06b50509150eee38d738612dcc50c921.ppt
- Количество слайдов: 55



INTRAPARTUM PYREXIA IS NOT THE RESPONSIBILITY OF THE ANAESTHETIST - OR IS IT? Subcommittee Obstetric Anaesthesia and Intensive care Annual meeting 5 TH March 2009 P J Steer Professor of Obstetrics Academic Department of Obstetrics and Gynaecology Chelsea and Westminster Hospital © Imperial College London 1
 Steer et al,")
Study of Cord artery p. H, St Mary’s 1984 (n =1216) Steer et al, Obstet Gynecol 74: 715 -721, 1989 Epidural No Epidural

Investigation of fetal temperature during labour • Thermistor attached to the fetal surface of a Showell Surgicraft electrode • Mike Carter (bioengineer) • Luca Fusi (British Council Research Fellow) Thermistor here Mike Carter

L. Fusi, P. J. Steer, M. J. A. Maresh, and R. W. Beard. Maternal pyrexia associated with the use of epidural anaesthesia in labour. Lancet i: 1250 -1252, 1989. 82 citations to April 2008

OVERNIGHT INCREASE IN EPIDURAL RATE FROM 1% TO 83% Tripler Army Medical Center, Hawaii, October 1993 • Temperature in labour > 37. 50 C rose from 8. 2% to 26. 2% • Temperature > 380 C rose from 0. 6% to 11% M. K. Yancey, et al epidural analgesia and intrapartum maternal hyperthermia. Obstet Gynecol 98: 763 -770, 2001.

The temperature team 1992 -5 Macaulay, Steer, Bond & Randall
 Fetal core temperature 1 o. C warmer")
Main heat loss through placenta (‘heat exchanger’) Fetal core temperature 1 o. C warmer than mother (2 nd law of thermodynamics)

Probe for measuring maternal and fetal temperature in labour Fetal scalp Lower uterine segment

EPIDURAL

EPIDURAL

J. H. Macaulay, K. Bond, and P. J. Steer. Epidural analgesia in labor and fetal hyperthermia. Obstet Gynecol 80: 665 -669, 1992. Cited 36 times to April 2008

RUPTURED MEMBRANES STUDY 1997 -2000 Dick Marjanovic Charlotte Patient

RUPTURED MEMBRANES STUDY • 52 women with term prelabour rupture of the amniotic membranes • 50 chose epidural anaesthesia • Intrapartum pyrexia (>37. 5 o. C) was common: – oral 25% – uterine 77% – fetal scalp 94%

Sujoy Banerjee 2001 -3 S. Banerjee, P. Cashman, S. M. Yentis, and P. J. Steer. Maternal Temperature Monitoring During Labor: Concordance and Variability Among Monitoring Sites. Obstet. Gynecol. 103 (2): 287 -293, 2004. Intrauterine temperature probe Skin probe Powerlab

Mean temperature at different sites by duration of labour

The incidence of fever in ILEA was significantly lower at four hours (2/42, vs. 10/44, P = 0. 036)

V. R. Mantha, M. C. Vallejo, V. Ramesh, A. L. Phelps, and S. Ramanathan. Int. J Obstet Anesth. 17 (2): 123 -129, 2008.

Why do epidurals cause a rise in maternal temperature during labour?

Body temperature is a balance between heat production and heat loss • Metabolism • Muscular activity • uterine contractions • • • Conduction Convection Radiation Hyperventilation Sweating (minimum 25% of heat loss, rising to 100% if ambient temperature 370 C - Heat of vaporisation of water is about 580 Calories/litre)

Body temperature during labour • Heat production is high due to muscular activity (especially uterine contraction) • Ambient temperature is high (260 C) • Heat loss is normally high due to: – hyperventilation – Vasodilatation – Sweating

Effect of epidurals in labour • Increase vasodilatation • Decrease skeletal muscle activity • Abolish hyperventilation • Promote shivering • Abolish sweating over the lower half of the body • Modify temperature information input to hypothalamus

CONCLUSION • EPIDURALS CAUSE A RISE IN MATERNAL TEMPERATURE DURING LABOUR DOES THIS MATTER?

1657 nulliparous women with term pregnancies and singleton vertex fetuses who were afebrile at admission E. Lieberman, J. M. Lang, F. Jr Frigoletto, D. K. Richardson, S. A. Ringer, and A. Cohen. Epidural analgesia, intrapartum fever, and neonatal sepsis evaluation. Pediatrics 99 (3): 415 -419, 1997.

INTRAPARTUM MATERNAL FEVER AND NEONATAL OUTCOME • 1218 nulliparous women in spontaneous labour • labours with signs of infection were excluded • 123 women had fever > 380 C; 120 had epidurals Fever • • % 1 min Apgar score <1 % Hypotonia % Oxygen therapy % Neonatal seizures 23 5 8. 2 3. 3 Lieberman et al, Pediatrics, 105; 8 -13, 2000 No fever 8 0. 5 1. 3 0. 2
, a persistent")
INTRAPARTUM MATERNAL FEVER AND NEONATAL ENCEPHALOPATHY “Maternal pyrexia (odds ratio 3. 82), a persistent occipitoposterior position (4. 29), and an acute intrapartum event (4. 44) were all risk factors for newborn encephalopathy” N. Badawi, J. J. Kurinczuk, J. M. Keogh, L. M. Alessandri, F. O'Sullivan, Burton, PR, P. J. Pemberton, and F. J. Stanley. Intrapartum risk factors for newborn encephalopathy: the Western Australian case-control study. BMJ 317 (7172): 1554 -1558, 1998.

INTRAPARTUM MATERNAL FEVER AND CEREBRAL PALSY “Maternal fever exceeding 38 OC in labor was associated with an increased risk of unexplained cerebral palsy (odds ratio 9. 3, 95% CI 2. 7 -31. 0)” J. K. Grether and K. B. Nelson. Maternal infection and cerebral palsy in infants of normal birth weight. JAMA 278 (3): 207 -211, 1997.

NW Thames database – spontaneous onset of labour gestation 37 -42 weeks; 358, 979 births 1988 -2000

NW Thames database – spontaneous onset of labour gestation 37 -42 weeks; 358, 979 births 1988 -2000

NW Thames database – spontaneous onset of labour gestation 37 -42 weeks; 358, 979 births 1988 -2000

NW Thames database – spontaneous onset of labour gestation 37 -42 weeks; 358, 979 births 1988 -2000

NW Thames database – spontaneous onset of labour gestation 37 -42 weeks; 358, 979 births 1988 -2000

NW Thames database – spontaneous onset of labour gestation 37 -42 weeks; 358, 979 births 1988 -2000

NW Thames database – spontaneous onset of labour gestation 37 -42 weeks; 358, 979 births 1988 -2000

Perinatal outcome – multiple regression Intrapartum or neonatal death Neonatal convulsions Overall R = 0. 009 p = 0. 00003 R = 0. 007 p = 0. 02 Epidural p = 0. 3 p = 0. 9 Duration of labour p = 0. 04 p = 0. 1 Pyrexia in labour p = 0. 000025 p = 0. 018

Where both factors coexisted, the risk was 12. 5%. . . .

EVIDENCE FOR NEONATAL COOLING BEING PROTECTIVE AGAINST THE EFFECTS OF HYPOXIA • Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial – P. D. Gluckman, J. S. Wyatt, D. Azzopardi, R. Ballard, A. D. Edwards, D. M. Ferriero, R. A. Polin, C. M. Robertson, M. . Thoresen, A. Whitelaw, and A. J. Gunn. – Lancet 365: 663 -670, 2005. • Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy – S. Shankaran, A. R. Laptook, R. A. Ehrenkranz, J. E. Tyson, S. A. Mc. Donald, E. F. Donovan, A. A. Fanaroff, W. K. Poole, L. L. Wright, R. D. Higgins, N. N. Finer, W. A. Carlo, S. Duara, W. Oh, C. M. Cotten, D. K. Stevenson, B. J. Stoll, J. A. Lemons, R. Guillet, and A. H. Jobe. . – N. Engl. J Med. 353 (15): 1574 -1584, 2005.

CONCLUSIONS • The commonest cause of intrapartum pyrexia in modern practice is the use of epidural anaesthesia • Pyrexia in labour has a strong association with neonatal encephalopathy and cerebral palsy • Preventing temperature rise is known to limit hypoxic ischaemic damage in animals and stroke victims • Neonatal brain cooling can reduce damage in hypoxic ischaemic encephalopathy • Trials of temperature control in labour in relation to both short term and long term outcome are needed Banerjee S & Steer PJ International Journal of Obstetric Anaesthesia (2003) 12; 280 -286

Effect of paracetamol S. Banerjee, P. Cashman, S. M. Yentis, and P. J. Steer. Maternal Temperature Monitoring During Labor: Concordance and Variability Among Monitoring Sites. Obstet. Gynecol. 103 (2): 287 -293, 2004

Prophylactic acetaminophen does not prevent epidural fever in nulliparous women: a doubleblind placebo-controlled trial. • 42 women assigned at random to 650 mg paracetamol PR immediately after epidural anaesthesia and then 4 hrly until delivery • Maternal pyrexia >38 o. C occurred in 25% of each group • There was no evidence of infection in either group L. Goetzl, J. Rivers, T. Evans, D. R. Citron, B. E. Richardson, E. Lieberman, and M. S. Suresh. J. Perinatol. 24 (8): 471 -475, 2004.
 or")
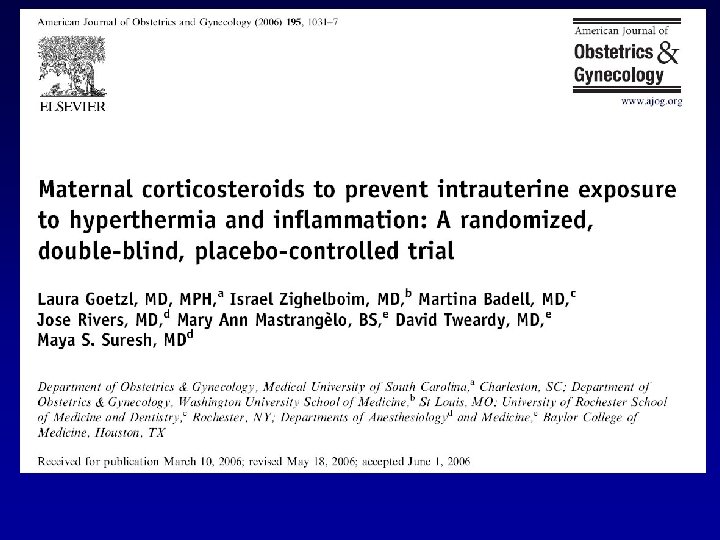
Goetzl et al 2006 • Placebo, methylprednisolone 25 mg 8 hourly (low dose) or 100 mg 4 hourly (high dose) • Randomised 101 to placebo, 50 to low dose and 49 to high dose

Goetzl et al 2006 placebo Low dose High dose Maternal fever >=380 C 34% 21. 8% 2% Neonatal sepsis evaluation 24% 17. 8% 4. 1%

“A Cobber is a cooling neck wrap which can be worn around the neck or forehead. It actually reduces your body temperature by 3 -4 degrees. ” http: //www. coolgardenstuff. com/products 2/prods/COBBER. html

Vaibhav Sharma Neck Cooler study March 2004

Cooling with the Cobber following a hot bath Initial Temperature 380 C

Case 1 Neck Cooler

FHR 175 bpm Meconium ++ Maternal Shivering +++ FBS p. H 7. 39 Neck coolers Case 4 Top-up Felt Cold

Resuscitation of the baby in case 4

N A Richards, Z S Maharoullee, S M Yentis, P J Steer Pilot study of neck warmers 2008

Nicci Richards Neck warmer study 2008 – 10 in each group

Randomised trial of neck warmers in 200 parturients starting next week

Watch this space!
06b50509150eee38d738612dcc50c921.ppt