60e24bfecee4d07321555c9c2c03f88d.ppt
- Количество слайдов: 50



JRCPTB Key points from the new CMT GIM curricula Guide for trainers and trainees

Rationale for change • 2007 curricula split into 2 parts - GIM/acute and generic • Need simple way of clearly linking to GMC Good Medical Practice which will enable relicensing for Juniors • Need to retain good features e. g. Top 20 presentations, linkage of competences to assessments, use of e. Portfolio • Need to link to 2009 Academy work that all curricula will have a common competences section (replaces generic) • MRCP (UK) did not map to CMT curriculum and not necessary to complete Core training i. e. position of exam unclear • Levels 1, 2 and 3 not easily defined • Trainee and service pressure to redevelop clarity over specialty of GIM and loss of dual CCT • JRCPTB desire to support separate specialty of Acute Medicine JRCPTB

Moving from the two Curricula of 2007

JRCPTB To a new single curriculum for 2009

Moving from a career pathway like this JRCPTB

Moving to a career pathway like this Selection FY 2 36 to 60 months to completion minimum Selection Core Medical Training or Acute Care Common Stem GIM Training MRCP (UK) and WPBAs Work place based assessments JRCPTB

Moving to a career pathway like this for dual CCT Selection 60 months to completion minimum Selection Specialty Core Medical Training Specialty FY 2 GIM MRCP Work Placed Based Assessments JRCPTB
 • Core competences have replaced the generic curriculum and will underpin")
Main features (1) • Core competences have replaced the generic curriculum and will underpin all speciality curricula • 4 Emergency, ‘Top 20’ and ‘Other Presentations’ remain • All parts of the curricula have mapped assessments • MRCP in its three components Part 1, Part 2 and PACES maps to all parts of the curriculum for the CMT stage of GIM training and is necessary for full completion of CMT JRCPTB
 • Spiral curriculum remains, GIM represents ‘maturation’ of the CMT trainee")
Main features (2) • Spiral curriculum remains, GIM represents ‘maturation’ of the CMT trainee • For system and symptom specific competences clearly defined, assessments will ‘sample’ the curriculum. One assessment will usually cover several areas of the curriculum. • Procedural competences clearly defined • Progression through the full curricula well defined by the decision aids JRCPTB

JRCPTB Examples of the new layout Curriculum starts with common competences
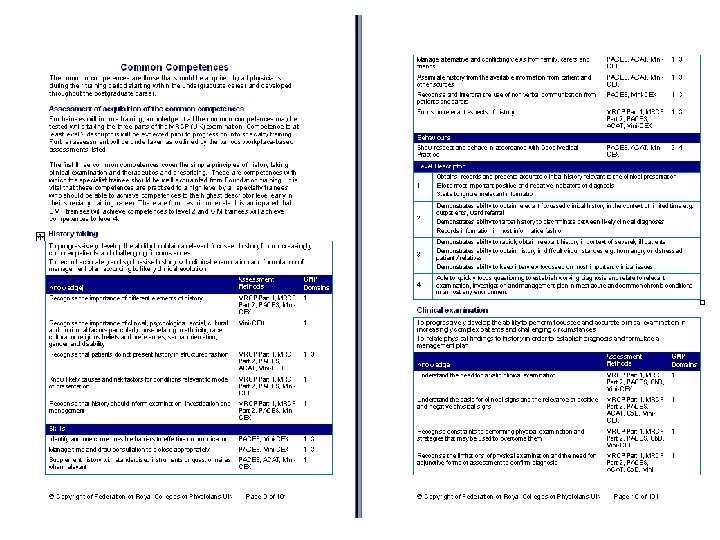

Layout of syllabus • Standardised throughout – knowledge, skills, behaviours • Assessment methods highlighted e. g. Cb. D, ACAT and mini-CEX • Four Domains of the new framework for GMC Good Medical Practice which each item relates to highlighted • For Common Competences – descriptor levels described 1 -2, relevant to CMT and 3 -4 Specialty training • Will be linked and “made live” by e. Portfolio JRCPTB


• Will enable Relicensing for Junior Doctors by providing evidence such as work place based assessments and MRCP attainment from the e. Portfolio JRCPTB

Emergency presentations

Top 20 Presentations

Other important presentations

System specific competences

Moving from just a computer exercise • New curricula will be fully integrated with e. Portfolio • Competences will be achieved from work place based assessments and MRCP • Consultants playing an active part in this JRCPTB

CMT e-Portfolio Assessors Aug 08 – May 09 ACAT percentage Average overall rating 44 5. 04 Consultant 4087 Sp. R 4771 52 SAS 399 4 5. 09

CMT e-Portfolio Assessors Aug 08 – May 09 CBD percentage Average overall rating 45 5. 00 Consultant 4134 Sp. R 4604 51 SAS 357 4 5. 07

CMT e-Portfolio Assessors Aug 08 – May 09 mini-CEX Consultant 3215 28% 5. 04 Sp. R 7268 63% 5. 11 SAS 4% Nurse 1% GP 0 SHO 2% Other 2%

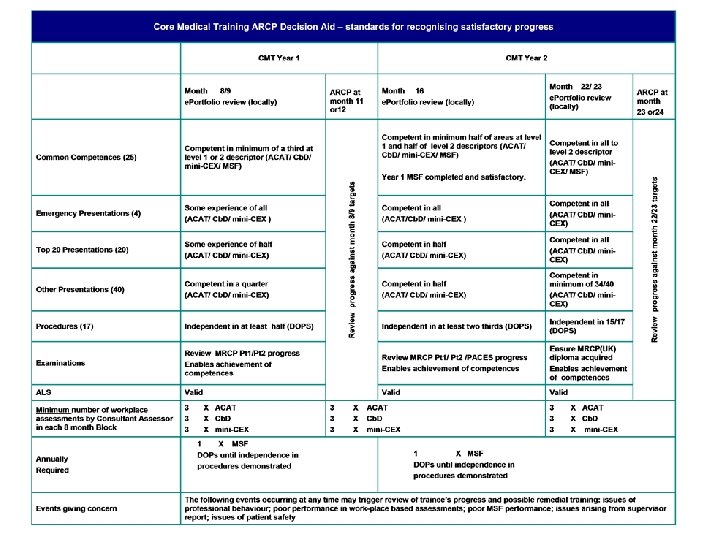
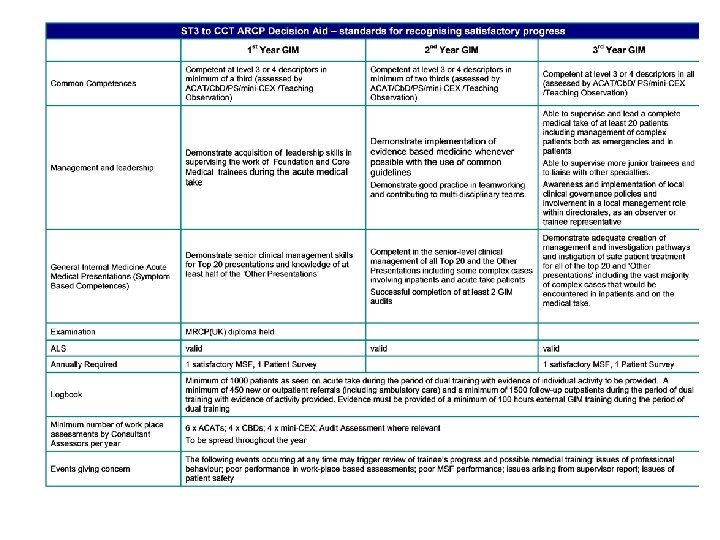
Key to progression is the ARCP decision grid • Based on feedback from users e. g. CMT Committee and Ho. S • Recognises portfolio review at 8, 16 and 23 • ARCP annual at 11 or 12 and 23 or 24 • More clarity e. g. numbers of assessments in each 8 month block and minimum by consultants • Explicit about achievement of all parts of MRCP being necessary for full completion of CMT and attainment of CMT certificate JRCPTB

Key to implementation will be continuing use of e. Portfolio Will look the same Link to new curricula Will still be able to link a number of competences to single assessment and now include parts of MRCP JRCPTB
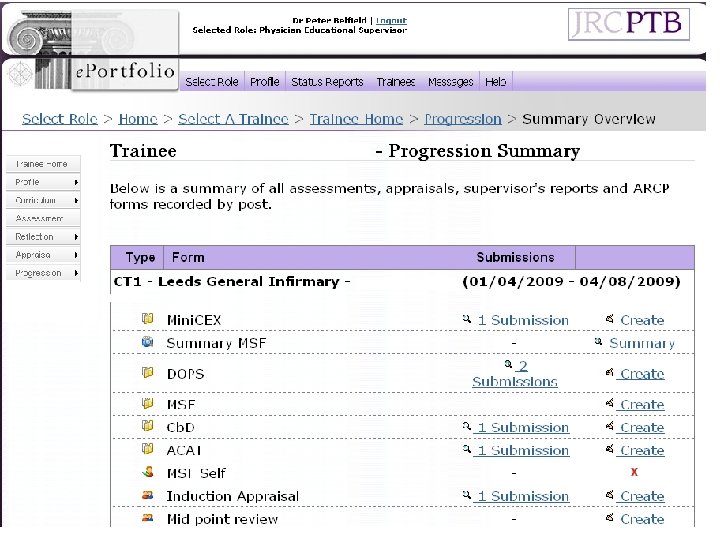

Example portfolio
 • Fully mapped to CMT part of GIM curricula • There was a")
MRCP(UK) • Fully mapped to CMT part of GIM curricula • There was a change in regulations in 2008 • Part 1 can still be taken in FY 2 year as previously but now can be taken after one years experience as opposed to 18 months • Part 2 and PACES can be taken simultaneously if wanted • CMT final certification of completion requires full MRCP (career progress with this during training will be monitored with ARCP and depending on progress may be extended in exceptional circumstances for some trainees for >2 years) JRCPTB

Significant task of implementation • All new 2009 CMT trainees start on new 2009 GIM curricula on CMT part • CMT trainees who started in 2008 will complete the 2007 curricula (acute conditions and generic) on which they started • Need to inform trainees and trainers of change which starts in August 2009 JRCPTB

JRCPTB CMT part of new curriculum Affects 2000 trainees and trainers from August 2009

JRCPTB Specialty training in GIM
 is")
Implementation of the GIM curriculum in acute medical specialties • Passing of MRCP(UK) is now one of the main required competences to exit from CMT • e. Portfolio used to record acquisition of competences • Logbook of anonymised patient contacts where possible, ’experience’ prior to August 2007 will be accepted • GIM competences will usually be acquired on the acute medical take and in triaged in-patient wards and specialty outpatient clinics JRCPTB
 • ARCP crucial • Documentary evidence of WPBA’s essential • HOS’/SAC SHA")
GIM progression(1) • ARCP crucial • Documentary evidence of WPBA’s essential • HOS’/SAC SHA reps will need to establish close links with GIM and acute medical specialty training program directors to ensure that specialty STC’s have a designated GIM- responsible STC member. JRCPTB
 • TPD’s/college tutors and educational supervisors must ensure that the eportfolio is")
GIM progression(2) • TPD’s/college tutors and educational supervisors must ensure that the eportfolio is properly completed, ARCP’s are properly conducted and that trainees are gathering their documentary evidence. • JRCPTB will need to link more closely to STC chairs and TPD’s JRCPTB

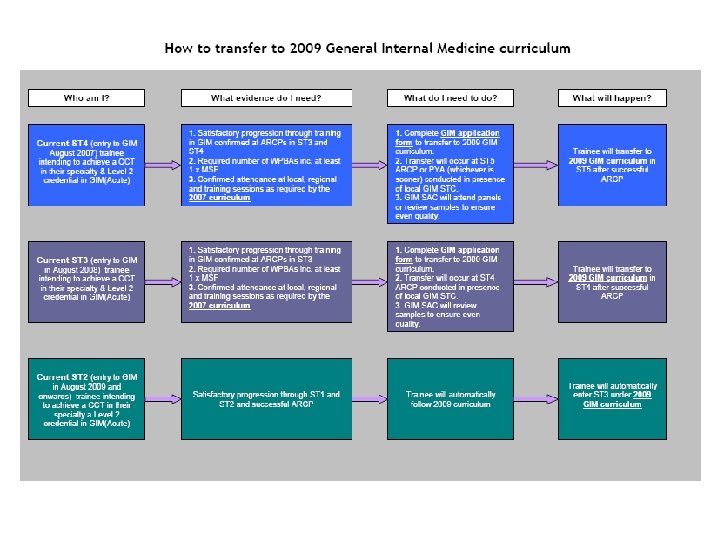
Current status of trainees re CCT in GIM • Pre January 2003, dually accrediting-no change • January 2003 -July 2007, dually accrediting-no change • July 2007 -July 2009, recruited into single medical specialty training, eligible for level 2 credential in GIM/Acute Medicine: will be able to apply to transfer to the new GIM curriculum and then progress to a CCT in GIM as well as their specialty provided that the curricula requirements are fulfilled. JRCPTB

Current status of July 2007 -July 2009 GIM/Acute level 3 STR’s • The 350 STR’S in this group can remain in their current training programs where they will receive a CCT in GIM/acute medicine. or, • They can apply to transfer to the new acute medicine curriculum once this has PMETB approval and acute medicine is recognised as a speciality. This new curriculum will award a CCT in Acute Medicine, provided the training program is successfully completed. JRCPTB

Questions about CCT’s • Can level 3 GIM/acute STR’s obtain a new GIM CCT as well as an acute medicine CCT? (yes, in theory) • Can level 2 GIM/acute STR’s transfer to the new acute medicine curriculum? (no , but they can get a GIM/acute CCT by completing a one year MAU -based high quality training post) • Are there any legal/mandatory problems in allowing transfer for level 2 trainees without external assessment of their training but by ‘sampling’ of trainee portfolios in each deanery? (should be OK) JRCPTB

Communication plan • • • Heads of Schools JRCPTB RAs SACs RCP Trainees Committee CMT Committee College Tutors Educational Supervisors Fellows Trainees JRCPTB

JRCPTB How will GIM/Acute Trainees transfer to the new GIM curriculum? From October 2009
 • WPBAs as defined in the GIM (Acute) ARCP Decision Aid •")
Required evidence(1) • WPBAs as defined in the GIM (Acute) ARCP Decision Aid • Minimum: – 3 ACATs (aiming for 6), 4 mini-CEX and 4 Cb. D per year; – DOPS until independence in procedures demonstrated; – MSF JRCPTB
 • Evidence of attendance at a minimum of 70% of Deanery training")
Required evidence(2) • Evidence of attendance at a minimum of 70% of Deanery training days where 2 hours of GIM is provided • Evidence of attendance at a minimum of 35 hours per year of external GIM conferences or courses • A proportion of this training can be achieved by recognition of e-learning modules JRCPTB
 • Personal management of an indicative number of 300 patients per year")
Required evidence(3) • Personal management of an indicative number of 300 patients per year admitted on the general medical “take” • Personal management of equivalent over 3 years of 450 new outpatients/and or inpatient complex referrals or ambulatory care patients JRCPTB
 • Demonstrated senior level competence in the Top 20 and Other Presentations")
Required evidence(4) • Demonstrated senior level competence in the Top 20 and Other Presentations JRCPTB

Outpatients • 450 new out patients over the duration of training can include new interfirm referrals • It is essential that logbooks are used to record OP and interfirm referral numbers • Workplace-based assessments are the key to providing documentary evidence of GIM exposure JRCPTB

Outpatients experience • Usually in the primary specialty • Can be obtained in clinics in other specialties • Minimum of 450 new or referral patients over dual training period • Minimum of 1500 follow up patients over the dual training period JRCPTB

Context of in and out patients • GIM experience can be accumulated in specialty in patient wards and in specialty out patients where patients often have multisystem conditions. This will usually occur in the trainee’s own specialty. JRCPTB
 and ST 5 (2007 entry) • ST")
Transferring to GIM in ST 4(2008 entry) and ST 5 (2007 entry) • ST 4 trainees will transfer at their ARCP conducted in the presence of local GIM STC. • ST 5 trainees will transfer at their PYA or ARCP (whichever is sooner) in the presence of local GIM STC. This will require more time for these PYA’s and new documentation from JRCPTB to facilitate a review of training before the PYA. • Externality will be provided by the SAC ‘sampling’ the PYAs and ARCPs on a random basis to ensure even quality. JRCPTB
60e24bfecee4d07321555c9c2c03f88d.ppt