

10673061.ppt
- Количество слайдов: 68
 Introductory Neuroimaging: What you need to know at 3 am And some cool stuff. . . Kathleen Tozer, MD
Introductory Neuroimaging: What you need to know at 3 am And some cool stuff. . . Kathleen Tozer, MD
 Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
 Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
 Which study? Acute change • For acute mental status change, first study is ALWAYS noncontrast head CT • Brain MR: – Stroke protocol (noncontrast) – ICH protocol (with contrast) – Tumor protocol (with contrast)
Which study? Acute change • For acute mental status change, first study is ALWAYS noncontrast head CT • Brain MR: – Stroke protocol (noncontrast) – ICH protocol (with contrast) – Tumor protocol (with contrast)
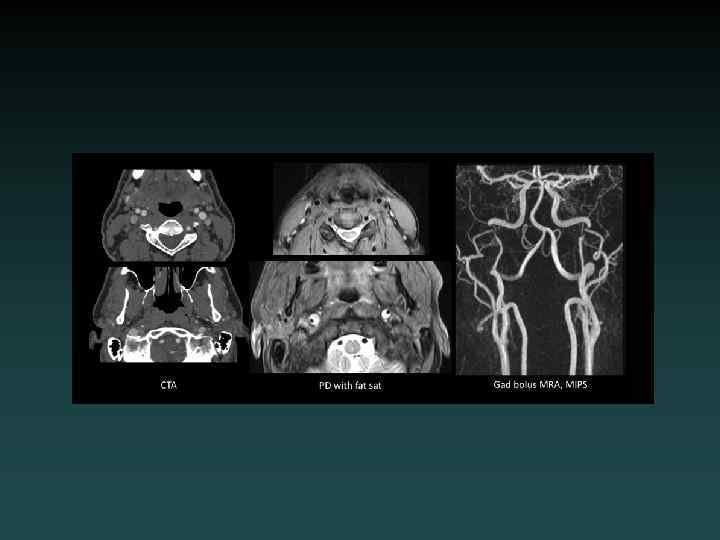
 Which study? Vascular • CTA: – Neck: Aortic arch through Circle of Willis. – Head: Circle of Willis only • MRA: – Brain: noncontrast – Neck: without and with contrast.
Which study? Vascular • CTA: – Neck: Aortic arch through Circle of Willis. – Head: Circle of Willis only • MRA: – Brain: noncontrast – Neck: without and with contrast.
 Regarding contrast: • Iodinated contrast: – GFR > 60: • in the clear – GFR < 60: • If acute, tread cautiously, especially if <30 • Hydration, mucomyst, Sodium bicarb protocol • Decrease dose, Visipaque – ESRD: • Coordinate with hemodialysis
Regarding contrast: • Iodinated contrast: – GFR > 60: • in the clear – GFR < 60: • If acute, tread cautiously, especially if <30 • Hydration, mucomyst, Sodium bicarb protocol • Decrease dose, Visipaque – ESRD: • Coordinate with hemodialysis
 Regarding contrast: • Gadolinium contrast: – GFR > 60: • in the clear – GFR 30 -60: • weigh risks. • Consider noncontrast study first. • Multihance – GFR < 30: • CONTRAINDICATED due to risk of NSF (nephrogenic systemic fibrosis). – Try noncontrast. – Consult radiology for alternative studies.
Regarding contrast: • Gadolinium contrast: – GFR > 60: • in the clear – GFR 30 -60: • weigh risks. • Consider noncontrast study first. • Multihance – GFR < 30: • CONTRAINDICATED due to risk of NSF (nephrogenic systemic fibrosis). – Try noncontrast. – Consult radiology for alternative studies.
 • CT density scale: – – – – Air = -1000") Hounsfield Units (HU) • CT density scale: – – – – Air = -1000 Fat = -120 Water = 0 Muscle = +40 Blood clot = +65 Bone = +1000 Metal >> +1000
Hounsfield Units (HU) • CT density scale: – – – – Air = -1000 Fat = -120 Water = 0 Muscle = +40 Blood clot = +65 Bone = +1000 Metal >> +1000
 Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
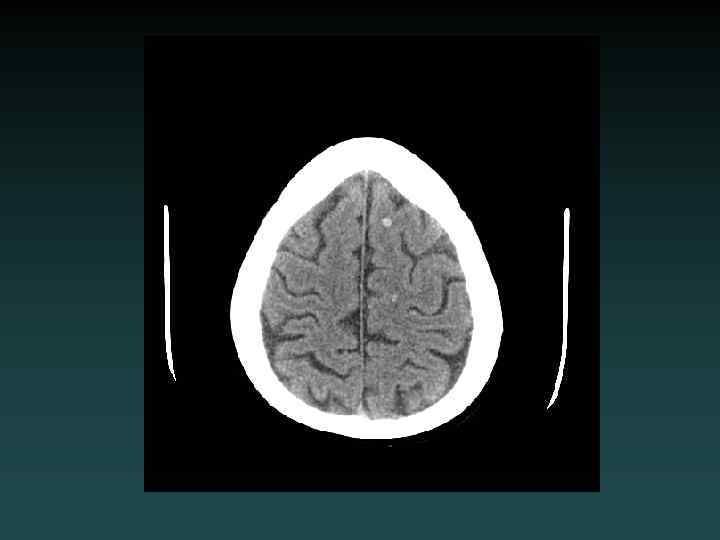
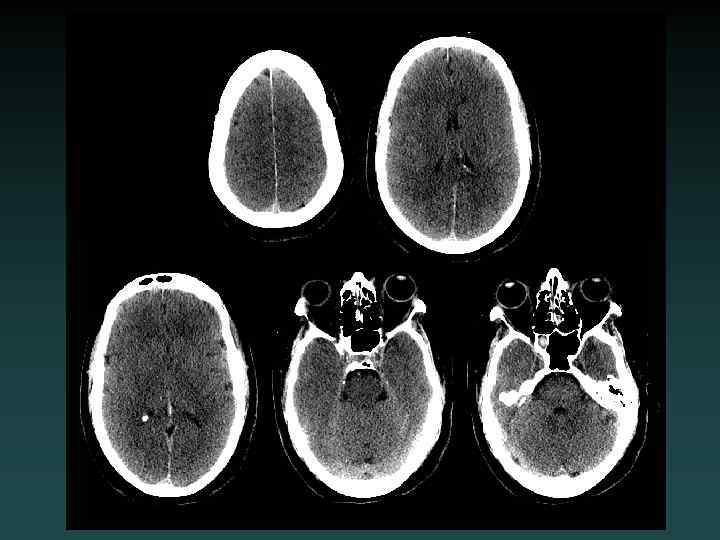
 Normal Anatomy
Normal Anatomy
 Normal Anatomy
Normal Anatomy
 Normal Anatomy
Normal Anatomy
 Normal Anatomy
Normal Anatomy
 Acute Head CT Checklist • • Midline Shift Mass Effect Density CSF Spaces Vascular Territories Intra-/Extra-axial Herniation
Acute Head CT Checklist • • Midline Shift Mass Effect Density CSF Spaces Vascular Territories Intra-/Extra-axial Herniation
 Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
 Epidural Hematoma • Injury to epidural vessel – Arterial bleeding • Lentiform shape • Does not cross sutures – May cross falx or tentorium • Look for: – FRACTURE – RAPID EXPANSION
Epidural Hematoma • Injury to epidural vessel – Arterial bleeding • Lentiform shape • Does not cross sutures – May cross falx or tentorium • Look for: – FRACTURE – RAPID EXPANSION
 Acute Subdural Hematoma • Injury to bridging vessel – Venous • Crescent shaped • May cross sutures – Does not cross falx or tentorium • Does not enter sulci • Watch for: – MASS EFFECT – SLOW EXPANSION
Acute Subdural Hematoma • Injury to bridging vessel – Venous • Crescent shaped • May cross sutures – Does not cross falx or tentorium • Does not enter sulci • Watch for: – MASS EFFECT – SLOW EXPANSION

 • MIXED – (Acute-on-chronic)") Chronic Subdural Hematoma • HYPODENSE – (blood degradation) • MIXED – (Acute-on-chronic)
Chronic Subdural Hematoma • HYPODENSE – (blood degradation) • MIXED – (Acute-on-chronic)

 Isodense Subdural Hematoma • ISODENSE – Coagulopathy – Anemia – Evolution of blood products • Look for: – Sulcal Effacement – Subtle Mass Effect
Isodense Subdural Hematoma • ISODENSE – Coagulopathy – Anemia – Evolution of blood products • Look for: – Sulcal Effacement – Subtle Mass Effect
 Subarachnoid Hemorrhage • Subarachnoid – Sulci – Cisterns – Ventricles • Trauma – lateral convexities • Aneurysm – basal cisterns • Interpeduncular Cistern – most sensitive
Subarachnoid Hemorrhage • Subarachnoid – Sulci – Cisterns – Ventricles • Trauma – lateral convexities • Aneurysm – basal cisterns • Interpeduncular Cistern – most sensitive
 Cerebral Contusion • Intraparenchymal • “Coup-Contrecoup” – Blow to head – Sudden deceleration – Brain impacts inner table (contralateral side) • Look for: – Scalp contusion – Halo of edema
Cerebral Contusion • Intraparenchymal • “Coup-Contrecoup” – Blow to head – Sudden deceleration – Brain impacts inner table (contralateral side) • Look for: – Scalp contusion – Halo of edema
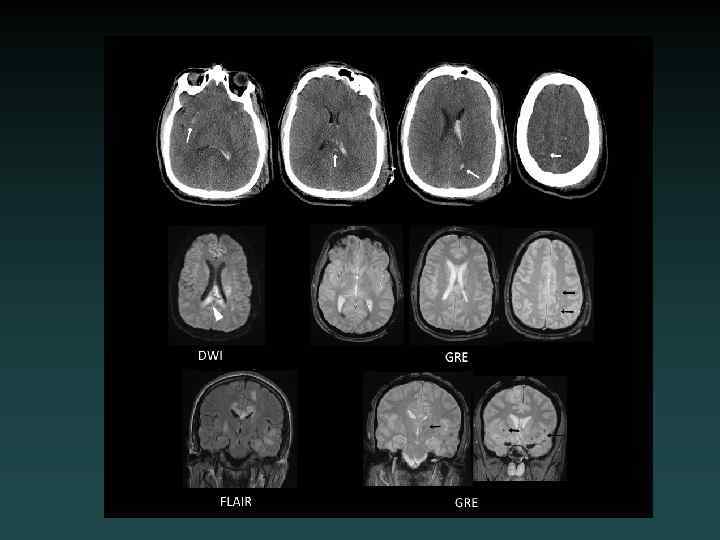
 Subcortical Injury • Shear-Strain forces – Penetrating vessels – Axonal injury • “Tip of the iceberg” – Consider MRI • Neurological deficits may be out of proportion to degree of injury visible on CT
Subcortical Injury • Shear-Strain forces – Penetrating vessels – Axonal injury • “Tip of the iceberg” – Consider MRI • Neurological deficits may be out of proportion to degree of injury visible on CT
 MRI: Diffuse Axonal Injury
MRI: Diffuse Axonal Injury
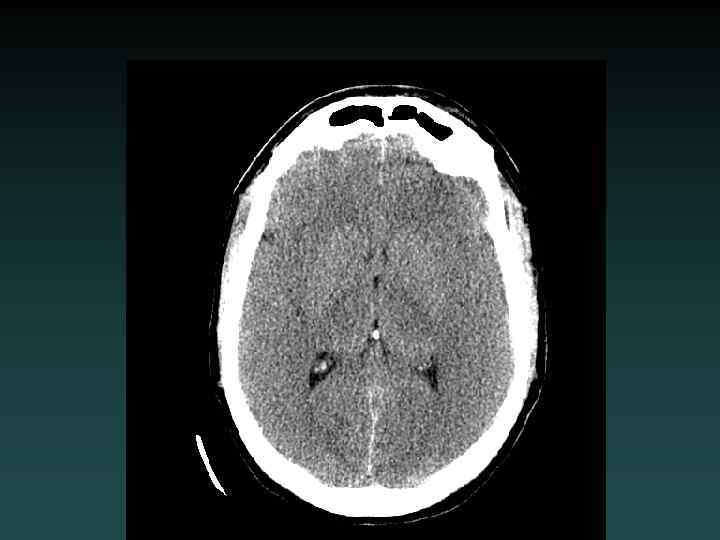
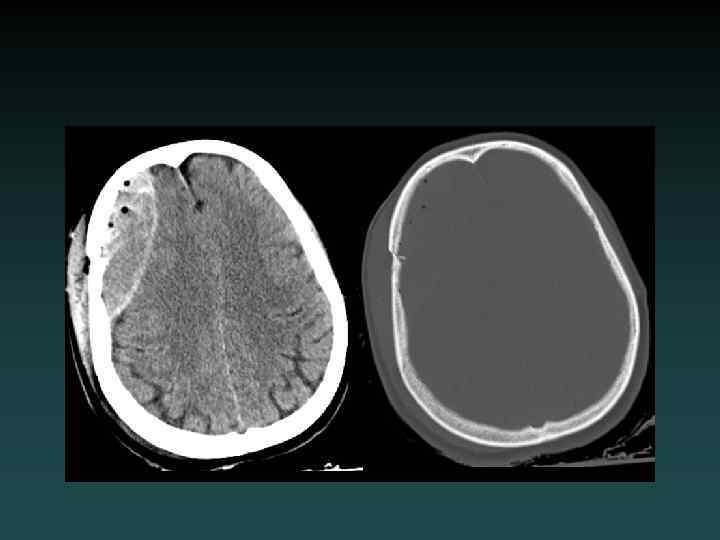
 Diffuse Cerebral Edema • Grey-white interface often obscured • Sulcal effacement • Focal subtypes: – Vasogenic • Extracellular • White matter > GM – Cytotoxic • Intracellular • Grey matter > WM
Diffuse Cerebral Edema • Grey-white interface often obscured • Sulcal effacement • Focal subtypes: – Vasogenic • Extracellular • White matter > GM – Cytotoxic • Intracellular • Grey matter > WM
 Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
 Stroke
Stroke
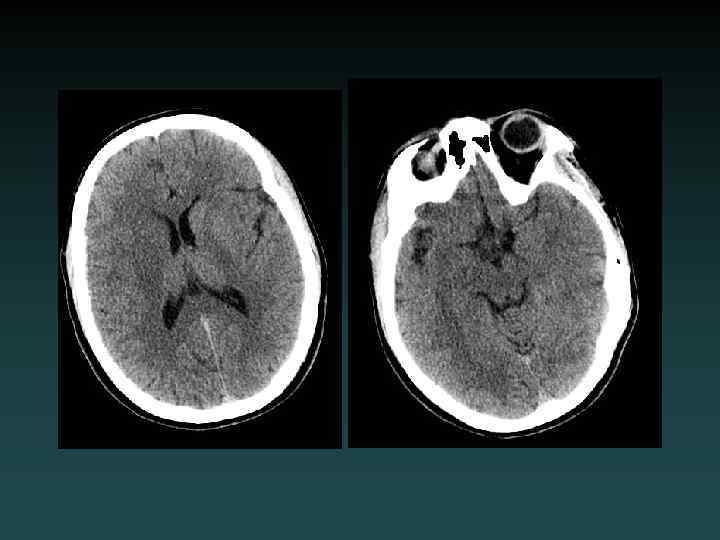
 Acute Ischemia-Infarction • Subtle HYPODENSITY – Vascular distribution – Loss of grey-white margin • CT often NEGATIVE • Early CT signs – “Hyperdense MCA” – “Insular ribbon” • Role of CT: EXCLUDE BLEED • MRA or CTA useful • DSA for intervention • Early treatment may improve outcome
Acute Ischemia-Infarction • Subtle HYPODENSITY – Vascular distribution – Loss of grey-white margin • CT often NEGATIVE • Early CT signs – “Hyperdense MCA” – “Insular ribbon” • Role of CT: EXCLUDE BLEED • MRA or CTA useful • DSA for intervention • Early treatment may improve outcome
 Diffusion-MRI: Acute Infarct
Diffusion-MRI: Acute Infarct
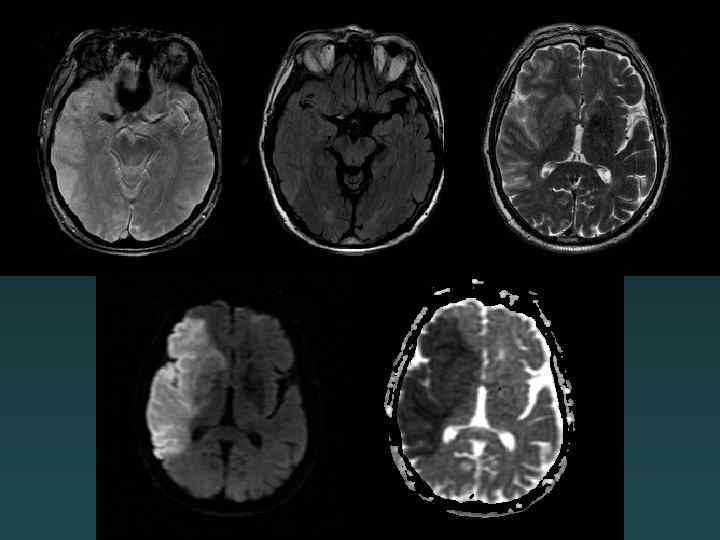
 Acute facial droop, hemiparesis
Acute facial droop, hemiparesis
 CTA
CTA
 Angio
Angio
 Post intervention
Post intervention
 Watershed Infarction
Watershed Infarction
 15 hours later
15 hours later
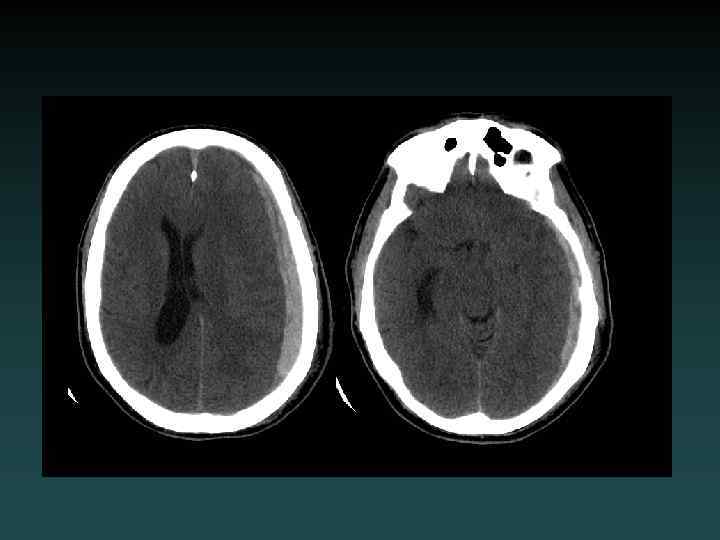
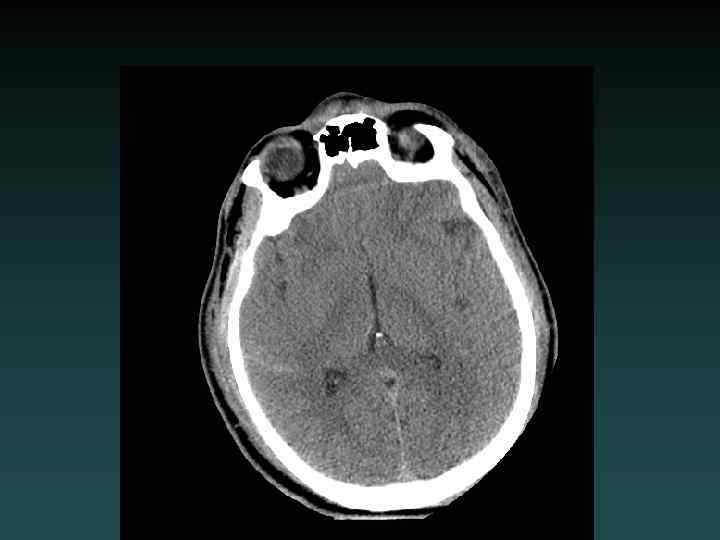
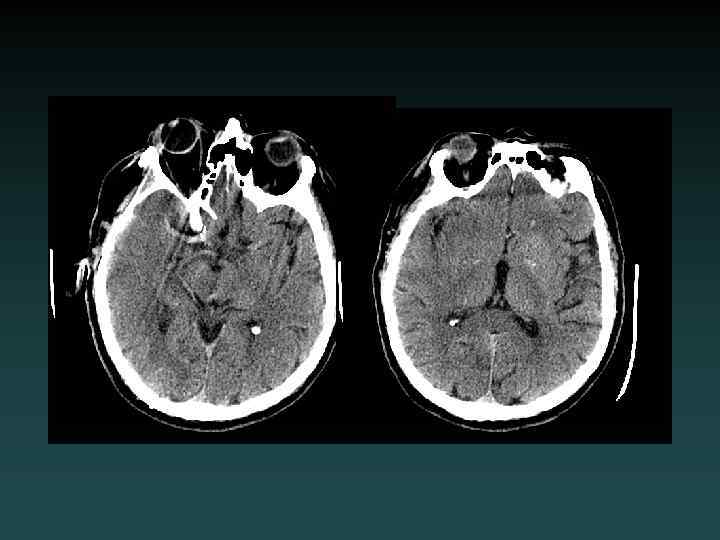
 Anoxic brain injury • Loss of Gray-White • Progresses with worsening edema • Pseudo. SAH • Hydrocephalus • Cisterns compressed
Anoxic brain injury • Loss of Gray-White • Progresses with worsening edema • Pseudo. SAH • Hydrocephalus • Cisterns compressed
 Subacute Infarction • • 2 -14 days out Hypodensity ENHANCEMENT Hemorrhagic transformation
Subacute Infarction • • 2 -14 days out Hypodensity ENHANCEMENT Hemorrhagic transformation
 MRI: Enhancing Subacute Infarct
MRI: Enhancing Subacute Infarct
 Chronic Infarction • VOLUME LOSS – Ex vacuo dilatation • Hypodensity – encephalomalacia
Chronic Infarction • VOLUME LOSS – Ex vacuo dilatation • Hypodensity – encephalomalacia
 Dural Sinus Thrombosis • Occlusive thrombosis • Subtle early signs – Bilateral infarcts – Hemorrhages • CTV or DSA – Filling defect • MRI/MRV
Dural Sinus Thrombosis • Occlusive thrombosis • Subtle early signs – Bilateral infarcts – Hemorrhages • CTV or DSA – Filling defect • MRI/MRV

 Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
Outline • Choosing a study • Normal anatomy • Trauma • Ischemic stroke • Aneurysm
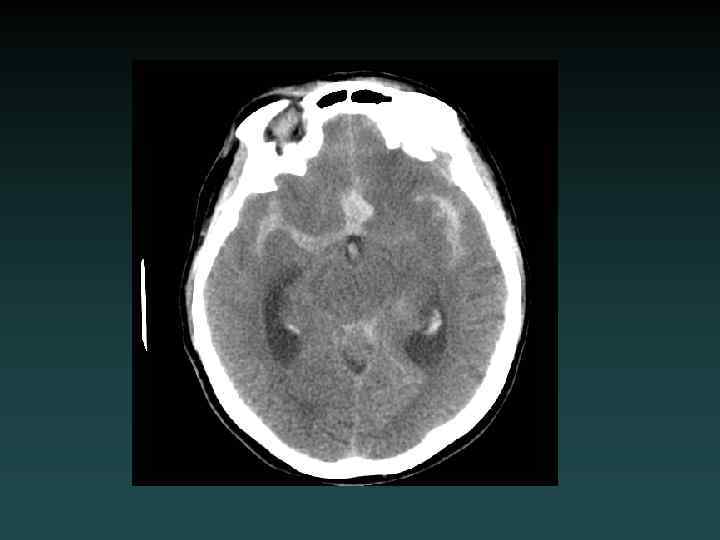
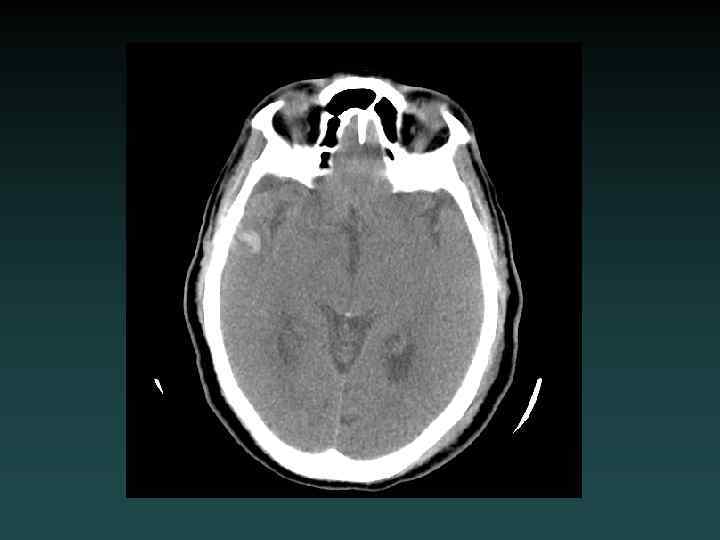
 Aneurysmal SAH • Sudden severe headache • HYPERDENSE CSF spaces • Location – Interhemispheric: ACo. A – Sylvian: MCA • HYDROCEPHALUS, VASOSPASM and ISCHEMIA – MUST find the aneurysm! • DSA, CTA and/or MRA
Aneurysmal SAH • Sudden severe headache • HYPERDENSE CSF spaces • Location – Interhemispheric: ACo. A – Sylvian: MCA • HYDROCEPHALUS, VASOSPASM and ISCHEMIA – MUST find the aneurysm! • DSA, CTA and/or MRA
 Saccular Aneurysm
Saccular Aneurysm
 Fusiform Aneurysm
Fusiform Aneurysm
 Active Re-bleeding
Active Re-bleeding
 Ruptured Aneurysm
Ruptured Aneurysm
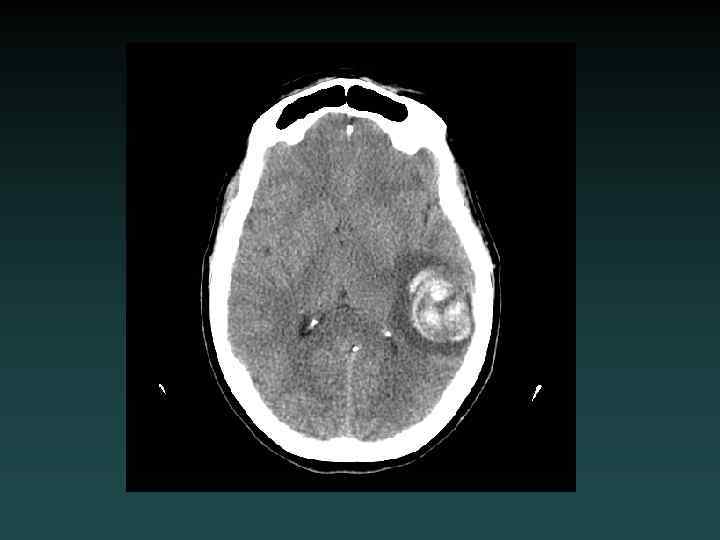
 Intracerebral Hemorrhage • Hypertension – Most common – Characteristic Locations • IF LOBAR BLEED: – – SEARCH for underlying cause! MRI/MRA/MRV DSA or CTA Repeat imaging if negative initially • Look for: – EXPANSION – UNDERLYING LESION
Intracerebral Hemorrhage • Hypertension – Most common – Characteristic Locations • IF LOBAR BLEED: – – SEARCH for underlying cause! MRI/MRA/MRV DSA or CTA Repeat imaging if negative initially • Look for: – EXPANSION – UNDERLYING LESION
 MRI: Blood Products
MRI: Blood Products
 MRI: Hemorrhagic Tumor
MRI: Hemorrhagic Tumor
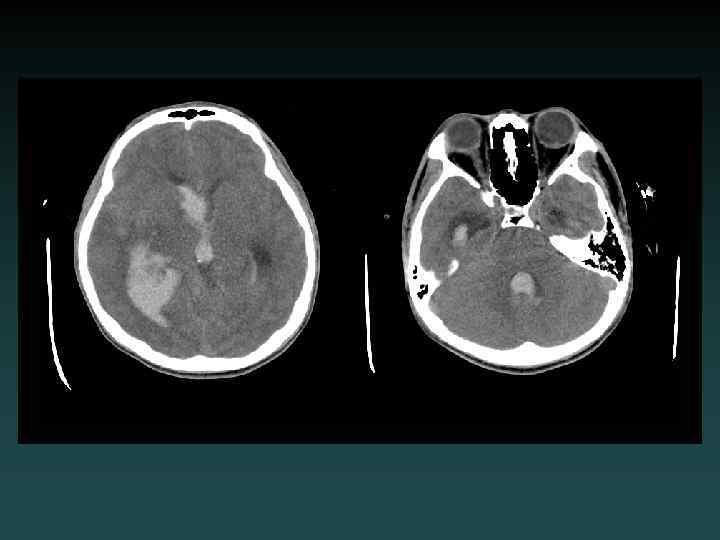
 Parenchymal Hemorrhage with Ventricular Extension
Parenchymal Hemorrhage with Ventricular Extension
 MRI Flow Voids: AVM
MRI Flow Voids: AVM