


 Know stroke: Save life
Know stroke: Save life
 Stroke Fast Facts • Affects ~ 800, 000 people per year • Leading cause of disability, cognitive impairment, and death • Stroke is № 3 cause of death in R. F. (№ 5 in U. S. ) • 37% of all americans cannot exactly identify even one warning sign for stroke
Stroke Fast Facts • Affects ~ 800, 000 people per year • Leading cause of disability, cognitive impairment, and death • Stroke is № 3 cause of death in R. F. (№ 5 in U. S. ) • 37% of all americans cannot exactly identify even one warning sign for stroke
 Brain Organisation Cerebrum Cerebellum Brain stem
Brain Organisation Cerebrum Cerebellum Brain stem
 Cerebral Blood Supply Cerebrum Cerebellum Brainstem Middle cerebral a. Superior Pontine cerebellar a. branches Anterior cerebral a. Anterior inf. Anterior cerebellar a. spinal aa. Posterior cerebral a. Posterior inf. cerebellar a. The most important questions: 1) Where is the damage in the brain? 2) How much tissue are included
Cerebral Blood Supply Cerebrum Cerebellum Brainstem Middle cerebral a. Superior Pontine cerebellar a. branches Anterior cerebral a. Anterior inf. Anterior cerebellar a. spinal aa. Posterior cerebral a. Posterior inf. cerebellar a. The most important questions: 1) Where is the damage in the brain? 2) How much tissue are included
 What is Stroke? • The term “stroke” encompasses both ischemic and hemorrhagic disturbances of the cerebral circulation producing central neurological deficits of acute or subacute onset. • The stoppage of blood flow – ischemic stroke (80 -85%) • The rupture of the blood vessel – hemorrhagic stroke (15 -20%)
What is Stroke? • The term “stroke” encompasses both ischemic and hemorrhagic disturbances of the cerebral circulation producing central neurological deficits of acute or subacute onset. • The stoppage of blood flow – ischemic stroke (80 -85%) • The rupture of the blood vessel – hemorrhagic stroke (15 -20%)
 Diabetes mellitus, smoking, cholesterol") Risk Factors of Stroke Non-modifiable Modifiable Age Hypertension Sex (males) Diabetes mellitus, smoking, cholesterol (damaging the vessel wall) Ethnicity Heart risk factors: atrial fibrillation, heart attack, heart failure Previous strokes or TIA
Risk Factors of Stroke Non-modifiable Modifiable Age Hypertension Sex (males) Diabetes mellitus, smoking, cholesterol (damaging the vessel wall) Ethnicity Heart risk factors: atrial fibrillation, heart attack, heart failure Previous strokes or TIA
 Consequences of Ischemia • Ischemic penumbra – the zone of the tissue in which the local cerebral perfusion lies between the functional threshold and the infarction threshold. Due to collateral arteries! • Unconsciousness in 10 -12 sec • EEG ceases in 30 -40 sec • Cytotoxic cerebral edema. The ischemic cascade • Vasogenic cerebral edema • Compression of the brain tissue. Brain swelling • Post stroke inflammation (necrosis, cavity)
Consequences of Ischemia • Ischemic penumbra – the zone of the tissue in which the local cerebral perfusion lies between the functional threshold and the infarction threshold. Due to collateral arteries! • Unconsciousness in 10 -12 sec • EEG ceases in 30 -40 sec • Cytotoxic cerebral edema. The ischemic cascade • Vasogenic cerebral edema • Compression of the brain tissue. Brain swelling • Post stroke inflammation (necrosis, cavity)
 Ischemic Core and Penumbra Normal function 20 15 10 Neuronal dysfunction PENUMBRA 5 CORE 1 2 CBF 8 -18 Neuronal death CBF <8 3 TIME (hours) CEREBRAL BLOOD FLOW (ml/100 g/min) Clot in Artery Penumbra Core
Ischemic Core and Penumbra Normal function 20 15 10 Neuronal dysfunction PENUMBRA 5 CORE 1 2 CBF 8 -18 Neuronal death CBF <8 3 TIME (hours) CEREBRAL BLOOD FLOW (ml/100 g/min) Clot in Artery Penumbra Core
 Classification of Cerebral Ischemia by Temporal Course • Ischemia causes critical hypoperfusion in the area of the brain • May be either transient(TIA, RIND) or permanent(completed stroke) TIA=Transient Ischemic Attack 2 -15 min, sometimes as long as 24 hours RIND=Reversible Ischemic Neurological Deficit Up to 7 days Stroke in evolution, progressive stroke Stroke with neurological deficits that continue to worsen for hours or days after onset Completed stroke Established neurological deficit that is irreversible or only partly reversible
Classification of Cerebral Ischemia by Temporal Course • Ischemia causes critical hypoperfusion in the area of the brain • May be either transient(TIA, RIND) or permanent(completed stroke) TIA=Transient Ischemic Attack 2 -15 min, sometimes as long as 24 hours RIND=Reversible Ischemic Neurological Deficit Up to 7 days Stroke in evolution, progressive stroke Stroke with neurological deficits that continue to worsen for hours or days after onset Completed stroke Established neurological deficit that is irreversible or only partly reversible
 Ischemic Stroke Classification by etiology: 1. Atherosclerosis of large extra- and intracranial vessels (atherosclerotic plaque, hemodynamic insufficiency in poststenotic circulation) 2. Embolic events (arterio-arterial, cardiogenic embolization) 3. Cerebral small vessel disease/atherosclerosis (high BP) 4. Other etiology (vasculopathies, coagulopathies) 5. Obstruction of venous outflow (venous sinus thrombosis) 6. Undetermined etiology Types: 1. Territorial infarcts 2. Watershed infarcts 3. Lacunar infarcts (small vessel strokes)
Ischemic Stroke Classification by etiology: 1. Atherosclerosis of large extra- and intracranial vessels (atherosclerotic plaque, hemodynamic insufficiency in poststenotic circulation) 2. Embolic events (arterio-arterial, cardiogenic embolization) 3. Cerebral small vessel disease/atherosclerosis (high BP) 4. Other etiology (vasculopathies, coagulopathies) 5. Obstruction of venous outflow (venous sinus thrombosis) 6. Undetermined etiology Types: 1. Territorial infarcts 2. Watershed infarcts 3. Lacunar infarcts (small vessel strokes)
, retinal infarction") Signs & Symptoms • Ophthalmic a. – amarourosis fugax (transient monocular blindness), retinal infarction • ICA – monocular visual lost and contralateral hemiparesis (oculocerebral syndrome) • MCA – brachiofacial hemiparesis and hemisensory deficit, homonymous hemi/quadrantanopsia, horizontal gaze palsy, impairment of spatial orientation • Other: apathy, abulia, hemiballism, mild paresis • Brainstem infarcts: lacunar, depends on the particular brainstem nuclei and fiber tracts that they affect: ipsilateral cranial nerve deficits and a contralateral hemisensory defect/hemiparesis • Cerebellar infarcts: vertigo, nausea, unsteady gait, acute headache, dysarthria Impairment of gait: circumduction of the spastically extended lower limb + flexion of the paretic upper limb at the wrist and elbow + absence of arm swing on the affected side (Wernicke-Mann gait)
Signs & Symptoms • Ophthalmic a. – amarourosis fugax (transient monocular blindness), retinal infarction • ICA – monocular visual lost and contralateral hemiparesis (oculocerebral syndrome) • MCA – brachiofacial hemiparesis and hemisensory deficit, homonymous hemi/quadrantanopsia, horizontal gaze palsy, impairment of spatial orientation • Other: apathy, abulia, hemiballism, mild paresis • Brainstem infarcts: lacunar, depends on the particular brainstem nuclei and fiber tracts that they affect: ipsilateral cranial nerve deficits and a contralateral hemisensory defect/hemiparesis • Cerebellar infarcts: vertigo, nausea, unsteady gait, acute headache, dysarthria Impairment of gait: circumduction of the spastically extended lower limb + flexion of the paretic upper limb at the wrist and elbow + absence of arm swing on the affected side (Wernicke-Mann gait)
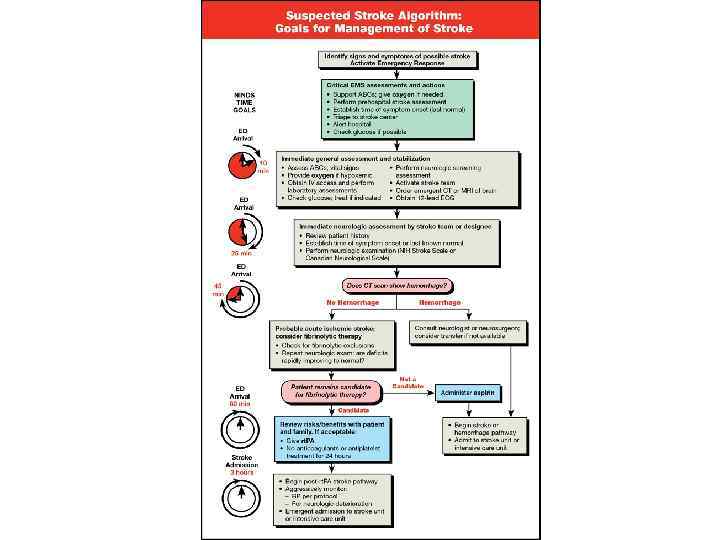
 Diagnostic Precise history taking A thorough clinical neurological examination Examination of the CVC Laboratory tests: ESR, blood sugar, lipid profile, complete blood count and HBN, coagulation profile, protein C, antiphospholipid antibodies • Imaging studies: CT – acute brain hemorrhage; MRI – infarct zone, perifocal edema; doppler ultrasonography; ECG; angio-MRI; cerebral angiography; echocardiography • •
Diagnostic Precise history taking A thorough clinical neurological examination Examination of the CVC Laboratory tests: ESR, blood sugar, lipid profile, complete blood count and HBN, coagulation profile, protein C, antiphospholipid antibodies • Imaging studies: CT – acute brain hemorrhage; MRI – infarct zone, perifocal edema; doppler ultrasonography; ECG; angio-MRI; cerebral angiography; echocardiography • •
 Determining the Location • Large Vessel: – Look for cortical signs • Small Vessel: – No cortical signs on exam • Posterior Circulation: – Crossed signs – Cranial nerve findings • Watershed: – Look at watershed and borderzone areas – Hypo-perfusion
Determining the Location • Large Vessel: – Look for cortical signs • Small Vessel: – No cortical signs on exam • Posterior Circulation: – Crossed signs – Cranial nerve findings • Watershed: – Look at watershed and borderzone areas – Hypo-perfusion
 Cortical Signs Right brain: - Right gaze preference - Neglect Left brain: - Left gaze preference - Aphasia If present, think LARGE VESSEL stroke
Cortical Signs Right brain: - Right gaze preference - Neglect Left brain: - Left gaze preference - Aphasia If present, think LARGE VESSEL stroke
 – Expressive aphasia –") Aphasia Broca’s: Left posterior inferior frontal gyrus (fluid speech production) – Expressive aphasia – slowly & poor articulated speech Wernicke’s: Posterior part of the superior temporal gyrus (understanding) – Receptive aphasia – Poor comprehension of what people are saying to you
Aphasia Broca’s: Left posterior inferior frontal gyrus (fluid speech production) – Expressive aphasia – slowly & poor articulated speech Wernicke’s: Posterior part of the superior temporal gyrus (understanding) – Receptive aphasia – Poor comprehension of what people are saying to you
 Case 1 • 74 year old African American female with sudden onset of left-sided weakness • She was at church when she noted left facial droop • History of HTN and atrial fibrillation • Meds: Losartan
Case 1 • 74 year old African American female with sudden onset of left-sided weakness • She was at church when she noted left facial droop • History of HTN and atrial fibrillation • Meds: Losartan
 Examination • BP- 172/89, P– 104, T- 98. 0, RR– 22, O 2 - 94% • General exam: Unremarkable except irregular rate and rhythm • NEURO EXAM: - Speech dysarthric but language intact - Right gaze preference - Left facial droop - Left-sided hemiplegia - Neglect
Examination • BP- 172/89, P– 104, T- 98. 0, RR– 22, O 2 - 94% • General exam: Unremarkable except irregular rate and rhythm • NEURO EXAM: - Speech dysarthric but language intact - Right gaze preference - Left facial droop - Left-sided hemiplegia - Neglect
 Imaging studies
Imaging studies
 Case 1 • Right MCA infarct, most likely cardioembolic from atrial fibrillation • Patient underwent mechanical thrombectomy with intra-arterial verapamil, clot removal successful • Excellent recovery – patient was discharged 48 hours later on Coumadin
Case 1 • Right MCA infarct, most likely cardioembolic from atrial fibrillation • Patient underwent mechanical thrombectomy with intra-arterial verapamil, clot removal successful • Excellent recovery – patient was discharged 48 hours later on Coumadin
 Case 2 • 85 year old male who woke up with left face, arm, and leg numbness • History of HTN, DM, and tobacco use • Meds: Insulin, aspirin • BP- 168/96, P– 92 • General exam: Unremarkable • NEURO EXAM: No cortical signs on exam; Decreased sensation on left face, arm, and leg
Case 2 • 85 year old male who woke up with left face, arm, and leg numbness • History of HTN, DM, and tobacco use • Meds: Insulin, aspirin • BP- 168/96, P– 92 • General exam: Unremarkable • NEURO EXAM: No cortical signs on exam; Decreased sensation on left face, arm, and leg
 Imaging studies
Imaging studies
 Case 2 • Right thalamic lacunar infarct • Discharged to rehab 72 hours after admission
Case 2 • Right thalamic lacunar infarct • Discharged to rehab 72 hours after admission
 • Sumarachnoid hemorrhage (SAH) Etiology of ICH: 1.") Hemorrhagic Stroke • Intracerebral hemorrhage (ICH) • Sumarachnoid hemorrhage (SAH) Etiology of ICH: 1. Due to the rupture of vascular lesions of hypertensive origin 2. Aneurysms (saccular or “berry-like”) 3. Arteriovenous malformations 4. Bleeding diathesis 5. In hypertensive crisis or drug abuse (cocane) Etiology of SAH: 1. Spontaneous rupture of a saccular aneurysm or an artery at the base of the brain 2. Arteriovenous malformations 3. Vasculopathies , coagulopathies 4. Preceding trauma
Hemorrhagic Stroke • Intracerebral hemorrhage (ICH) • Sumarachnoid hemorrhage (SAH) Etiology of ICH: 1. Due to the rupture of vascular lesions of hypertensive origin 2. Aneurysms (saccular or “berry-like”) 3. Arteriovenous malformations 4. Bleeding diathesis 5. In hypertensive crisis or drug abuse (cocane) Etiology of SAH: 1. Spontaneous rupture of a saccular aneurysm or an artery at the base of the brain 2. Arteriovenous malformations 3. Vasculopathies , coagulopathies 4. Preceding trauma
 Common Sites of saccular aneurysms
Common Sites of saccular aneurysms
 Clinical Manifestations ICH SAH Chronic arterial hypertension, advanced age Worst headache of my life Impairment of consciousness Nausea and vomitting Generalized epileptic seizures Impairment of consciousness Cranial nerve palsies
Clinical Manifestations ICH SAH Chronic arterial hypertension, advanced age Worst headache of my life Impairment of consciousness Nausea and vomitting Generalized epileptic seizures Impairment of consciousness Cranial nerve palsies
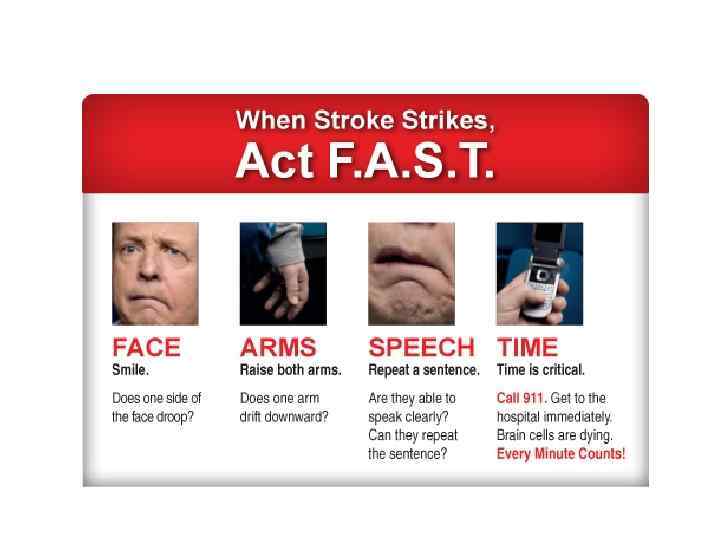
 Face: Asymmetry. Drooping of their mouth on one side. Ask to smile Arm: Difficulty or inability in raising one or both hands Speech: Slurred. May not be really able to understand what you are saying to them Time to call 112 or 03 VIDEO! https: //www. youtube. com/watch? v=w. H 7 k 5 CFp 4 h. I
Face: Asymmetry. Drooping of their mouth on one side. Ask to smile Arm: Difficulty or inability in raising one or both hands Speech: Slurred. May not be really able to understand what you are saying to them Time to call 112 or 03 VIDEO! https: //www. youtube. com/watch? v=w. H 7 k 5 CFp 4 h. I
 Symptoms 1. Sudden numbness and weakness: face/arm/leg 2. Sudden trouble speaking or understanding others because of the damage of the key speech areas 3. Sudden trouble in seeing in one or both eyes 4. Sudden dizziness or loss of balance or coordination 5. Sudden severe headache
Symptoms 1. Sudden numbness and weakness: face/arm/leg 2. Sudden trouble speaking or understanding others because of the damage of the key speech areas 3. Sudden trouble in seeing in one or both eyes 4. Sudden dizziness or loss of balance or coordination 5. Sudden severe headache
 • Would you be able to recognize the signs of") Upon reflection (savvy? ) • Would you be able to recognize the signs of a stroke? • Are you at risk for a stroke? • VIDEO! https: //www. youtube. com/watch? v=5 ZNv. ZP 5 a. QT 8
Upon reflection (savvy? ) • Would you be able to recognize the signs of a stroke? • Are you at risk for a stroke? • VIDEO! https: //www. youtube. com/watch? v=5 ZNv. ZP 5 a. QT 8
 Information: • http: //www. strokeassociation. org/STROKEORG/ • https: //www. khanacademy. org/science/health-andmedicine/circulatory-system-diseases#stroke • Fundamentals of neurology. 2006 Thieme
Information: • http: //www. strokeassociation. org/STROKEORG/ • https: //www. khanacademy. org/science/health-andmedicine/circulatory-system-diseases#stroke • Fundamentals of neurology. 2006 Thieme
 Thank you!
Thank you!