

22cc0cd3d4250cb734cb3eb42e7748c7.ppt
- Количество слайдов: 132
 Issues in Transgender Primary Care Carol F. Milazzo, MD, FAAP Vice Chair, Dept. of Pediatrics Sutter Roseville Medical Center World Professional Assn. For Transgender Health Samuel Merritt University 27 Feb 2011
Issues in Transgender Primary Care Carol F. Milazzo, MD, FAAP Vice Chair, Dept. of Pediatrics Sutter Roseville Medical Center World Professional Assn. For Transgender Health Samuel Merritt University 27 Feb 2011
 Faculty Disclosure § I have no personal financial relationship with any entity producing, marketing, re-selling or distributing health care goods or services consumed by, or used on, patients. § The pharmaceutical treatments discussed are used in accordance with professional consensus represented by the WPATH Standards of Care, but may not have US FDA approval for these indications.
Faculty Disclosure § I have no personal financial relationship with any entity producing, marketing, re-selling or distributing health care goods or services consumed by, or used on, patients. § The pharmaceutical treatments discussed are used in accordance with professional consensus represented by the WPATH Standards of Care, but may not have US FDA approval for these indications.
 Biography § 1983 -86 – Staff Pediatrician, US Naval Hospital, Roosevelt Roads, PR § 1987 -99 – Assistant Professor in Pediatrics, Creighton University & Univ. of Nebraska § 2000 -present – Solo practice, Roseville, CA § Fellow American Academy of Pediatrics, Member WPATH, IFGE, GLMA
Biography § 1983 -86 – Staff Pediatrician, US Naval Hospital, Roosevelt Roads, PR § 1987 -99 – Assistant Professor in Pediatrics, Creighton University & Univ. of Nebraska § 2000 -present – Solo practice, Roseville, CA § Fellow American Academy of Pediatrics, Member WPATH, IFGE, GLMA
 § ~5, 000 active patients") Practice Description § 1500 sq. ft. (140 m 2) § ~5, 000 active patients § ~300 adolescent & young adult transgender patients (ages 5 -40 yrs), FTM/MTF ≈ 1: 1 § Average 6 -7 new referrals/mo. (↑ since 2007) § Practitioners: 1 MD + 1 NP + support staff
Practice Description § 1500 sq. ft. (140 m 2) § ~5, 000 active patients § ~300 adolescent & young adult transgender patients (ages 5 -40 yrs), FTM/MTF ≈ 1: 1 § Average 6 -7 new referrals/mo. (↑ since 2007) § Practitioners: 1 MD + 1 NP + support staff

 Query posted on online pediatric discussion group § “I have seen an increasing number of youths referred by mental health professionals for initiation and medical supervision of cross gender hormone treatment. I wonder if others have had similar experiences. ” -cfm
Query posted on online pediatric discussion group § “I have seen an increasing number of youths referred by mental health professionals for initiation and medical supervision of cross gender hormone treatment. I wonder if others have had similar experiences. ” -cfm
 Responses to query § “I find your post disturbing. Surely young adolescents are not given hormone treatments for this purpose. I hope you are not participating in this type of ‘treatment. ’”
Responses to query § “I find your post disturbing. Surely young adolescents are not given hormone treatments for this purpose. I hope you are not participating in this type of ‘treatment. ’”
 Responses to query § “…this involves minors, and adolescents are often confused about their sexuality. Many [youths engage] in same-gender sex experimentation and this may contribute to confusion. ”
Responses to query § “…this involves minors, and adolescents are often confused about their sexuality. Many [youths engage] in same-gender sex experimentation and this may contribute to confusion. ”
 Responses to query § “The ‘mental health professionals’ sending you these patients need mental health evaluations themselves!”
Responses to query § “The ‘mental health professionals’ sending you these patients need mental health evaluations themselves!”
 Responses to query § “As child psychiatrist I think that my mission is not to … satisfy pathologic desires, even if patients say they would be better. ”
Responses to query § “As child psychiatrist I think that my mission is not to … satisfy pathologic desires, even if patients say they would be better. ”
 Responses to query § “I don’t understand why the medical profession has to assist people mutilating themselves into the physical appearance of the other sex. This is especially true of a minor. ”
Responses to query § “I don’t understand why the medical profession has to assist people mutilating themselves into the physical appearance of the other sex. This is especially true of a minor. ”
 Responses to query § “I profess my ignorance of the literature in this arena, but have an innate suspicion and caution re. study bias (a la Kinsey Report). ”
Responses to query § “I profess my ignorance of the literature in this arena, but have an innate suspicion and caution re. study bias (a la Kinsey Report). ”
 Responses to query § “I remain unconvinced of the appropriateness of this intervention. HBIGDA appears to be primarily a political advocacy organization. Treatments this drastic should be based on good science, not political beliefs. ”
Responses to query § “I remain unconvinced of the appropriateness of this intervention. HBIGDA appears to be primarily a political advocacy organization. Treatments this drastic should be based on good science, not political beliefs. ”
 Response to responses § “Not everyone may feel comfortable or competent with such issues, but we should recognize them, their seriousness, and learn to refer them to our colleagues who are experienced and willing to care for these patients. ” -cfm
Response to responses § “Not everyone may feel comfortable or competent with such issues, but we should recognize them, their seriousness, and learn to refer them to our colleagues who are experienced and willing to care for these patients. ” -cfm
 Spectrum of Attitudes among health professionals § These responses to the query demonstrate a range of attitudes and misconceptions about the treatment of transgender youth. Professional ignorance and bias pose significant barriers to access to competent and sensitive health care for these patients.
Spectrum of Attitudes among health professionals § These responses to the query demonstrate a range of attitudes and misconceptions about the treatment of transgender youth. Professional ignorance and bias pose significant barriers to access to competent and sensitive health care for these patients.
 Objectives § Recognize health care issues that transgenders face. § Understand diagnosis and clinical management of gender dysphoria. § Identify resources for health professionals serving transgenders.
Objectives § Recognize health care issues that transgenders face. § Understand diagnosis and clinical management of gender dysphoria. § Identify resources for health professionals serving transgenders.
 Definitions § Transgender = Gender variant – individuals whose gender expression or identification differs from culturally assigned expectations and stereotypes based on anatomic sex.
Definitions § Transgender = Gender variant – individuals whose gender expression or identification differs from culturally assigned expectations and stereotypes based on anatomic sex.
 Joan of Arc
Joan of Arc
 Ru. Paul
Ru. Paul
 Boy George
Boy George
 Prince Charles Evzones
Prince Charles Evzones
 Utilikilts
Utilikilts
 Rosie the Riveter
Rosie the Riveter
 Rosie the Riveter Bob the Builder
Rosie the Riveter Bob the Builder
 Definitions § Transsexual – A subset of transgender individuals that seeks conformity of the body with their gender identity through medical (hormone) and/or surgical means.
Definitions § Transsexual – A subset of transgender individuals that seeks conformity of the body with their gender identity through medical (hormone) and/or surgical means.
 Definitions § Note Gender identity and expression are independent of sexual orientation.
Definitions § Note Gender identity and expression are independent of sexual orientation.
 in Adolescents or Adults – 302. 85*") Diagnostic Criteria GID Gender Identity Disorder (GID) in Adolescents or Adults – 302. 85* § A strong and persistent cross-gender identification (not merely a desire for any perceived cultural advantages of being the other sex).
Diagnostic Criteria GID Gender Identity Disorder (GID) in Adolescents or Adults – 302. 85* § A strong and persistent cross-gender identification (not merely a desire for any perceived cultural advantages of being the other sex).
 Diagnostic Criteria GID § Persistent discomfort with his or her sex or sense of inappropriateness in the gender role of that sex. (Gender dysphoria). § The disturbance is not concurrent with a physical intersex condition.
Diagnostic Criteria GID § Persistent discomfort with his or her sex or sense of inappropriateness in the gender role of that sex. (Gender dysphoria). § The disturbance is not concurrent with a physical intersex condition.
 Diagnostic Criteria GID § The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. * Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, APA, 2000.
Diagnostic Criteria GID § The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. * Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, APA, 2000.
 DSM-5 Gender Incongruence § A marked incongruence between one’s experienced/expressed gender and assigned gender, of at least 6 months duration as manifested by 2 or more of the following indicators
DSM-5 Gender Incongruence § A marked incongruence between one’s experienced/expressed gender and assigned gender, of at least 6 months duration as manifested by 2 or more of the following indicators
 DSM-5 Gender Incongruence § A strong desire for the primary and/or secondary characteristics of the other gender § A strong desire to be treated as the other gender
DSM-5 Gender Incongruence § A strong desire for the primary and/or secondary characteristics of the other gender § A strong desire to be treated as the other gender
 DSM-5 Gender Incongruence § Incongruence between experienced expressed gender and primary or secondary sex characteristics § A strong desire to be rid of one’s primary and/or secondary sex characteristics § A strong conviction that one has the typical feelings and reactions of the other gender
DSM-5 Gender Incongruence § Incongruence between experienced expressed gender and primary or secondary sex characteristics § A strong desire to be rid of one’s primary and/or secondary sex characteristics § A strong conviction that one has the typical feelings and reactions of the other gender
 GID in Children DSM-IV 302. 6* § GID in prepubertal children has more variable outcome than in adolescents or adults. Some have gender dysphoria that resolves spontaneously. Therefore these children should not be offered physical treatment nor surgery… * Cohen-Kettenis & Pfafflin, 2003
GID in Children DSM-IV 302. 6* § GID in prepubertal children has more variable outcome than in adolescents or adults. Some have gender dysphoria that resolves spontaneously. Therefore these children should not be offered physical treatment nor surgery… * Cohen-Kettenis & Pfafflin, 2003
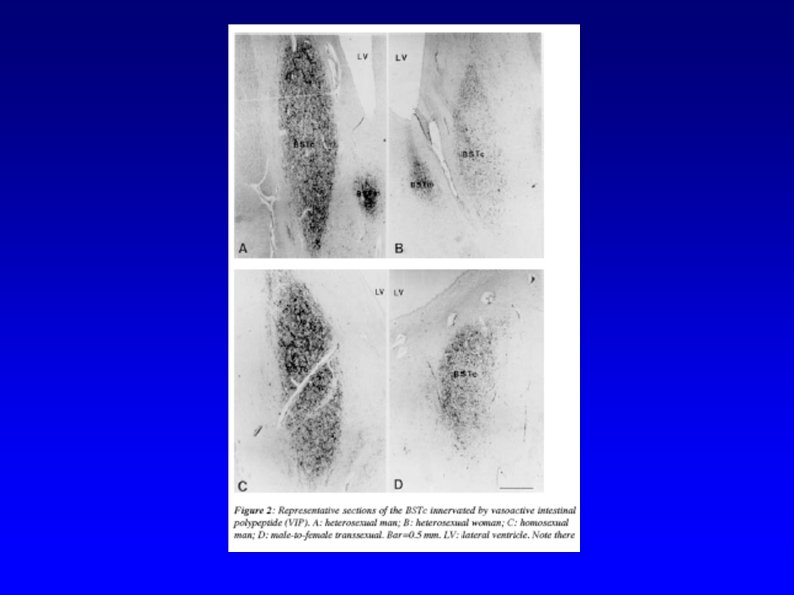
 Etiology § Nature vs. nurture? § Anatomic evidence § BSTc § 2 D: 4 D Ratios
Etiology § Nature vs. nurture? § Anatomic evidence § BSTc § 2 D: 4 D Ratios

 2 D: 4 D Ratio 2 D < 4 D Male ♂ 2 D ≥ 4 D Female ♀
2 D: 4 D Ratio 2 D < 4 D Male ♂ 2 D ≥ 4 D Female ♀
 ratios in") Typical female 2 nd– 4 th finger length (2 D: 4 D) ratios in male-to-female transsexuals—possible implications for prenatal androgen exposure Harald J. Schneider, Johanna Pickel and Günter K. Stalla Clinical Neuroendocrinology Group, Max Planck Institute of Psychiatry, Kraepelinstrasse 10, 80804 Munich, Germany Abstract Prenatal exposure to androgens has been implicated in transsexualism but the etiology of the condition remains unclear. The ratio of the 2 nd to the 4 th (2 D: 4 D) digit lengths has been suggested to be negatively correlated to prenatal androgen exposure. We wanted to assess differences in 2 D: 4 D ratio between transsexuals and controls. Sixty-three male-to-female transsexuals (MFT), 43 female-to-male transsexuals (FMT), and 65 female and 58 male controls were included in the study. Photocopies of the palms and digits of the hands were taken of all subjects and 2 D: 4 D ratios were measured, according to standard published procedures. Comparison between right-handed individuals revealed that the right-hand 2 D: 4 D in MFT is higher than in control males but similar to that observed in control females. In FMT we found no differences in 2 D: 4 D relative to control females. Our findings support a biological etiology of male-to-female transsexualism, implicating decreased prenatal androgen exposure in MFT. We have found no indication of a role of prenatal hormone exposure in female-to-male transsexualism. Psychoneuroendocrinology Volume 31, Issue 2, February 2006, Pages 265 -269
Typical female 2 nd– 4 th finger length (2 D: 4 D) ratios in male-to-female transsexuals—possible implications for prenatal androgen exposure Harald J. Schneider, Johanna Pickel and Günter K. Stalla Clinical Neuroendocrinology Group, Max Planck Institute of Psychiatry, Kraepelinstrasse 10, 80804 Munich, Germany Abstract Prenatal exposure to androgens has been implicated in transsexualism but the etiology of the condition remains unclear. The ratio of the 2 nd to the 4 th (2 D: 4 D) digit lengths has been suggested to be negatively correlated to prenatal androgen exposure. We wanted to assess differences in 2 D: 4 D ratio between transsexuals and controls. Sixty-three male-to-female transsexuals (MFT), 43 female-to-male transsexuals (FMT), and 65 female and 58 male controls were included in the study. Photocopies of the palms and digits of the hands were taken of all subjects and 2 D: 4 D ratios were measured, according to standard published procedures. Comparison between right-handed individuals revealed that the right-hand 2 D: 4 D in MFT is higher than in control males but similar to that observed in control females. In FMT we found no differences in 2 D: 4 D relative to control females. Our findings support a biological etiology of male-to-female transsexualism, implicating decreased prenatal androgen exposure in MFT. We have found no indication of a role of prenatal hormone exposure in female-to-male transsexualism. Psychoneuroendocrinology Volume 31, Issue 2, February 2006, Pages 265 -269
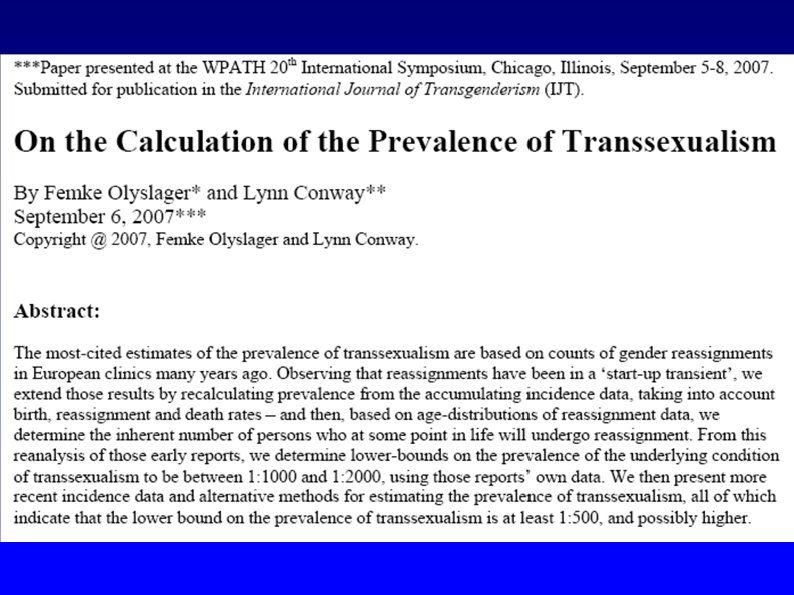
 Prevalence § Old estimate 1: 30, 000 § New estimate 1: 1000 – 1: 2000
Prevalence § Old estimate 1: 30, 000 § New estimate 1: 1000 – 1: 2000
 Prevalence in Adolescents § There is no epidemiological data for this age group § The observed sex ratio in adolescents approaches 1: 1
Prevalence in Adolescents § There is no epidemiological data for this age group § The observed sex ratio in adolescents approaches 1: 1
 Health Care Issues* § Societal marginalization § Internalization of stigma § Gender dysphoria § Risk taking behaviors * An Overview of U. S. Trans Health Priorities: A Report by the Disparities Working Group of the National Coalition for LGBT Health, August, 2004
Health Care Issues* § Societal marginalization § Internalization of stigma § Gender dysphoria § Risk taking behaviors * An Overview of U. S. Trans Health Priorities: A Report by the Disparities Working Group of the National Coalition for LGBT Health, August, 2004
 Societal Marginalization Trans youth experiences in school* § Gender-based verbal harassment 96% § Gender-based physical harassment 83% § Did not feel safe in school 75% § Dropped out of school 75% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
Societal Marginalization Trans youth experiences in school* § Gender-based verbal harassment 96% § Gender-based physical harassment 83% § Did not feel safe in school 75% § Dropped out of school 75% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
 Societal Marginalization § Barriers to health access § Unemployment § Depression § Educational deficiencies, § Discrimination by employers, § ID incompatibility with presenting gender.
Societal Marginalization § Barriers to health access § Unemployment § Depression § Educational deficiencies, § Discrimination by employers, § ID incompatibility with presenting gender.
 Societal Marginalization Homelessness § § Rejection by family § Lack of income § Discrimination in housing § Lack of accommodation by homeless shelters
Societal Marginalization Homelessness § § Rejection by family § Lack of income § Discrimination in housing § Lack of accommodation by homeless shelters
 Internalization of Stigma § Thoughts of suicide 83% § Attempted suicide 54% § Self mutilation 21% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
Internalization of Stigma § Thoughts of suicide 83% § Attempted suicide 54% § Self mutilation 21% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
 Gender dysphoria § Engaged in body modification 88% § Engaged in hormone therapy 25% § Received silicone injections 8% § Intend to acquire hormones and/or undergo surgery in the future 33% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
Gender dysphoria § Engaged in body modification 88% § Engaged in hormone therapy 25% § Received silicone injections 8% § Intend to acquire hormones and/or undergo surgery in the future 33% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
 Risk taking behaviors § Engaged in sex work 46% § Alcohol use 75% § Illegal drug use 79% § Sold illegal drugs 21% § Sex under influence of alcohol 96% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
Risk taking behaviors § Engaged in sex work 46% § Alcohol use 75% § Illegal drug use 79% § Sold illegal drugs 21% § Sex under influence of alcohol 96% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
 Risk taking behaviors § Sex under influence of illegal drugs 75% § Reported being HIV positive 13% § Reported an STD 17% § Engaged in risk behaviors for HIV transmission 96% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
Risk taking behaviors § Sex under influence of illegal drugs 75% § Reported being HIV positive 13% § Reported an STD 17% § Engaged in risk behaviors for HIV transmission 96% * A qualitative study of trans youth in Philadelphia, n=24, age range 16 -21, Lydia Sausa, Ph. D. , 2003
 Barriers to Access - Provider COMPETENCE § Lack of recognition of condition, its morbidity § Lack of treatment knowledge and skills BIAS § Reluctance/refusal to serve transgenders § Insensitivity of provider/staff § Institutional bias EXCLUSION OF CONDITION BY INSURANCE
Barriers to Access - Provider COMPETENCE § Lack of recognition of condition, its morbidity § Lack of treatment knowledge and skills BIAS § Reluctance/refusal to serve transgenders § Insensitivity of provider/staff § Institutional bias EXCLUSION OF CONDITION BY INSURANCE
 Barriers to Access - Patient § Lack of support or hostility of parents/peers § Poor self esteem/depression § Mistrust of providers § Low socioeconomic status § § § Lack of transportation Lack of health insurance, finances Exclusion of condition by insurance
Barriers to Access - Patient § Lack of support or hostility of parents/peers § Poor self esteem/depression § Mistrust of providers § Low socioeconomic status § § § Lack of transportation Lack of health insurance, finances Exclusion of condition by insurance
 Tasks § Professional education § Networking § Practice accommodation
Tasks § Professional education § Networking § Practice accommodation
 Professional Education § STRENGTH: Medical school and residency training curricula include the principles of endocrinology. § WEAKNESS: These curricula do not include transgender health care.
Professional Education § STRENGTH: Medical school and residency training curricula include the principles of endocrinology. § WEAKNESS: These curricula do not include transgender health care.
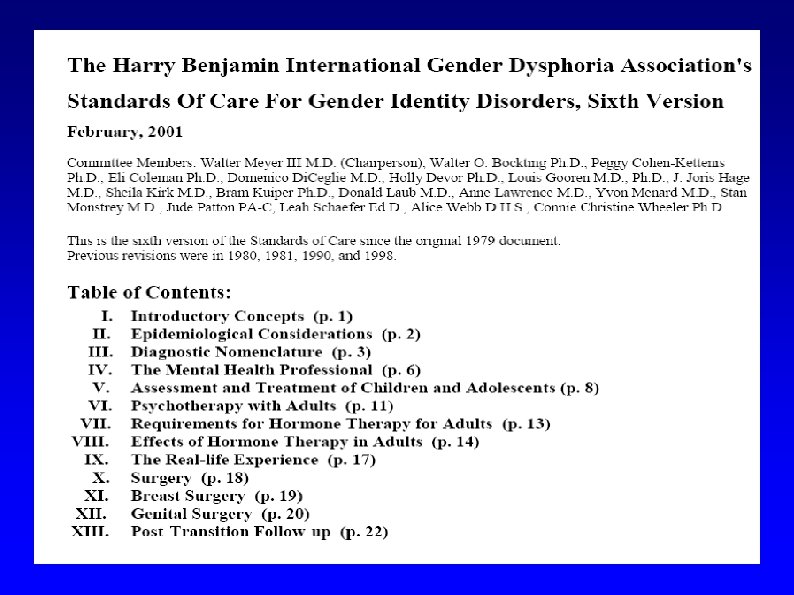
 Standards of Care, Sixth Version") Professional Education: Opportunities § The WPATH (formerly HBIGDA) Standards of Care, Sixth Version
Professional Education: Opportunities § The WPATH (formerly HBIGDA) Standards of Care, Sixth Version
 § http: //www. wpath. org/ publications_standards. cfm § Online") WPATH Standards of Care (SOC) § http: //www. wpath. org/ publications_standards. cfm § Online in English, Spanish and Croatian translations § De facto authoritative consensus, in constant revision
WPATH Standards of Care (SOC) § http: //www. wpath. org/ publications_standards. cfm § Online in English, Spanish and Croatian translations § De facto authoritative consensus, in constant revision
 §") Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism
Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism
 §") Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols
Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols
 Published Clinical Protocols Online § § Anne Lawrence, M. D. § Callen-Lorde Community Health Center (NY) § Vancouver Coastal Health Transgender Health Program § Tom Waddell Health Center (SF)
Published Clinical Protocols Online § § Anne Lawrence, M. D. § Callen-Lorde Community Health Center (NY) § Vancouver Coastal Health Transgender Health Program § Tom Waddell Health Center (SF)
 Published Clinical Protocols § de Vries, A. , Cohen-Kettenis, P. , Delemarre-van der Waal, H. “Clinical Management of Gender Dysphoria in Adolescents. ” IJT 9. 3/4 (2006): 83 -94.
Published Clinical Protocols § de Vries, A. , Cohen-Kettenis, P. , Delemarre-van der Waal, H. “Clinical Management of Gender Dysphoria in Adolescents. ” IJT 9. 3/4 (2006): 83 -94.
 Published Clinical Protocols § Ettner R, Monstrey S, Eyler A, eds. Principles of Transgender Medicine and Surgery, Haworth, 2007.
Published Clinical Protocols § Ettner R, Monstrey S, Eyler A, eds. Principles of Transgender Medicine and Surgery, Haworth, 2007.
 §") Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings
Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings
 Professional meetings § WPATH Symposia § National and international professional societies
Professional meetings § WPATH Symposia § National and international professional societies
 §") Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings § Peer discussion
Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings § Peer discussion
 Peer discussion § Online discussion groups, e. g. Yahoo! Transmedicine, Trans youth clinical support, Transhealthalliance, etc. § Consults among local gender team members
Peer discussion § Online discussion groups, e. g. Yahoo! Transmedicine, Trans youth clinical support, Transhealthalliance, etc. § Consults among local gender team members
 §") Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings § Peer discussion § Academic curricula
Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings § Peer discussion § Academic curricula
 Academic curricula § AMA: “In June 2007, the AMA House of Delegates voted to revise current AMA policies to ensure inclusion and protection for transgender physicians, medical students and patients. ”
Academic curricula § AMA: “In June 2007, the AMA House of Delegates voted to revise current AMA policies to ensure inclusion and protection for transgender physicians, medical students and patients. ”
 Academic curricula § American Medical Student Association: LGBT Health Action Committee § GLMA: Trans Health Care Committee
Academic curricula § American Medical Student Association: LGBT Health Action Committee § GLMA: Trans Health Care Committee
 §") Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings § Peer discussion § Academic curricula § Local education opportunities
Professional Education: Opportunities § The WPATH Standards of Care, Sixth Version (formerly HBIGDA) § The International Journal of Transgenderism § Published Clinical Protocols § Professional meetings § Peer discussion § Academic curricula § Local education opportunities
 Local education opportunities § Educate local clinicians* § Present at local grand rounds
Local education opportunities § Educate local clinicians* § Present at local grand rounds
 Networking FACILITATES: § Consultation with colleagues § Referral of patients to/from other gender team members § Patient access
Networking FACILITATES: § Consultation with colleagues § Referral of patients to/from other gender team members § Patient access
 Networking § Join WPATH, IFGE, national societies § Network and advocate for transgender care inclusion within specialty societies § Contact/speak at community organizations, e. g. , PFLAG, gender support groups § Join or form a local team of gender professionals
Networking § Join WPATH, IFGE, national societies § Network and advocate for transgender care inclusion within specialty societies § Contact/speak at community organizations, e. g. , PFLAG, gender support groups § Join or form a local team of gender professionals
 The SOC Gender Team Model MEDICAL DOCTOR THERAPIST PATIENT SURGEON
The SOC Gender Team Model MEDICAL DOCTOR THERAPIST PATIENT SURGEON
 Forming a Local Gender Team § Ask patients about local providers § Contact local LGBT community center/transgender support groups § Contact professional organizations, e. g. , WPATH, IFGE § Web searches, WPATH and GLMA online provider databases
Forming a Local Gender Team § Ask patients about local providers § Contact local LGBT community center/transgender support groups § Contact professional organizations, e. g. , WPATH, IFGE § Web searches, WPATH and GLMA online provider databases
 Networking § Advertising – practice web site
Networking § Advertising – practice web site
 Practice website § Provides descriptive and useful information on health management, introduction to staff, practice flavor and policies. www. cfmilazzo. com
Practice website § Provides descriptive and useful information on health management, introduction to staff, practice flavor and policies. www. cfmilazzo. com
 Networking § Advertising – practice web site § Letterhead* and Business cards
Networking § Advertising – practice web site § Letterhead* and Business cards
 Children Adolescents Young Adults Carol F. Milazzo, MD 406 Sunrise Ave, Ste 280 Roseville, CA 95661 Tel. (916) 782 -3786 Special interest in: Attention Deficit Disorders Autism Spectrum Disorders Gender Dysphoria Fellow, American Academy of Pediatrics Member, Sacramento Pediatric Society International Foundation for Gender Education World Professional Association for Transgender Health
Children Adolescents Young Adults Carol F. Milazzo, MD 406 Sunrise Ave, Ste 280 Roseville, CA 95661 Tel. (916) 782 -3786 Special interest in: Attention Deficit Disorders Autism Spectrum Disorders Gender Dysphoria Fellow, American Academy of Pediatrics Member, Sacramento Pediatric Society International Foundation for Gender Education World Professional Association for Transgender Health
 Practice Accommodation Staff sensitivity Patient comfort
Practice Accommodation Staff sensitivity Patient comfort
 Staff sensitivity - complaints § “The doctor said I could never pass as a woman with all my tattoos. ” - MTF § “I overheard the doctor repeatedly refer to me as ‘he’ when addressing his staff. ” – MTF § Perception of the provider/staff as judgmental or adversarial may interfere with patient compliance and safety
Staff sensitivity - complaints § “The doctor said I could never pass as a woman with all my tattoos. ” - MTF § “I overheard the doctor repeatedly refer to me as ‘he’ when addressing his staff. ” – MTF § Perception of the provider/staff as judgmental or adversarial may interfere with patient compliance and safety
 Staff sensitivity education § Ask patient about preferred pronouns & use them when addressing the patient § When in doubt, ask! Do not make assumptions based on observed gender cues § Be non-judgmental
Staff sensitivity education § Ask patient about preferred pronouns & use them when addressing the patient § When in doubt, ask! Do not make assumptions based on observed gender cues § Be non-judgmental
 §") Patient comfort § Offer appointments at convenient times for patient (and family/significant others) § Reserve exam rooms & times that avoid uncomfortable situations with other patients
Patient comfort § Offer appointments at convenient times for patient (and family/significant others) § Reserve exam rooms & times that avoid uncomfortable situations with other patients
 Patient comfort § Have a gender-neutral restroom § “This is a SAFE Place” posters – GLSEN, PFLAG
Patient comfort § Have a gender-neutral restroom § “This is a SAFE Place” posters – GLSEN, PFLAG
 Patient comfort § Intake forms—provide for preferred pronoun, preferred name, gender other than M or F
Patient comfort § Intake forms—provide for preferred pronoun, preferred name, gender other than M or F
 HISTORY WORKSHEET Carol F. Milazzo, M. D. To help us better serve you, please fill out this form before your exam. Patient preferred name: Patient legal name: Birthdate: Age: Gender [ ] M [ ] F [ ] Other Primary care physician Preferred pronoun: Phone Address Therapist Address Phone When started therapy MEDICAL HISTORY: Please list all current and past medications and herbal preparations and duration Please list all medication allergies
HISTORY WORKSHEET Carol F. Milazzo, M. D. To help us better serve you, please fill out this form before your exam. Patient preferred name: Patient legal name: Birthdate: Age: Gender [ ] M [ ] F [ ] Other Primary care physician Preferred pronoun: Phone Address Therapist Address Phone When started therapy MEDICAL HISTORY: Please list all current and past medications and herbal preparations and duration Please list all medication allergies
 Physician Encounter Patient types: § § Referred by gender therapist § Self-referred § § § Initial inquiry about treatment resources Self-medicating (harm reduction) Full, partial or no gender reassignment
Physician Encounter Patient types: § § Referred by gender therapist § Self-referred § § § Initial inquiry about treatment resources Self-medicating (harm reduction) Full, partial or no gender reassignment
 Physician Encounter § Patient centered § Collaborate with patient in treatment planning § Discuss patient goals, eligibility criteria, treatment options, expectations, risks, benefits and alternatives
Physician Encounter § Patient centered § Collaborate with patient in treatment planning § Discuss patient goals, eligibility criteria, treatment options, expectations, risks, benefits and alternatives
 Sex Steroids Sex hormones are steroids, a class of molecules derived from cholesterol. Cholesterol
Sex Steroids Sex hormones are steroids, a class of molecules derived from cholesterol. Cholesterol
 Testosterone Estradiol
Testosterone Estradiol
 Sex Hormone Mechanism of Action
Sex Hormone Mechanism of Action
 Regulation of Sex Hormones Hypothalamus Gn. RH - - + + - Pituitary FSH LH - + + - Gonad Testosterone or Estradiol/Progesterone -
Regulation of Sex Hormones Hypothalamus Gn. RH - - + + - Pituitary FSH LH - + + - Gonad Testosterone or Estradiol/Progesterone -
 Male P 1 P 2 P 3 P 4 P 5") Pubertal Stages (Tanner) Male P 1 P 2 P 3 P 4 P 5 Prepubertal, testicular length less than 2. 5 cm early increase in testicular size, scrotum slightly pigmented, few long and dark pubic hair testicular length 3. 3 -4 cm, lengthening of the penis, increase in pubic hair testicular length 4. 1 -4. 5 cm, increase in length and thickening of the penis, adult amount of pubic hair testicular length greater than 4. 5 cm, full sperm production
Pubertal Stages (Tanner) Male P 1 P 2 P 3 P 4 P 5 Prepubertal, testicular length less than 2. 5 cm early increase in testicular size, scrotum slightly pigmented, few long and dark pubic hair testicular length 3. 3 -4 cm, lengthening of the penis, increase in pubic hair testicular length 4. 1 -4. 5 cm, increase in length and thickening of the penis, adult amount of pubic hair testicular length greater than 4. 5 cm, full sperm production
 Female P 1 P 2 P 3 P 4 P 5") Pubertal Stages (Tanner) Female P 1 P 2 P 3 P 4 P 5 Prepubertal Early development of subareolar breast bud +/- small amounts of pubic hair and axillary hair Increase in size of palpable breast tissue and areolae, increased amount of dark pubic hair and of axillary hair Further increase in breast size and areolae that protrude above breast level adult pubic hair Adult stage, pubic hair with extension to upper thigh
Pubertal Stages (Tanner) Female P 1 P 2 P 3 P 4 P 5 Prepubertal Early development of subareolar breast bud +/- small amounts of pubic hair and axillary hair Increase in size of palpable breast tissue and areolae, increased amount of dark pubic hair and of axillary hair Further increase in breast size and areolae that protrude above breast level adult pubic hair Adult stage, pubic hair with extension to upper thigh
 Progestogens") Treatment Options § Fully reversible interventions: Pubertal delay, hormone blockers (extends diagnostic period) Progestogens Androgen blockers: spironolactone, finasteride Leuprolide, Histrelin (Gn. RH agonists)
Treatment Options § Fully reversible interventions: Pubertal delay, hormone blockers (extends diagnostic period) Progestogens Androgen blockers: spironolactone, finasteride Leuprolide, Histrelin (Gn. RH agonists)
 Progesterone/Prometrium®") Progestins Medroxyprogesterone/Provera® – 10 mg/d cost 10 mg tab = $0. 18 (generic) Progesterone/Prometrium® - 100 mg/d cost 100 mg tab = $1. 00 (no generic)
Progestins Medroxyprogesterone/Provera® – 10 mg/d cost 10 mg tab = $0. 18 (generic) Progesterone/Prometrium® - 100 mg/d cost 100 mg tab = $1. 00 (no generic)
 • Effects reversible") Progestins – desired effects • Used for “chemical castration”, contraception (mini-pill) • Effects reversible • Suppresses estrogen and testosterone production • Stops periods • Not feminizing by itself, but contributes to breast growth when used with estrogen
Progestins – desired effects • Used for “chemical castration”, contraception (mini-pill) • Effects reversible • Suppresses estrogen and testosterone production • Stops periods • Not feminizing by itself, but contributes to breast growth when used with estrogen
 Progestins – adverse effects • Elevates cholesterol • Decreases bone density • Some report depression (Provera)
Progestins – adverse effects • Elevates cholesterol • Decreases bone density • Some report depression (Provera)
 Androgen Blockers Spironolactone - 50 -200 mg/d div. twice daily cost 100 mg tab = $1. 17 • Blocks testosterone receptors • Diuretic, retains potassium (avoid salt substitutes), sodium and water loss (dehydration cramps), mild decrease in blood pressure • Decreased blood count since testosterone stimulates RBC production
Androgen Blockers Spironolactone - 50 -200 mg/d div. twice daily cost 100 mg tab = $1. 17 • Blocks testosterone receptors • Diuretic, retains potassium (avoid salt substitutes), sodium and water loss (dehydration cramps), mild decrease in blood pressure • Decreased blood count since testosterone stimulates RBC production
 • Blocks 5 -alpha-reductase • Stops conversion of") Androgen Blockers - MTF Finasteride (Proscar®/Propecia®) • Blocks 5 -alpha-reductase • Stops conversion of testosterone to DHT • 5 mg tabs = $2. 50$3. 00 • 1 mg tabs = $2. 00
Androgen Blockers - MTF Finasteride (Proscar®/Propecia®) • Blocks 5 -alpha-reductase • Stops conversion of testosterone to DHT • 5 mg tabs = $2. 50$3. 00 • 1 mg tabs = $2. 00
 Estrogen Blockers § Tamoxifen – binds and blocks estrogen receptors in breast, partial agonist on endometrium. Adverse effects: endometrial cancer, hypertriglyceridemia, thromboembolism. § 20 mg tab = $0. 72
Estrogen Blockers § Tamoxifen – binds and blocks estrogen receptors in breast, partial agonist on endometrium. Adverse effects: endometrial cancer, hypertriglyceridemia, thromboembolism. § 20 mg tab = $0. 72
 Estrogen Blockers § Clomiphene - binds and blocks estrogen receptors. Adverse effects: ovarian enlargement, cyst formation. § 50 mg tab = $2. 83
Estrogen Blockers § Clomiphene - binds and blocks estrogen receptors. Adverse effects: ovarian enlargement, cyst formation. § 50 mg tab = $2. 83
 Gn. RH Agonists § Block release of FSH/LH at pituitary, therefore no stimulation of gonads to produce sex hormones
Gn. RH Agonists § Block release of FSH/LH at pituitary, therefore no stimulation of gonads to produce sex hormones
 intramuscular $300/mo. § Depo-Lupron® intramuscular $1, 500 -$2,") Gn. RH Agonists § Leuprolide (Lupron®) intramuscular $300/mo. § Depo-Lupron® intramuscular $1, 500 -$2, 000/mo.
Gn. RH Agonists § Leuprolide (Lupron®) intramuscular $300/mo. § Depo-Lupron® intramuscular $1, 500 -$2, 000/mo.
 Gn. RH Agonists § Histrelin subcutaneous hydrogel implant Vantas®, $1, 400/year for prostate Ca/uterine fibroids § Supprelin LA®, $16, 700/year for CPP
Gn. RH Agonists § Histrelin subcutaneous hydrogel implant Vantas®, $1, 400/year for prostate Ca/uterine fibroids § Supprelin LA®, $16, 700/year for CPP
 Gn. RH Agonists – adverse effects • Decreases bone density with prolonged use • Local irritation (implant)
Gn. RH Agonists – adverse effects • Decreases bone density with prolonged use • Local irritation (implant)
 Treatment Options § Partially reversible interventions: Cross-gender hormone therapy § Testosterone enanthate, cypionate (IM, transdermal) § Estradiol (oral, IM, transdermal)
Treatment Options § Partially reversible interventions: Cross-gender hormone therapy § Testosterone enanthate, cypionate (IM, transdermal) § Estradiol (oral, IM, transdermal)
 Treatment Options § Irreversible interventions: Surgery Mastectomy Hysterectomy Phalloplasty Metoidioplasty Vaginoplasty Augmentation mammoplasty
Treatment Options § Irreversible interventions: Surgery Mastectomy Hysterectomy Phalloplasty Metoidioplasty Vaginoplasty Augmentation mammoplasty
 Physician Encounter § Collaborate with patient in treatment planning § Discuss patient goals, eligibility criteria, treatment options, expectations, risks, benefits and alternatives § Obtain informed consent, and consent of parent/guardian if patient is a dependent minor (may qualify as confidential reproductive care for minors in some states? )
Physician Encounter § Collaborate with patient in treatment planning § Discuss patient goals, eligibility criteria, treatment options, expectations, risks, benefits and alternatives § Obtain informed consent, and consent of parent/guardian if patient is a dependent minor (may qualify as confidential reproductive care for minors in some states? )
 •") Carol F. Milazzo, M. D. AUTHORIZATION FOR AND CONSENT TO MEDICAL TREATMENT (WPATH) • 1. I hereby agree and consent to allow Dr. Milazzo to provide and supervise my medical treatment in accordance with the WPATH Standards of Care. • 2. I have read and understood the information provided to me on medical treatment protocols, their risks, benefits and alternatives. • 3. I agree that I meet the eligibility criteria and readiness criteria for this medical treatment. • 4. I have had a chance to ask questions. • 5. The medical treatment protocols, their risks, benefits and alternatives have been adequately explained to me. • 6. I agree to comply with medical examinations and laboratory testing which Dr. Milazzo deems necessary to supervise my treatment. Signature: Date: Signature: Relationship: _______ (parent/conservator/guardian for minor under 18 years old)
Carol F. Milazzo, M. D. AUTHORIZATION FOR AND CONSENT TO MEDICAL TREATMENT (WPATH) • 1. I hereby agree and consent to allow Dr. Milazzo to provide and supervise my medical treatment in accordance with the WPATH Standards of Care. • 2. I have read and understood the information provided to me on medical treatment protocols, their risks, benefits and alternatives. • 3. I agree that I meet the eligibility criteria and readiness criteria for this medical treatment. • 4. I have had a chance to ask questions. • 5. The medical treatment protocols, their risks, benefits and alternatives have been adequately explained to me. • 6. I agree to comply with medical examinations and laboratory testing which Dr. Milazzo deems necessary to supervise my treatment. Signature: Date: Signature: Relationship: _______ (parent/conservator/guardian for minor under 18 years old)
 Physician Encounter § Medical, family and social history and review of systems for issues that may impact treatment—smoking, endocrine, cancer, liver, coagulation problems, STD’s, prior or concurrent treatments, family support, ability to afford treatments
Physician Encounter § Medical, family and social history and review of systems for issues that may impact treatment—smoking, endocrine, cancer, liver, coagulation problems, STD’s, prior or concurrent treatments, family support, ability to afford treatments
 physical examination § Investigate physiologic issues— pre-treatment") Physician Encounter § Problem focused (or expanded) physical examination § Investigate physiologic issues— pre-treatment hormone levels, intersex conditions § Order baseline and other indicated laboratory tests
Physician Encounter § Problem focused (or expanded) physical examination § Investigate physiologic issues— pre-treatment hormone levels, intersex conditions § Order baseline and other indicated laboratory tests
 Follow up management § Reassess goals § Monitor for clinical response, adverse effects and adjust treatment § Follow up laboratory tests § Provide referrals to competent and sensitive consultants, mammograms, pelvic exams, surgeons
Follow up management § Reassess goals § Monitor for clinical response, adverse effects and adjust treatment § Follow up laboratory tests § Provide referrals to competent and sensitive consultants, mammograms, pelvic exams, surgeons
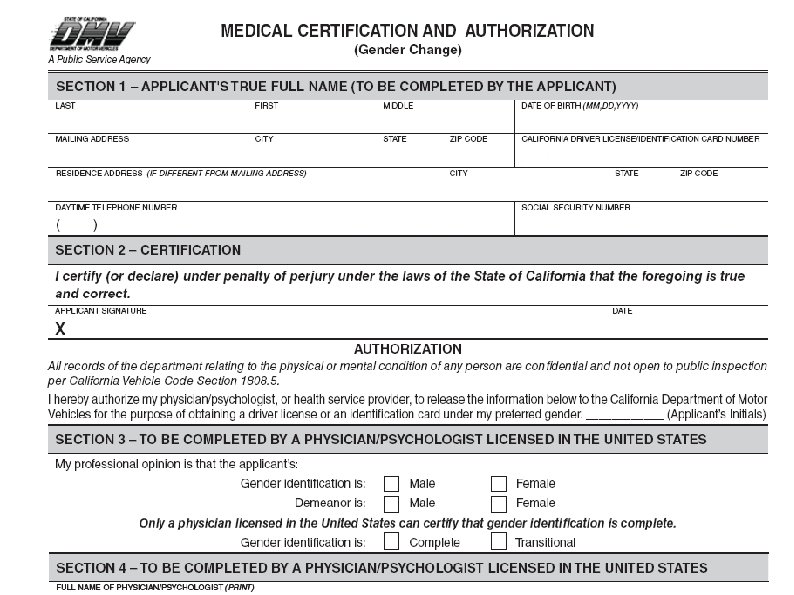
 Follow up management § Assist with ID documentation change DMV Form DL 329
Follow up management § Assist with ID documentation change DMV Form DL 329
 § Provide") Follow up management § Provide referrals to local peer support groups (mentoring) § Provide referrals to family support groups: Trans Youth Family Allies, PFLAG transgender network Gender Spectrum Family
Follow up management § Provide referrals to local peer support groups (mentoring) § Provide referrals to family support groups: Trans Youth Family Allies, PFLAG transgender network Gender Spectrum Family
 Billing issues § ICD-9 -DM Diagnostic codes § Medical diagnoses § Endocrine disorder (259. 9) § Hypogonadism (257. 2) Mental health diagnosis § § Gender identity disorder (302. 85)
Billing issues § ICD-9 -DM Diagnostic codes § Medical diagnoses § Endocrine disorder (259. 9) § Hypogonadism (257. 2) Mental health diagnosis § § Gender identity disorder (302. 85)
 AMA Resolution § “June 2007, the AMA House of Delegates voted to revise current AMA policies to ensure inclusion and protection for transgender physicians, medical students and patients. ”
AMA Resolution § “June 2007, the AMA House of Delegates voted to revise current AMA policies to ensure inclusion and protection for transgender physicians, medical students and patients. ”
 § RESOLVED, That the AMA support public and private health") AMA Resolution 122 (2008) § RESOLVED, That the AMA support public and private health insurance coverage for treatment of gender identity disorder; and be it further RESOLVED, That the AMA oppose categorical exclusions of coverage for treatment of gender identity disorder when prescribed by a physician.
AMA Resolution 122 (2008) § RESOLVED, That the AMA support public and private health insurance coverage for treatment of gender identity disorder; and be it further RESOLVED, That the AMA oppose categorical exclusions of coverage for treatment of gender identity disorder when prescribed by a physician.
 References World Professional Association for Transgender Health’s Standards of Care for Gender Identity Disorders, Sixth Version, February 2001. http: //www. wpath. org
References World Professional Association for Transgender Health’s Standards of Care for Gender Identity Disorders, Sixth Version, February 2001. http: //www. wpath. org
 References An Overview of U. S. Trans Health Priorities: A Report by the Disparities Working Group of the National Coalition for LGBT Health, August, 2004. http: //www. nctequality. org/Health. Priorities. pdf
References An Overview of U. S. Trans Health Priorities: A Report by the Disparities Working Group of the National Coalition for LGBT Health, August, 2004. http: //www. nctequality. org/Health. Priorities. pdf
 References Sausa, L. The HIV Prevention and Educational Needs of Trans Youth: A Qualitative Study, 2003. http: //www. lydiasausa. com/Resources. htm
References Sausa, L. The HIV Prevention and Educational Needs of Trans Youth: A Qualitative Study, 2003. http: //www. lydiasausa. com/Resources. htm
 References de Vries, A. , Cohen-Kettenis, P. , Delemarre -van der Waal, H. “Clinical Management of Gender Dysphoria in Adolescents. ” IJT 9. 3/4 (2006): 83 -94.
References de Vries, A. , Cohen-Kettenis, P. , Delemarre -van der Waal, H. “Clinical Management of Gender Dysphoria in Adolescents. ” IJT 9. 3/4 (2006): 83 -94.
 Resources § PFLAG Transgender Network www. pflag. org § Trans Youth Family Allies www. imatyfa. org
Resources § PFLAG Transgender Network www. pflag. org § Trans Youth Family Allies www. imatyfa. org
 Resources § Gender Spectrum Family www. genderspectrum. com § Children’s National Medical Center, Outreach Program for Children with Gender-Variant Behaviors and their Families www. dcchildrens. com
Resources § Gender Spectrum Family www. genderspectrum. com § Children’s National Medical Center, Outreach Program for Children with Gender-Variant Behaviors and their Families www. dcchildrens. com
 Resources § Gender Health Center, Sacramento www. thegenderhealthcenter. org § Sacramento provider resource list at http: //www. sacgender. org/healthresources
Resources § Gender Health Center, Sacramento www. thegenderhealthcenter. org § Sacramento provider resource list at http: //www. sacgender. org/healthresources
 Resources § World Professional Association for Transgender Health www. wpath. org
Resources § World Professional Association for Transgender Health www. wpath. org
 Contact information Carol F. Milazzo, MD, FAAP www. cfmilazzo. com drmilazzo@cfmilazzo. com THANK YOU!
Contact information Carol F. Milazzo, MD, FAAP www. cfmilazzo. com drmilazzo@cfmilazzo. com THANK YOU!