs list (priority access to members) SCA template (free to members) Online continuing education cohcaonline. org
Council for Ohio Health Care Advocacy Only interprofessional health policy organization in Ohio Links APRNs, PAs, pharmacists, physicians and others Works for legislative change to improve the quality, safety and affordability of health care Jobs list (priority access to members) SCA template (free to members) Online continuing education cohcaonline. org