c7b95fc4703ff039256edd662bb25f15.ppt
- Количество слайдов: 34



Issues Regarding Qualification/Implementation of an Antibody Test for Trypanosoma cruzi Susan L. Stramer, Ph. D American Red Cross Blood Products Advisory Committee Meeting April 26, 2007 E 011375 A (03 -13 -01) 1

Outline u Clinical study design and results – 8/28/06 to 1/28/07 – 3 regions (West Division); So. Cal, No. Cal, AZ – MMWR 2/23/07; 56 (07): 141 -143 u Implementation: AABB Association Bulletin #06 -08 u IVD results 1/29/07 -4/17/07; approx 65% collected blood US – ARC, UBS, 15 other blood centers and >50 hospitals – Distribution in US and accuracy of predictions u Test performance – ELISA, RIPA, T. cruzi IFA, Leishmania IFA, “Special Protocol” u Lookback results u Donor demographics – Risk factors – Possible autochthonous cases (indigenous, native) E 011375 A (03 -13 -01) 2

Chagas Protocol/Assumptions u FDA request of Ortho to expand clinical studies to include areas where T. cruzi antibody prevalence previously documented – Pivotal clinical trial yield 0 conf’d pos (of 40, 665 tested); 99. 998% specificity (PI) – 100, 000 donations defined the study – Testing would continue through test licensure and implementation – So. Cal, No. Cal and AZ (West ARC Division) • FDA requirements for donor informed consent – Use of an information sheet with signature on BDR acknowledging receipt not allowed – Specific signature and date required on info sheet; matched to tubes that were tested • Due to these requirements, other blood centers declined E 011375 A (03 -13 -01) 3

ARC Prevalence Study T. cruzi Results 8/28/06 -1/28/07 All sites So. Cal Arizona No. Cal Total Attempted Donors Total Tested 189, 828 127, 053 26, 601 36, 174 148, 969 95, 662 23, 981 29, 326 Total RR 63 (1: 2365) 50 (1: 1913) 4 (1: 5995) 9 (1: 3258) Confirmed Total (%) Refusals 32 (1: 4655) 40, 859 (21. 5%) 25 (1: 3827) 2 (1: 11, 990) 31, 391 2620 (24. 7%) (9. 8%) 5 (1: 5865) 6848 (18. 9%) 40, 859 refusals/detection rate of 1: 4655 = 9 undetected donors! E 011375 A (03 -13 -01) 4

The prevalence of infection with T. cruzi in the US varies by region and might now be higher than previously thought, especially in geographic areas such as Los Angeles County, where a substantial proportion of blood and organ donors have emigrated from Chagas-endemic countries. MMWR 55 (29); 2006 E 011375 A (03 -13 -01) 5

Implementation u According to AABB Assn Bull #06 -08 – Collaboration with the CDC and FDA u Component mgmt – Components from RR donors quarantined/withdrawn from the market (3 calendar days) • Index • Prior in-date donations – As long as electronic records exist – Recipient tracing – Autologous unit release with approval of auto donor’s referring physician – Inventory testing (in-house or distributed) not recommended; each facility assess risk E 011375 A (03 -13 -01) 6

Implementation u Donor mgmt – RRs notified/deferred – Supplemental testing encouraged, although no FDA licensed confirmatory/supplemental test exists • RIPA most sensitive test, however not 100% – Leishmania testing on supplemental test unconfirmed; no mention Plasmodium or Paracoccidiodes braziliensus – Donor counseling including donor follow-up studies encouraged – No donor reentry – Refer supplemental test positive donors to knowledgeable physician • Referrals from personal physician, blood center, Am Assoc Tropical Med or CDC – Recipient tracing from supplemental test positive donors • “Licensed test for Ab detection has suitable performance characteristics for blood donor screening and as such may be useful in testing of the above individuals. ” u COI and Component Labels – Component tested by a licensed test and the results are negative/nonreactive E 011375 A (03 -13 -01) 7

Models for Testing/Implementation u Universal u Immunosuppressed patients – Puts burden on hospitals to identify correct units for recipients at highest risk u Geographic models – By US census data/WHO seroprevalence by country u Test one-time-only per donor where only new donors are tested; repeat donors are questioned re risk and only “yes” responses are tested – Assumes donor understands the questions, questions may be culturally sensitive, assumes no autochthonous risk – Must be validated; each positive requires knowledge of risk and when it occurred – Logistically complex relative to sample tracking and component management – Financial benefit has not been validated – Confusing message to test kit developers E 011375 A (03 -13 -01) 8

Total RR Donors RIPA Pos RIPA Reported ARC 213 41 191 Blood Systems T. cruzi Reactive Donors by State of Residence (01/29/07 – 04/17/07) 52 7 (2) 29 (4) 1 4 1 3 2 3 7 6 2 7 4 4 12 6 4 2 3 37 6 2 1 3 3 6 1 3 5 10 1 15 3 8 1 2 Nos. indicate 265 RR donors by state; no RR donors or testing not occurring in 6 states; 48 confirmed pos (+2) in 17 states: 19 CA, 11 FL, 3 MD, 2 NY, UT, VA; 1 AR, CT, GA, MT, NC, NJ, OR TN, WA, (AZ) 3 1 3 2 5 8 PR 4 2 56

RR donations reported to the AABB; 4/24/07 7 facilities reporting; 4 sites with RR donors 272 total RR E 011375 A (03 -13 -01) 10

Confirmed pos reported to the AABB website Of 228 = 21. 5% E 011375 A (03 -13 -01) 11

Do the states in which confirmed positive donors agree with models based on immigration? E 011375 A (03 -13 -01) 13

Based on immigration and test positive rates for endemic countries N. J. - N. Y. Metro L. A. County Washington, D. C.
 15")
E 011375 A (03 -13 -01) 15
 – PPV = 32 RIPA pos/63 RR=51%;")
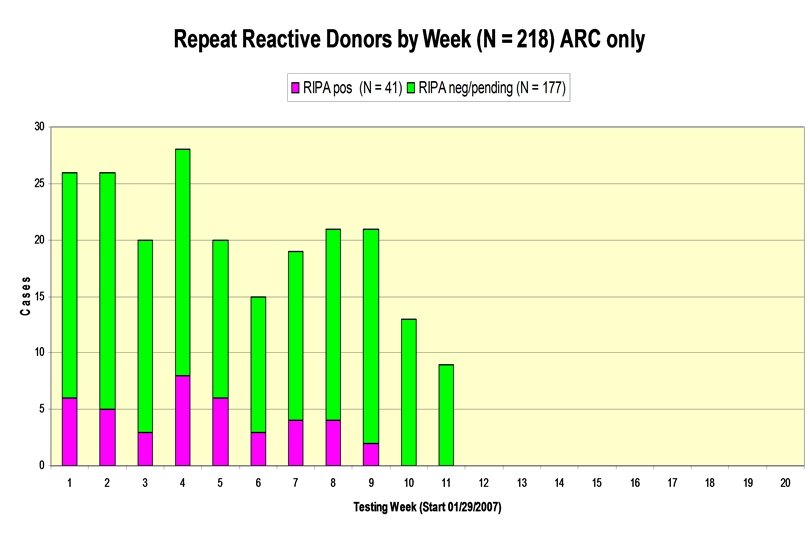
Test Performance u Clinical trial (8/28/06 -1/28/07) – PPV = 32 RIPA pos/63 RR=51%; pos in 2 states – RR rate = 63/148, 969 = 0. 042% – Prevalence = 32/148, 969 = 1: 4655 – Specificity = 148, 906 test neg/148, 906+31 false pos = 99. 979% • 99. 997% in PI u Nationwide screening (1/29/07 -4/17/07) – PPV = 50 RIPA pos/224 RR RIPA tested = 22%; pos in 17 states • 30 of 50 (60%) RIPA pos from 2 states (S CA, FL) – RR rate = 265 RRs (213 ARC + 52 BSL)/1, 757, 800 donations = 0. 015% – Projected prevalence based on 22% PPV of RIPA tested = 1: 30, 150 – Specificity (ARC) first week = 124, 934 test neg/124, 934+28 false pos = 99. 978% (6 pos) u Overall prevalence = 1: 21, 100, and 27% rate of RIPA positivity E 011375 A (03 -13 -01) 16
 N % RIPA Positive 73 29% 3. 45 0. 93 – 7.")
Samples (ARC/BSL) N % RIPA Positive 73 29% 3. 45 0. 93 – 7. 72 RIPA Negative 181 71% 1. 42 0. 82 – 3. 89 Mean S/CO Range

Variability of ELISA/RIPA u 3 samples in 10% negative gray zone that were RIPA pos u 2 samples +/- RIPA (index serum pos/neg in ret’d plasma) u Samples ELISA reactive @ index, nonrx ret’d plasma, reactive in f/u Index ELISA Plasma ELISA Follow up ELISA RIPA index RIPA plasma RIPA f/u 0. 96, 1. 2, 1. 1 0. 93, 1. 0, 0. 98 0. 85 n/a 0. 96, 0. 99 pos pos n/a pos 0. 98, 1. 05, 1. 0, 1. 1 0. 23 0. 34 n/a pos neg n/a 1. 2, 1. 3, 1. 4 0. 72 1. 43, 1. 39, 1. 43 pos pos 94% RIPA pos concordance = 30 ret’d plasma/32 index serum E 011375 A (03 -13 -01) 18

Retesting Retrieved Frozen Plasma u 51 confirmed pos donors by single to multiple RIPA => retested using ELISA or other research test; 14 -31% of low level reactivity is lost; overall 67 -84% reactivity retained Retrieved Plasma Results + Total + - Total + 34 15 49 42 7 49 - 0 2 2 1 1 2 Total Serum - 34 17 51 43 8 51 (67%) E 011375 A (03 -13 -01) 19 (31%) (84%) (14%)

Confirmatory: RIPA vs IFA u 54 RR samples (from which plasma units available for further testing) from the IND study were sent to Focus for IFA and titers if IFA pos (encouragement of S. Wendel) – 24 (44. 4%) RIPA pos; 11 IFA pos (20. 4%) – 16 discordant • 14 IFA-/RIPA + • 2 IFA+/RIPA– Overall agreement • 38/54=70. 4% *also Leish IFA reactive E 011375 A (03 -13 -01) 20 Index ELISA RIPA (x 2) 4. 3 3. 4 5. 5 3. 8 2. 7 4. 3 3. 9 0. 95 3. 5 1. 2 5. 7 5. 2 4. 0 6. 4 4. 1 2. 2 5. 9 6. 3 0. 47 2. 4 0. 7 6. 1 POS POS NEG POS (retr’d plasma) T. cruzi Ig. G IFA POS 1: 16 1: 64 1: 32 1: 16 1: 128 >1: 256 1: 16* >1: 256
 sent")
Leishmania Testing u All reactive, RIPA unconfirmed (IR in IND; RR in IVD) sent to Focus for Leishmania Ig. M/Ig. G IFA – 4 species: L. donovani, L. braziliensis, L. tropica, L. mexicana u IND: 65 IRs => 36 sent for Leish testing (index, ret’d plasma unit and follow up) – 31 RIPA neg; 5 RIPA pos (due to low level EIA; S/CO values of 0. 93 -1. 22) u IVD: 104 RRs RIPA neg to date sent for Leish testing (ret’d plasma only) E 011375 A (03 -13 -01) 21
: – 17.")
Leishmania Testing u 4 Leish pos donors (2 IND + 2 IVD): – 17. 5 yo female FT donor (CA) who was T. cruzi RIPA neg/IFA 1: 16 (+) • index 1: 32 Ig. G (L. tropica)/plasma (-); plasma 1: 16 Ig. G (L. donovani)/index (-) • Asian American; visited maternal relatives for 2 weeks in 1996 in urban areas of Brazil (mother and grandmother lived in Brazil); no travel risk for L. tropica; follow up testing negative; mother also tested negative for T. cruzi and Leishmania – 18 yo male RPT donor (CA) • plasma 1: 16 Ig. G (L. donovani)/index (-); 3 total donations • No travel risk; follow up testing negative – 71 yo female RPT donor (MA); 2 total donations; 1: 16 L. braziliensis Ig. G; no follow up – 64 yo female RPT (MI); 19 total donations; 1: 20 L. braziliensis Ig. M and 1: 40 L. donovoni Ig. M; no follow up u Likely all false pos for both T. cruzi by EIA and Leish by IFA u Recommendation; discontinue Leish following BPAC discussion E 011375 A (03 -13 -01) 22

Other Testing Results/Procedures u IND study – Follow up of 36 donors; 16 of 32 confirmed pos – 1/16 PCR positive; hemoculture pending/negative – Sample handling? ? u IVD testing; pending u “Special Protocol” for PCR and hemoculture – Increase sensitivity by having regions initiate processes • Pooling EDTA whole blood samples in guanidine/EDTA soln=>PCR (lyses cells and stabilizes kinetoplasts containing mutliple copies of DNA); store at 2 -8 C • Pooling heparinized whole blood samples, centrifuge/removal of plasma (Ab); mix buffy coat and red cells with LIT media; store at 2 -8 C • 23 samples submitted; 1 PCR pos donor to date (22 neg) E 011375 A (03 -13 -01) 23

IND Lookback Results u 32 confirmed positive donors during IND – 17 repeat donors (allogeneic/directed) – 140 prior donations => 170 components u Of 170 components – – 6 whole blood (destroyed) 3 platelets (2 destroyed, 1 transfused) 80 red cells (7 destroyed, 38 transfused, 35 pending) 81 plasma (11 destroyed, 4 transfused, 65 frac, 1 pending) u Of 1, 38 and 4 transfused components – 1 platelet recipient => deceased 11 days post transfusion – 38 red cell recipients => 15 living, 13 deceased, 10 unknown • 11 recipients tested from 8 donors (red cells transfused 7 -36 days); all ELISA/RIPA neg (7 also PCR neg) – 4 plasma recipients => deceased E 011375 A (03 -13 -01) 24

IVD Lookback Results u 41 confirmed positive donors since licensed test implemented – 21 repeat donors (allogeneic/directed) – 171 prior donations => 108 components (reported to date) u Of 108 components – – 17 platelets (6 destroyed, 6 transfused, 5 unknown) 49 red cells (1 destroyed, 9 transfused, 39 pending) 41 plasma (1 destroyed, 2 transfused, 27 frac, 11 pending) 1 cryo (1 pending) u Of 6, 9 and 2 transfused components – 6 platelet recipients => 5 deceased, 1 living => ELISA and PCR neg (RIPA pending) – 9 red cell recipients => 6 deceased, 1 unknown; 2 living => ELISA, RIPA and PCR neg (RIPA pending on one) – 2 plasma recipients => 2 living => ELISA neg (RIPA and PCR pending) E 011375 A (03 -13 -01) 25

Lookback Summary u Recipients from 10 RIPA pos donors tested u IND – 11 red cell recipients tested from 8 donors u IVD – 1 platelet recipient tested from 1 donor – 2 red cell recipients tested from same donor – 2 plasma recipients tested from 1 donor u Total 16 recipients test negative to date E 011375 A (03 -13 -01) 26

Lookback Significance u Lookback case summary – platelets/whole blood, considered to be highest risk – – 1 of 4 Leiby LA and Miami (NEJM 1999) 4 of 9 Kirchhoff Mexico (Transfusion 2006) 0 of 1 Stramer (IVD, unpub) 5 of 14 = 36% u Why not higher? – – Donor must be parasitemic (intermittent) Parasites must remain viable/infectious in component during processing/handling – Acute infections are most frequently recognized in immunosuppressed patients E 011375 A (03 -13 -01) 27

Donor Demographics u 61 RR IND ARC donors – 32 RIPA pos • 14 FT, 18 RPT • 19 male, 13 female • 17 -84 yo (mean 47 yo; median 50 yo) • 30 allo, 1 auto, 1 platelet pheresis • Countries represented (15 donor surveys received); 11/15 endemic areas: Mexico (5), US (4), El Salvador (2), Bolivia (2), Guatemala (1), Argentina (1) u 213 RR IVD ARC donors – 41 RIPA pos • 20 FT, 21 RPT • 26 male, 15 female • 39 allo, 1 auto, 1 directed (FT male) • Countries represented (10 donor surveys received); 9/10 endemic areas: Mexico (4), El Salvador (3), Brazil (1), Bolivia (1), US (1) E 011375 A (03 -13 -01) 28
 RIPA pos")
Donor Demographics u 52 RR IVD UBS donors – 7 + (2) RIPA pos • 6 FT, 3 RPT • 8 males, 1 female • 7 allo, 1 platelet pheresis, 1 auto • Countries represented: Mexico (4), El Salvador (2), Guatemala (1) Venezuela (1) (1 unknown) u Total 328 RR donors – 82 RIPA pos • 40 FT, 42 RPT • 53 males, 29 females • 76 allo, 2 platelet pheresis, 3 auto, 1 directed • Countries represented (N=33): Mexico (13), El Salvador (7), US (5), Bolivia (3), Guatemala (2), Venezuela (1), Argentina (1) Brazil (1) • 28/33 (85%) endemic areas vs 28/28 controls from nonendemic (US + 1 China) E 011375 A (03 -13 -01) 29
 Born/Lived Endemic Country Years in Endemic Country Mother Endemic Country Rural")
Gender Age (yrs) Born/Lived Endemic Country Years in Endemic Country Mother Endemic Country Rural Residence Endemic Country Cardiac/GI Symptoms F F (runner) M 50 60 El Salvador US only 35 n/a Y N Thatched roof N Racing heartbeat 50 Bolivia 6 Y N None M 57 Mexico 11 Y N None F (vet) 64 n/a N N Irreg heartbeat M 76 US born/lived in Mexico 29 Y N Swollen ankles F (LB) 34 El Salvador 29 Y Thatched roof; mud floors, bitten Visible neck veins M 39 Bolivia 11 Thatched roof; mud floors, bitten F 66 Guatemala 27 Y (w/cardiac symptoms) Y F 57 US only n/a N None, but yes for maternal family Extra heart sounds None F (PCR+) 29 Mexico 15 Y Thatched roof; mud floors None M 59 Mexico 19 Y Thatched roof; mud floors, bitten ECG irreg, diff. breathing M 42 Mexico 21 Y Mud floors Sticking sens esophagus, stomach E 011375 A (03 -13 -01) 30 Thatched roof; mud floors N
 Born/Lived Endemic Country Years in Endemic Country Mother Endemic Country Rural")
Gender Age (yrs) Born/Lived Endemic Country Years in Endemic Country Mother Endemic Country Rural Residence Endemic Country Cardiac/GI Symptoms M 57 Argentina 12 Y N Racing heartbeat F (preg; f/u CDC) M 33 El Salvador 18 Y N 75 Mexico 20 Y Dirt floor ECG irreg; multiple other Shortness breath F (6 56 Mexico 19 Y Dirt floor Shortness breath M (PCR+) F 27 El Salvador 18 Y N 42 Mexico 33 Y F 57 Brazil 46 Y (w/cardiac symptoms) Y ECG irreg; multiple other Shortness of breath M 57 El Salvador 33 Y F 33 Bolivia 3 Y (w/cardiac symptoms) M 50 US only n/a M 28 Mexico 17 children tested neg) E 011375 A (03 -13 -01) 31 Thatched roof; mud floors N Shortness of breath ECG irreg; multiple other Shortness of breath N n/a Trouble swallowing Y Dirt floor Racing heartbeat
 runner in Griffith Park –")
Possible Autochthonous Cases u u 61 yo female (CA) runner in Griffith Park – Griffith park zoo and other animals demonstrated to harbor T. cruzi (6 sp of triatomine bugs in CA; 18 mammal species are reservoirs) – Lived in LA entire life, high quality housing – Travel outside of the US • Time share in Cancun where she spends a week 1990 -1999; no camping 64 yo female (AZ) retired vet – Lived in rural Mexico where she volunteered as a vet/exposure to infectious material 57 yo female (CA) lives in rural area – Rural area recovering from fire damage – Has many pets and frequently sees raccoons, opossums, skunks on her property and adjacent property, also gardens on her property – Lived in LA entire life, high quality housing – Multiple transfusions in 1971 in CA – Asymptomatic 50 yo male (AR) – Lived in US entire life; one trip to Nassau – Asymptomatic – Only possible “risk” is time spend in Corpus Christi, TX where he slept outside for several weeks E 011375 A (03 -13 -01) 32

Summary and Conclusions u Prevalence 1: 21, 100 – 82 RIPA pos donors from 328 RR donors in 17 states during IND/IVD testing of >1. 9 million donations – 60% from California and Florida u Leishmania – Adds no value; only confusion! u Lookback (to date) – 60 transfused components from 278 mfg’d from 38 RIPA pos donors – 16 recipients tested neg from 10 donors; only 1 platelet recipient u Donor Demographics – 28/33 (85%) endemic areas vs 28/28 controls from nonendemic (US + 1 China) – 5 possible autochthonous cases; time of infection unknown E 011375 A (03 -13 -01) 33

Acknowledgements u American Red Cross – – – – – E 011375 A (03 -13 -01) 34 Greg Foster, SSO David Leiby, HL Roger Dodd, HL Ross Herron, West Div Pamela Kahm, West Div Norma Espinoza, West Div Kay Crull, West Div Muriel Nelson, IT Mike Savin, IT u Blood Systems Laboratories – – – Sally Caglioti Frank Radar Larry Morgan u Ortho Clinical Diagnostics – – – Cheryl Vitow Cindy Ballas Brian Mc. Donough
c7b95fc4703ff039256edd662bb25f15.ppt