f9de59b72888cbfeca730643543dcae0.ppt
- Количество слайдов: 95



Intraductal and intralobular epithelial proliferations Sarah E Pinder
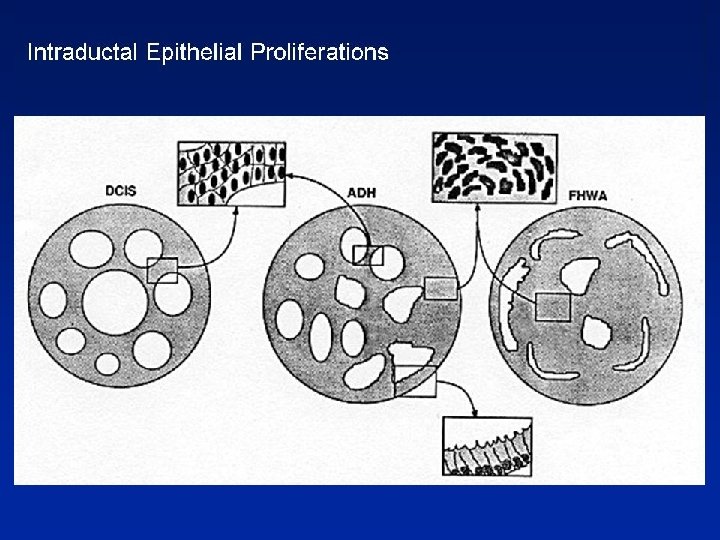

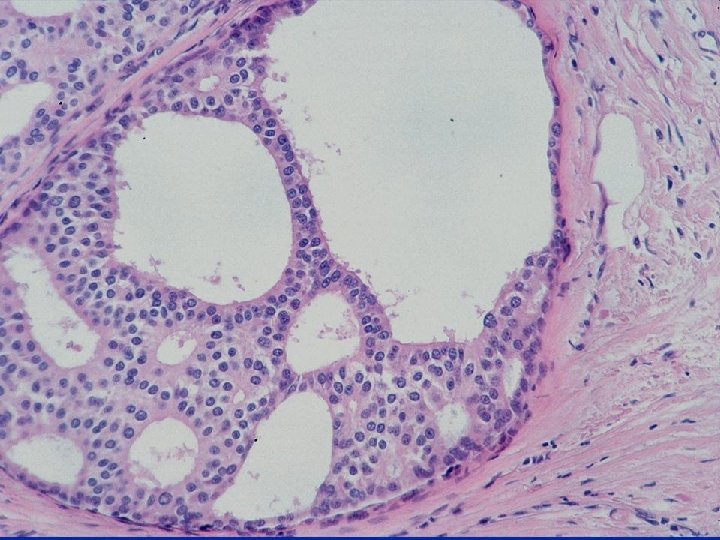
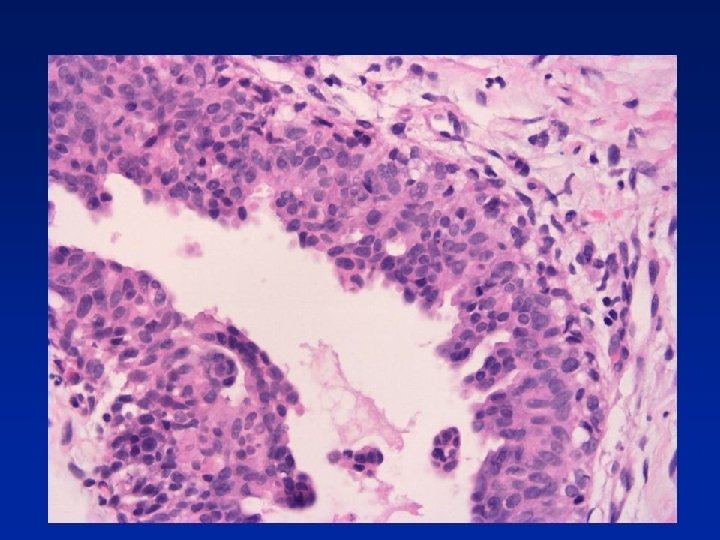
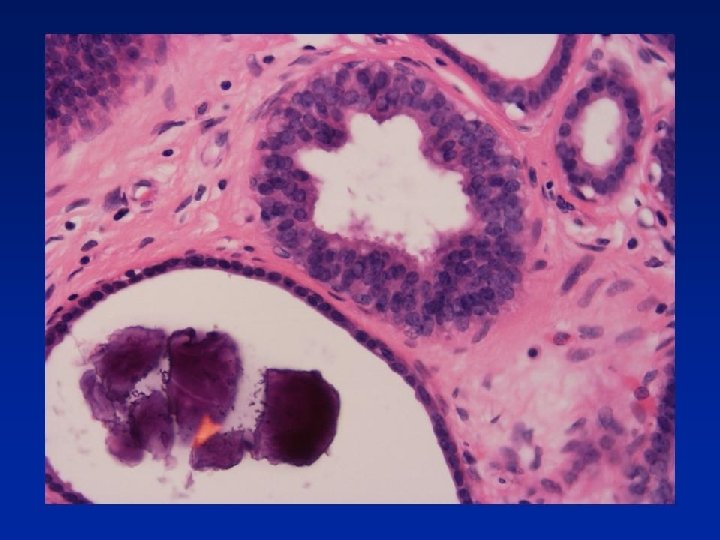
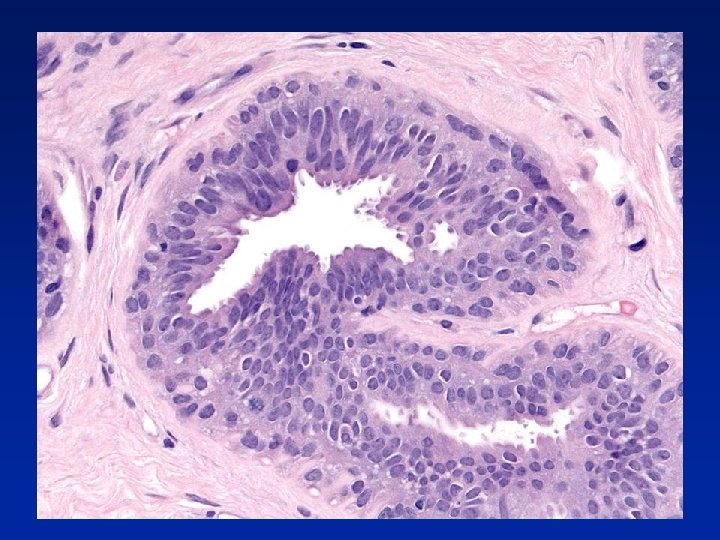
Usual Epithelial Hyperplasia • • Architectural features – Irregular fenestrations – Peripheral fenestrations – Stretched or twisted epithelial bridges – Uneven distribution and overlapping of nuclei Cellular features – Multiple cell types – Variation in appearance of epithelial cells – Variation in appearance of nuclei – Often oval rather than round – Indistinct cell margins
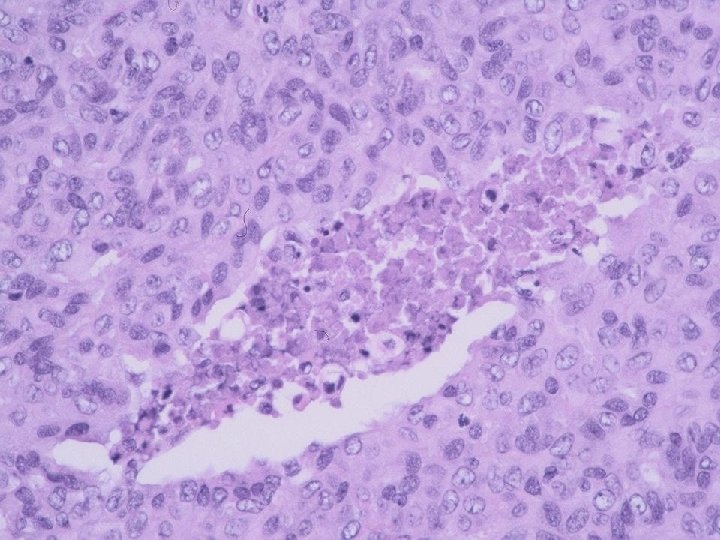

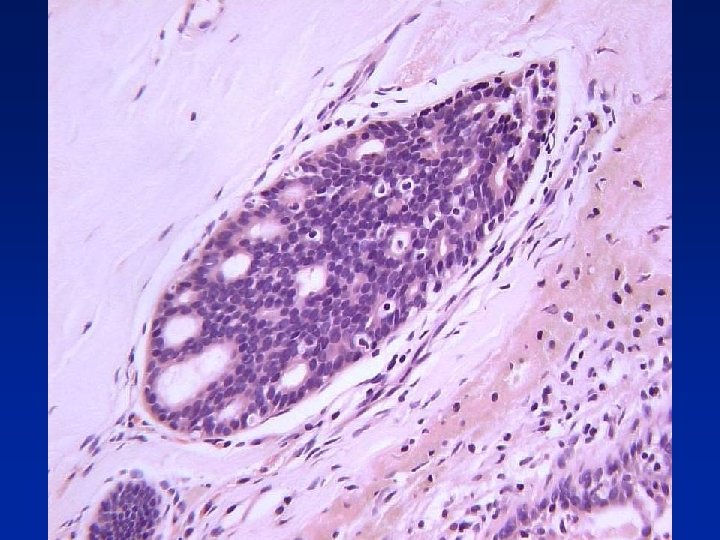
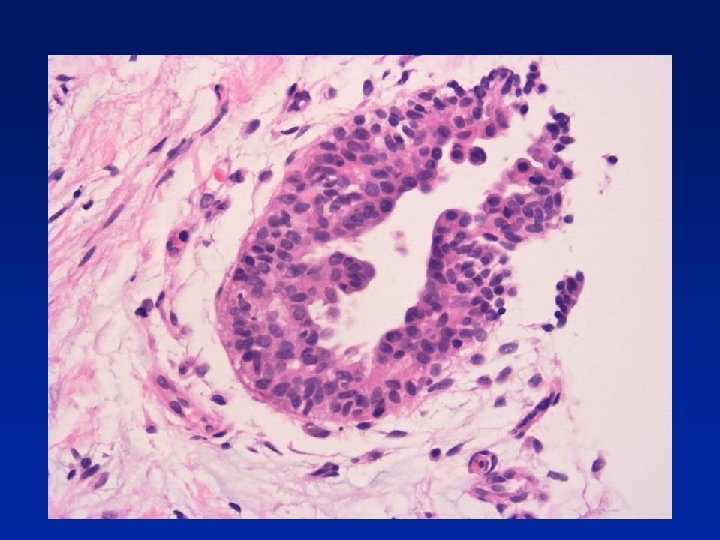
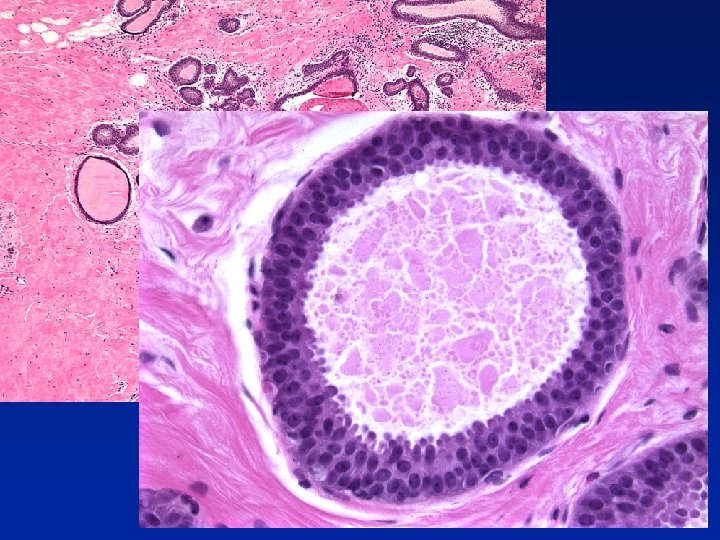
Atypical Ductal Hyperplasia Architectural features • Some features of UEH & some features of low grade DCIS Cytological features • Cells similar to those seen in low grade DCIS present in a portion of the space • Second population of cells typical of florid hyperplasia also present Size/extent • Less than 2 duct spaces with complete involvement (2 mm)
 Benign Atypical In situ")
NHS BSP EQA Scheme Kappa’s for overall diagnosis (all participants) Benign Atypical In situ / Invasive Overall hyperplasia Micro-invasive 902, 911, 912 0. 72 0. 19 0. 71 0. 81 0. 68 921, 922, 931 0. 75 0. 16 0. 71 0. 86 0. 72 932, 941, 942 0. 81 0. 15 0. 75 0. 88 0. 77 951, 952, 961 0. 75 0. 17 0. 77 0. 86 0. 77 962, 971, 972 0. 79 0. 26 0. 81 0. 91 0. 82 981, 982, 991 0. 84 0. 13 0. 69 0. 90 0. 79 All 0. 79 0. 18 0. 75 0. 88 0. 77

Common adult stem cells in the breast - biological concept Ck 5/Ck 8/18/19+ Ck 5/SMA+ Ck 8/18/19+ SMA+ “cells differentiate toward glandular or myoepithelial cells, passing through either Ck 5/Ck 8/18/19 or Ck 5/SMA-positive intermediates” Bocker et al. Lab Invest 2002; 82; 737 -745
 & basal intermediate epithelial")
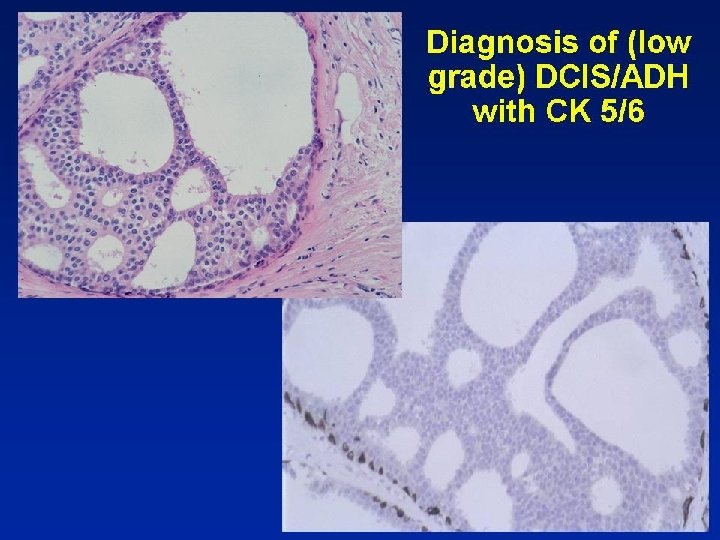
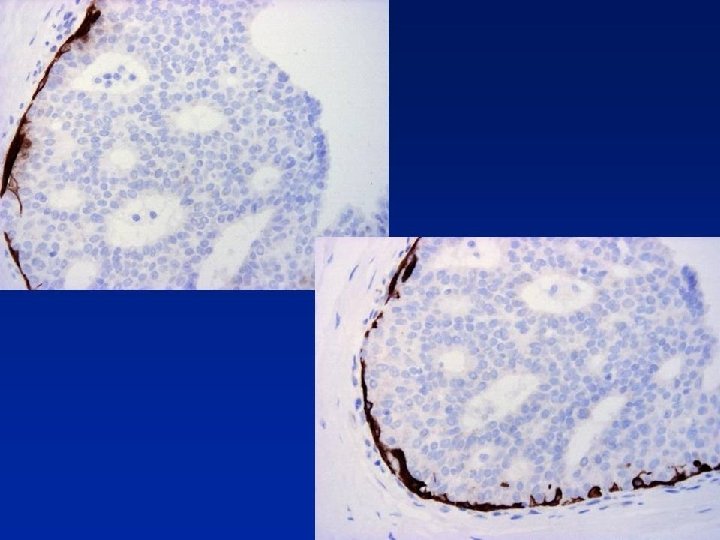
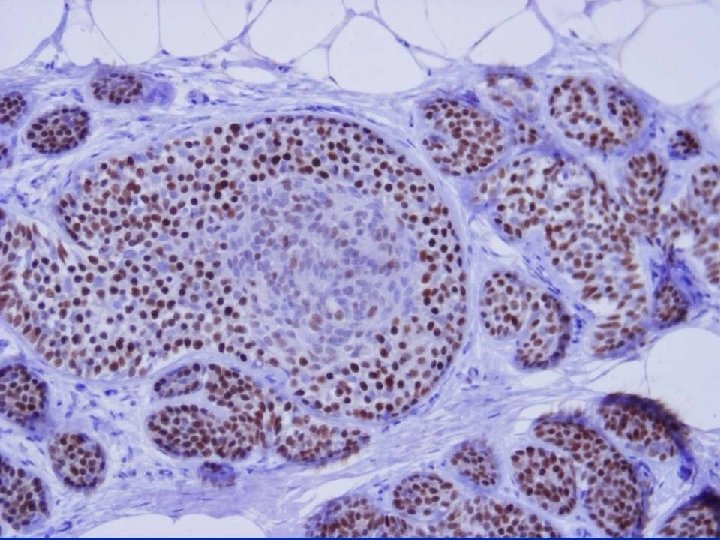
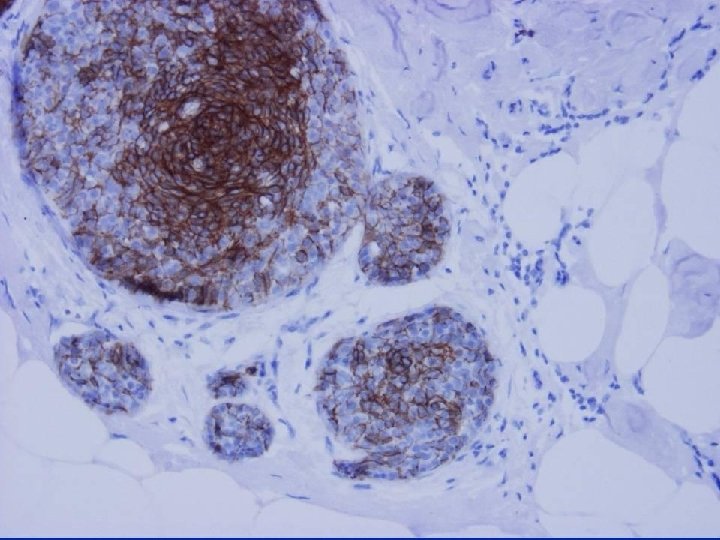
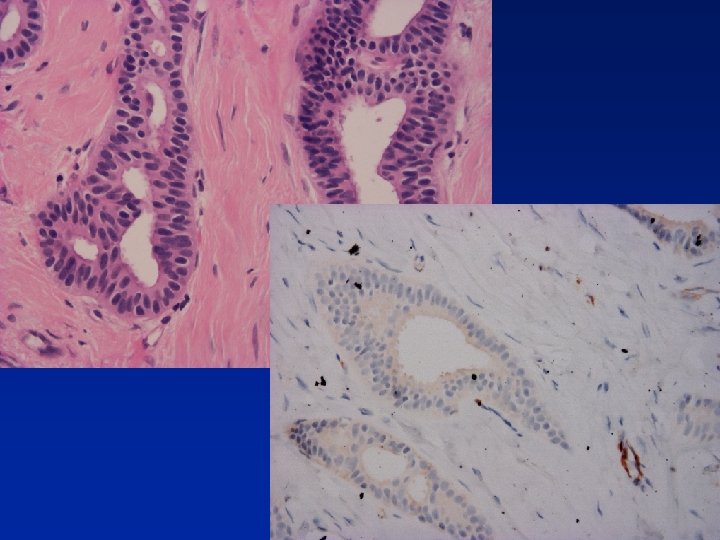
Cytokeratins in Intraductal Hyperplasia Luminal epithelial cytokeratins (CK 8, 19) & basal intermediate epithelial cytokeratins (CK 5, 6, 14) may be helpful in difficult intraductal proliferations - identify a mixed cell population in UEH Bocker W. Pathologe 1997; 18: 3 -18


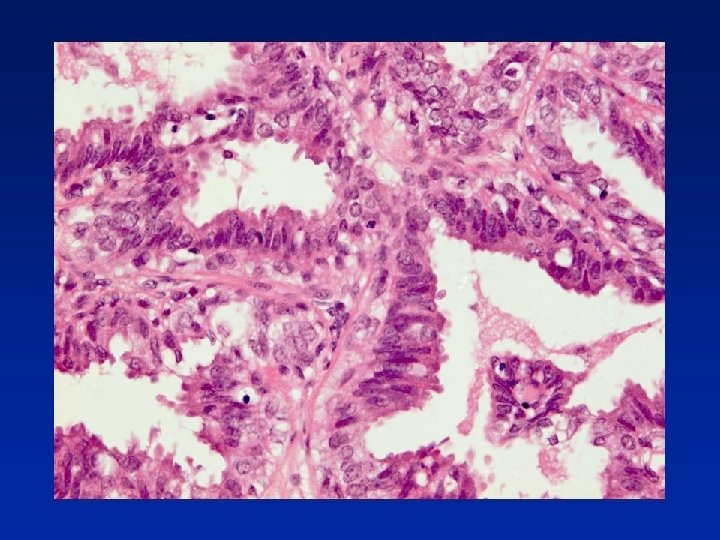
Gynaecomastoid Hyperplasia • Small, papillary-like clusters of epithelial cells • No fibrovascular stalks • 2 - 3 cells above basement membrane • Papillary clusters taper towards lumen • Small, pyknotic nuclei arranged around outer • edge of papillary structures Variable nuclear features - not regular, evenly spaced, c. f. DCIS Tham KT et al. Prog in Surg Pathol. 1989; 101 -9

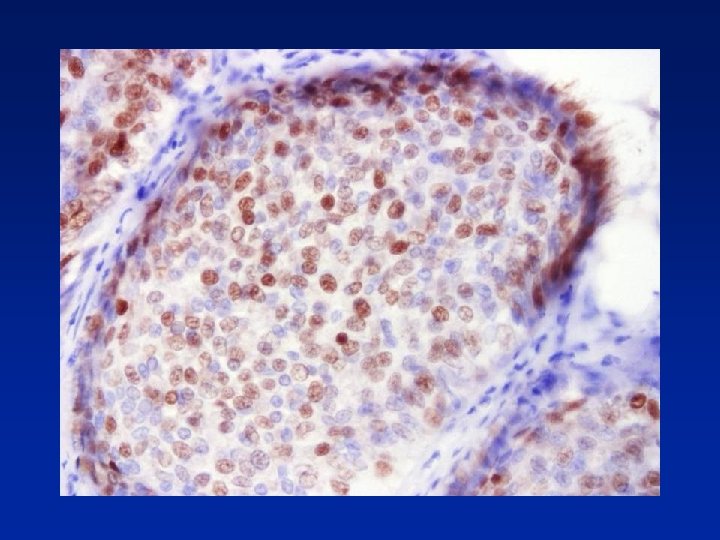
ER in Diagnosis of Intraductal Epithelial Proliferations • % of ER +ve cells slightly increased in UEH • ER +ve surrounded by ER -ve cells or • contiguous groups of +ve cells (sometimes >90% cells) In ADH, LCIS & low grade DCIS contiguous +ve cells Shoker BS et al. J Pathol 1999; 188; 237 -244


Side of Biopsy vs Side of Breast Cancer % Ipsilateral % Contralateral Low Grade DCIS ~100 ~0 ADH (NHS, Dupont & Page) ~50% AIDH (Tavassoli & Norris) ~75% ~25%

ADH - hints 1. If you have not considered low grade DCIS as diagnosis, then is NOT ADH 2. ADH is small, microfocal lesion - if lesion more than a few mm, then not ADH 3. ADH is clonal, luminal (CK 5 negative, CK 15 negative), uniformly ER positive

DCIS - Frequency 5% symptomatic breast carcinoma Over 20% screen-detected breast cancer General Population? Autopsy studies 0 -15% Welch Ann Int Med 1997

Excision of DCIS 3 D Mapping Egans Technique 82 cases 1 quadrant >1 quadrant Central 66% 23% 11% 81 cases 1 duct system 1 case Multiple ducts systems = a unicentric process Holland. Lancet 1990; 335; 519

Recurrent DCIS Genetic Studies • 18 pure DCIS with ipsilateral DCIS recurrence • 17 cases high concordance with CGH (median • • 81%) In only 1 case, no agreement Mean no. CGH changes higher in recurrence Commonest were gain of 17 q, loss of 8 p, 17 p i. e. recurrent DCIS = residual DCIS Waldman et al. JNCI 2000; 92; 313

Diagnosis of DCIS - NHS BSP EQA Scheme Kappa - Overall Diagnosis Circulation Benign In situ / MI Inv. Overall 902, 911, 912 0. 71 0. 81 0. 68 921, 922, 931 0. 75 0. 71 0. 86 0. 72 932, 941, 942 0. 81 0. 75 0. 88 0. 77 951, 952, 961 0. 75 0. 77 0. 86 0. 77 962, 971, 972 0. 79 0. 81 0. 91 0. 82 981, 982, 991 0. 84 0. 69 0. 90 0. 79 All 0. 79 0. 75 0. 88 0. 77 0. 00 – 0. 20 0. 21 – 0. 40 0. 41 – 0. 60 0. 61 – 0. 80 0. 81 – 1. 00 Slight Fair Moderate Substantial Almost perfect

Classification of DCIS Extent of DCIS - Relation to Architecture Comedo Solid Single quadrant 24 19 20 4 67 Multiple quadrant 2 (8%) 4 (17%) 5 (20%) 10 (71%) 21 26 23 25 14 88 Total Cribriform Micropapillary Total Bellamy. Hum Pathol 1993; 24; 16
 •")
DCIS - “Nottingham” Classification • Comedo DCIS • DCIS with necrosis (non-pure comedo) • DCIS without necrosis Poller et al. Modern Pathol 1994; 7: 257 -262 DCIS - Van Nuys Classification Silverstein et al. Lancet 1995; 345; 1154 -57

DCIS Differentiation • Well differentiated • Poorly differentiated • Moderately differentiated Holland et al. Sem Diag Pathol 1994; 11; 167 -180 DCIS - NHS BSP Grade • High grade • Intermediate grade • Low grade (Nuclear size, pleomorphism, nucleoli, mitoses) (Growth pattern, necrosis & polarisation) Pathology Reporting of Breast Disease. NHS BSP Publication 58, 2005

Grade & Number of Calcifications Invasion in Screen Detected Microcalcification • Grade of DCIS in core biopsy & increasing numbers of calcifications in lesion are predictive of invasion High grade & > 40 calcifications High grade & < 40 Not high grade 48% 15% 0% Bagnall MJC, Evans AJ, Wilson ARM et al. Clin Rad 2001

UK DCIS I Trial Univariate analysis for ipsilateral recurrence Grading System n N of events H. R. 95 % C. I. Nuclear Grade 1 2 3 86 225 913 6 (7. 0%) 13 (5. 8%) 135 (14. 8%) 0. 51 0. 41 1. 00* 0. 22 - 1. 15 0. 23 – 0. 72 Van Nuys Grade 1 2 3 99 212 913 5 14 135 0. 39 0. 45 1. 00* 0. 16 - 0. 94 0. 26 - 0. 78 Differentiation 1 2 3 90 248 886 6 14 134 0. 38 0. 47 1. 00* 0. 22 - 0. 66 0. 21 - 1. 07 Unpublished data

Evidence for Progression of DCIS Type Treatment Outcome High grade Biopsy alone Progression 50% in 5 yrs Low grade Biopsy alone Progression 30% in 15 yrs Low grade DCIS 40% of 28 patients with ‘missed’ lesions on biopsy developed invasion at same site at 30 year follow-up Page et al, Cancer 1995; 76; 1196 -1200

Progression of DCIS to Invasive Carcinoma Supported by Morphology • In tumours with both DCIS and invasion there is a significant correlation between grade of the DCIS and of invasive carcinoma Lampejo et al, Sem Diag Pathol 1994; 11: 215 -222 Gupta et al, Cancer 1997; 80 : 1740 -1745 • No progression in grade between the in-situ, invasive, locally recurrent and metastatic phases Millis et al, Eur J Cancer 1998; 34: 548 -553

Progression of DCIS to Invasive Carcinoma Supported by Genetic studies • • LOH common in DCIS (70 - 79%) 80% of DCIS shares LOH with associated invasive cancer O’Connell et al. JNCI; 1998; 90; 697 • CGH studies show a high degree of genetic homology between DCIS and invasive carcinoma Buerger et al, J Pathol 1999; 189: 521 -526; Bocker et al, J Pathol 2001; 195: 415 -421

DCIS Genetic studies • Allelic imbalance analysis suggests that low grade & high grade carcinomas follow different genetic pathways Roylance et al. J Pathol. 2002; 196: 32 -36

Normal cell Hyperplasia “In situ neoplasia” -16 q -16 p -17 p -22 q +6 q -17 p +11 q 13 +1 q Lobular in situ neoplasia Low Grade DCIS +17 q 12 Intermediate Grade DCIS High Grade DCIS
 Distribution of grades, & biomarkers by IHC,")
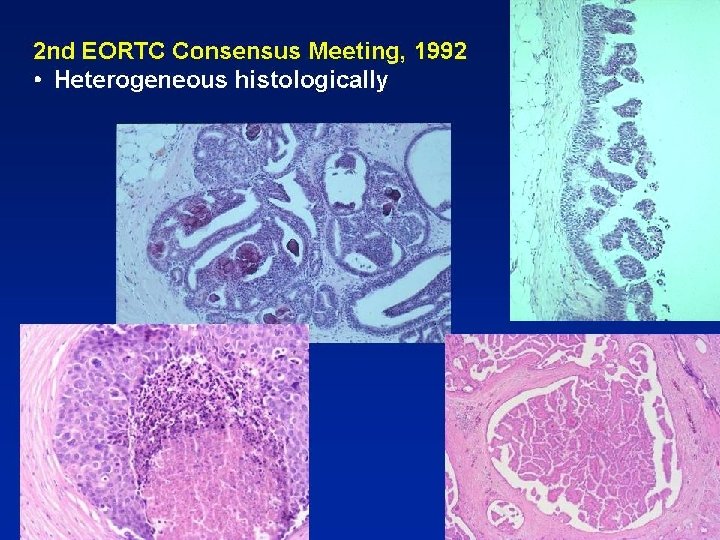
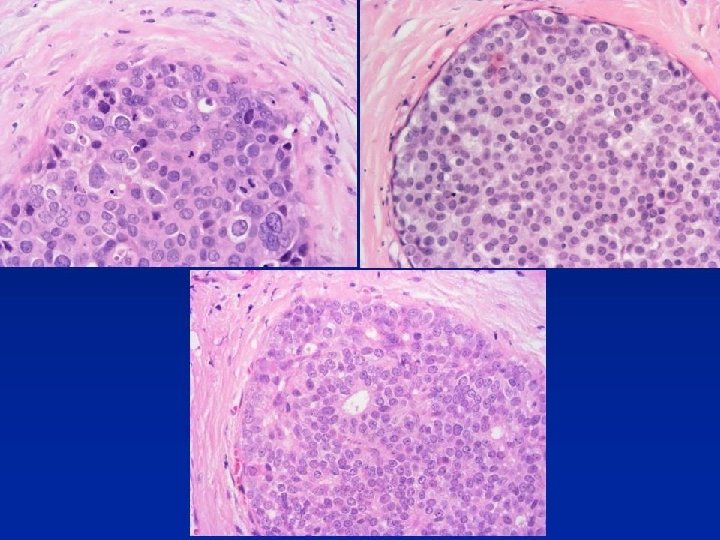
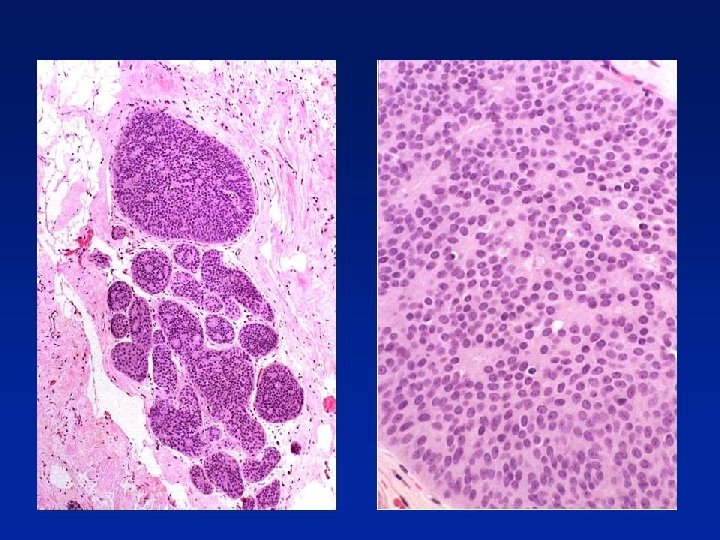
Heterogeneity? • • DCIS (n = 120) Distribution of grades, & biomarkers by IHC, ranging from well to poorly differentiated [“nearly identical to IBCs”] Multiple grades, biomarker phenotypes often coexist Supports hypothesis that poorly differentiated DCIS evolves from well-differentiated DCIS by randomly acquiring genetic defects Allred DC et al. Clin Cancer Res. 2008; 14: 370 -8

Classification of DCIS by Nuclear Grade NHS BSP EQA Scheme Circulation High Intermediate No. of cases 11 13 952, 961 0. 47 0. 19 0. 41 0. 35 962, 971, 972 0. 34 0. 25 0. 09 0. 28 981, 982, 991 0. 09 0. 06 0. 19 0. 11 992, 001, 002 0. 64 0. 29 0. 30 0. 44 0. 51 0. 23 0. 31 0. 36 Low Overall 4 28

College of American Pathologists’ Guidelines for DCIS Grading Nuclear Grade 1 Monotonous nuclei, 1. 5 to 2. 0 RBC diameters, with finely dispersed chromatin & only occasional nucleoli Grade 2 Neither nuclear grade 1 nor nuclear grade 3 Grade 3 Markedly pleomorphic nuclei, usually greater than 2. 5 RBC diameters, with coarse chromatin & prominent or multiple nucleoli

Molecular markers in DCIS • • Gene expression patterns in DCIS & invasive & metastatic tumours Serial analysis of gene expression (SAGE) m. RNA ISH to examine gene expression & IHC on TMAs Most dramatic change at normal to DCIS transition No clear universal "in situ" or "invasive" tumour signature 16, 430 transcripts analyzed Identified only 5 preferentially up-regulated in DCIS Porter D et al. Mol Cancer Res. 2003; 1: 362 -75

• • • Basal-epithelial-like group ERBB 2 -overexpressing group Normal breast-like group Luminal epithelial/ER positive group - subdivided into at least 2 sub-groups Robust - both by clustering using set selected for intrinsic properties and by outcome

Equivalent Subclasses of DCIS? • • Population-based series of 245 cases DCIS Histological characteristics & ER, HER 2, EGFR, CK 5/6, p 53 & Ki-67 Luminal A (ER+, HER 2 -); n = 149 (61%) Luminal B (ER+, HER 2+); n = 23 (9%) HER 2 positive (ER-, HER 2+); n = 38 (16%) Basal-like (ER-, HER 2 -, EGFR+ and/or CK 5/6+); n = 19 [8%] 16 (6%) unclassified (-ve for all 4 markers) Livasy CA et al. Hum Pathol. 2007; 38: 197 -204

Classification of DCIS by gene expression profiling • • • Supervised cluster analysis of 14 poorly differentiated DCIS & 24 grade 3 invasive carcinomas 80 genes differentially expressed, 13 up-regulated in DCIS & 67 down-regulated Mostly involved in cell growth & metabolism, protein binding Hannemann et al. Breast Cancer Res 2006; 8; R 61

Normal cell Hyperplasia “In situ neoplasia” -16 q -16 p -17 p -16 q -17 p LCIS & subgroup of DCIS may be different phenotypic forms of a common genotype +11 q 13 +1 q Lobular in situ neoplasia Low Grade DCIS +17 q 12 Intermediate Grade DCIS High Grade DCIS

Distinguishing LCIS from DCIS

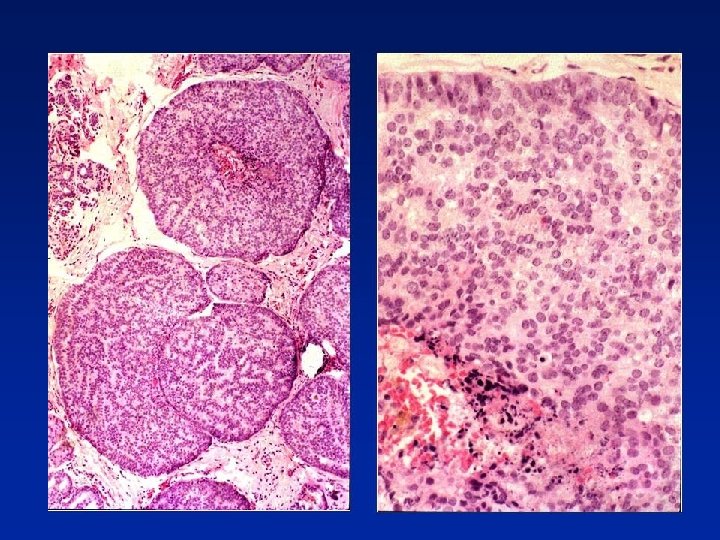
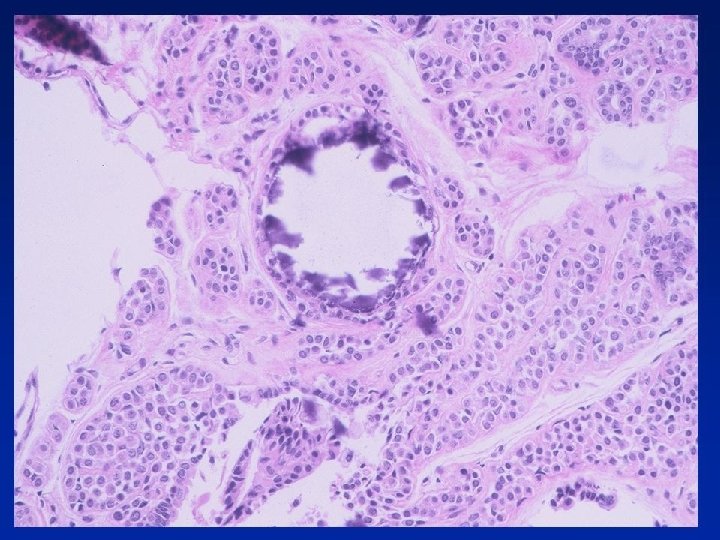
LCIS Vs. Low Grade Solid DCIS • Both processes - filling of membrane-bound spaces by uniform, regularly-placed cells with clear cytoplasm • DCIS - sharply defined cell membranes • LCIS - discohesion • Intracytoplasmic lumina more often in LCIS • Low power view - lobulo-centricity of LCIS, more haphazard lobular & duct distortion in DCIS • If features of both then classify as LCIS & DCIS because of bilateral & precursor risk
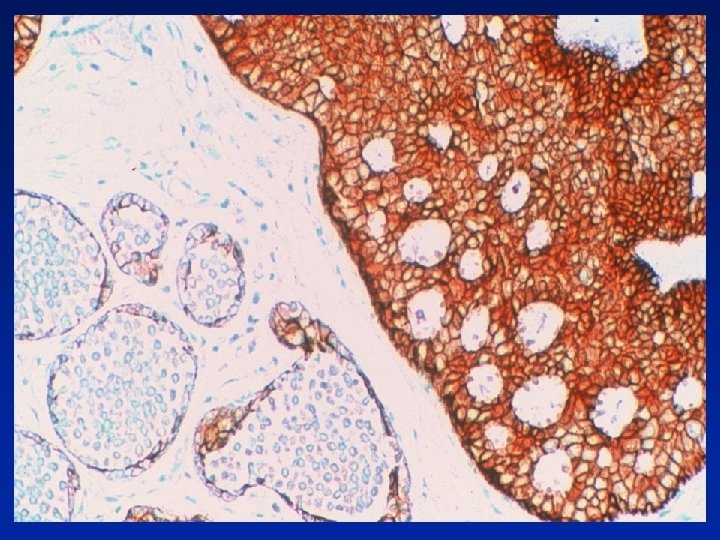
 E-cadherin heterogeneous Jacobs")
E-Cadherin • • 17 of 28 cases of indeterminate CIS (61%) E-cadherin heterogeneous Jacobs TW. Am J Surg Pathol 2001; 25: 229 -36 • 23 of 50 indeterminate CIS = ductal or lobular on immunoprofile In 27 IHC not typical of DIN or classic LIN Bratthauer GL et al. Hum Pathol. 2002; 33: 620 -7 • • • Group of lesions with overlapping morphological & IHC profile At present, regard as combined LCIS & DCIS because of the ? bilateral risk & precursor risk? respectively

Lobular in Situ Neoplasia • • Follow-up of 39 of 48 patients 0. 5% of 10, 542 benign breast biopsies Higher risk with LCIS (9 x) Lower risk with ALH (4 -5 x) Page DL. Human Pathol. 1991; 22; 1232 -1239

Genetics of Lobular Neoplasia • • CGH of 31 LCIS, 14 ALH Loss from 16 p, 16 q, 17 p & 22 q & gain from 6 q found at similar high frequency in LCIS & ALH Lu YJ. Cancer Res. 1998. 15; 58: 4721 -7 • • Low average rate of copy no. changes High rate gains & losses of material at 1 q & 16 q Buerger H et al. Mol Pathol. 2000; 53: 118 -21 • • ALH and LCIS are at similar genetic stage High degree of genetic homology with low grade DCIS
 as well as of increased risk")
LCIS • Marker of adjacent malignancy (? precursor) as well as of increased risk of subsequent carcinoma in either breast?

Update - Risk with LISN Meta-analysis 9 studies of 228 patients 15% ipsilateral, 9% contralateral carcinoma Ipsilateral 3 x more likely than contralateral • A “model of premalignancy for ALH intermediate between a local precursor and a generalised risk for both breasts” Page DL. Lancet. 2003; 361: 125 -9
) • • Lack E-cadherin & beta-catenin Gain")
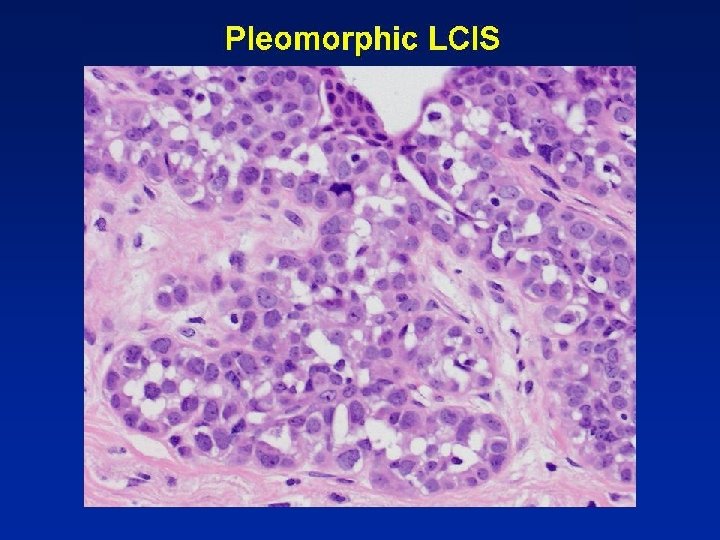
Pleomorphic LCIS (& Pleomorphic Apocrine LCIS (PALCIS)) • • Lack E-cadherin & beta-catenin Gain of 1 q & loss of 16 q - typical of lobular carcinoma Amplification of c-myc and HER 2 Same precursor or same genetic pathway as classic lobular carcinomas Reis-Filho J et al. J Pathol. 2005. • • • Lobular immunohistochemical profile & genetics More “aggressive” re proliferation, HER 2 etc Very limited data on clinical behaviour
 • CAPSS in 42% of 100")
Columnar alteration with prominent snouts & secretions (CAPSS) • CAPSS in 42% of 100 consecutive bxs for microcalcifications • Calcifications in CAPSS in 74% Fraser JL et al. Am J Surg Pathol. 1998; 22: 1521 -7

Columnar cell lesions • • • Blunt duct adenosis Atypical cystic lobules Cancerization of small ectatic ducts of the breast by ductal carcinoma in situ cells with apocrine snouts Hypersecretory hyperplasia Columnar alteration with prominent apical snouts and secretions (CAPPS) Mammary ductal intraepithelial neoplasia-flat type “Clinging ductal carcinoma in situ" Hyperplastic Unfolded Lobules (HULs) Enlarged lobular units with columnar alteration (ELUCA) Columnar cell lesions

Terminology Schnitt and Vincent-Salomon, 2003 • Columnar cell change • Columnar cell hyperplasia • Columnar cell change with atypia • Columnar cell hyperplasia with atypia

Terminology • Columnar cell change • Columnar cell hyperplasia • Columnar cell change with cytological atypia • Columnar cell change with architectural atypia

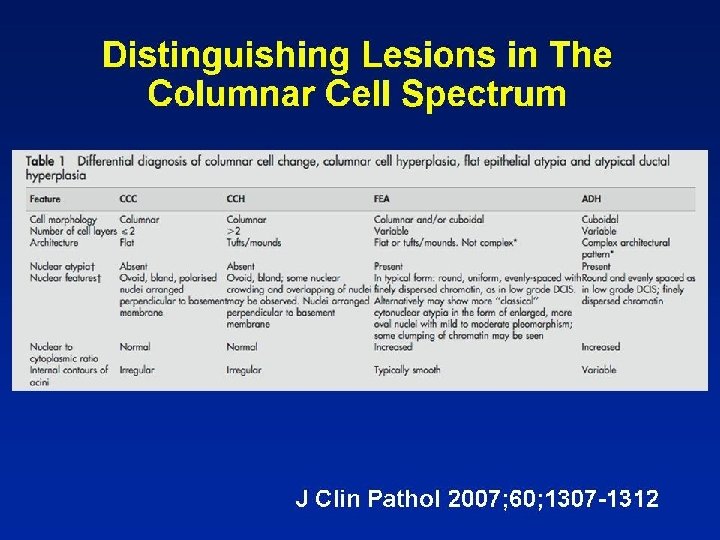
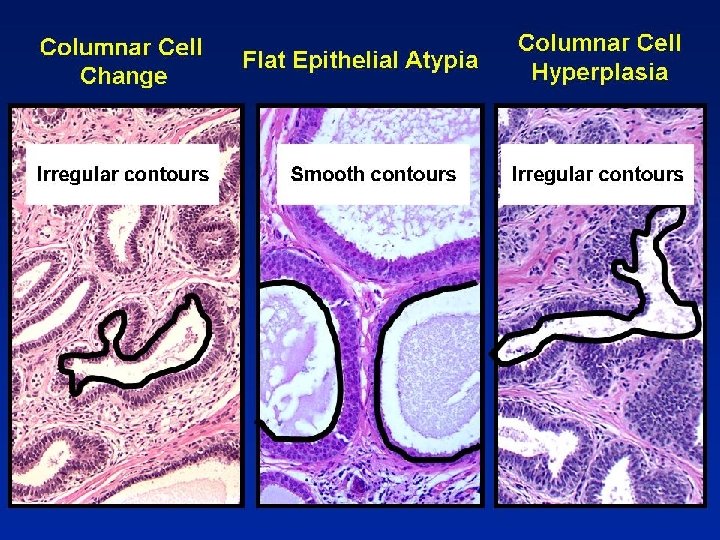
Present Terminology • Columnar cell change • Columnar cell hyperplasia • Flat epithelial atypia
 line •")
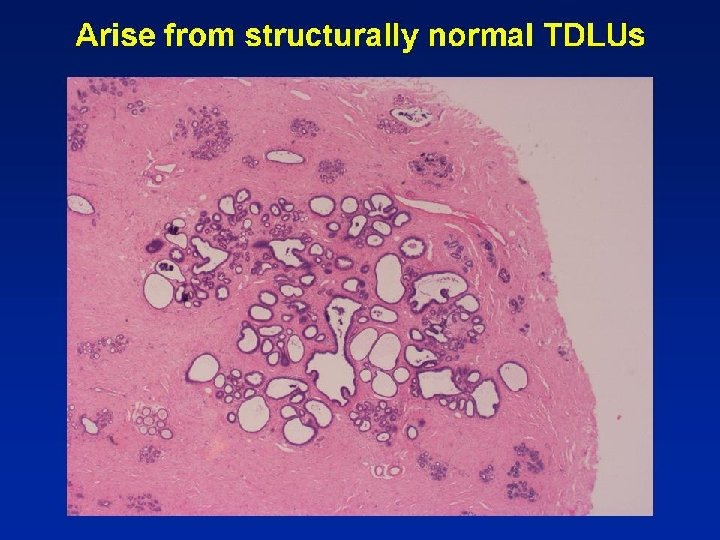
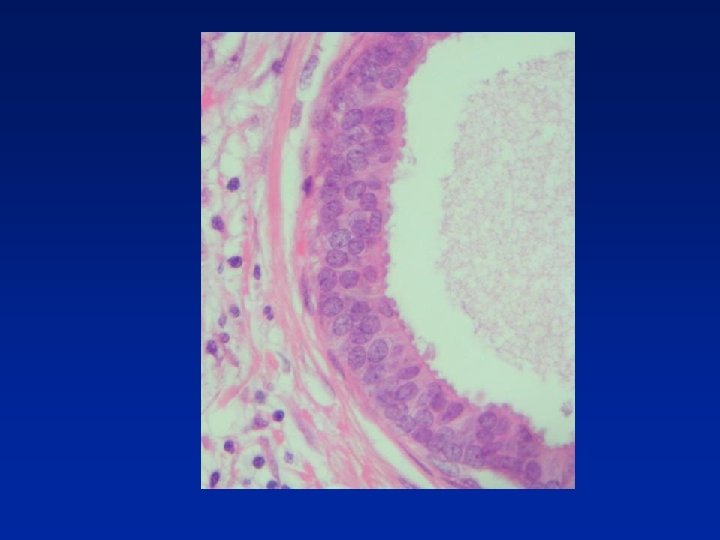
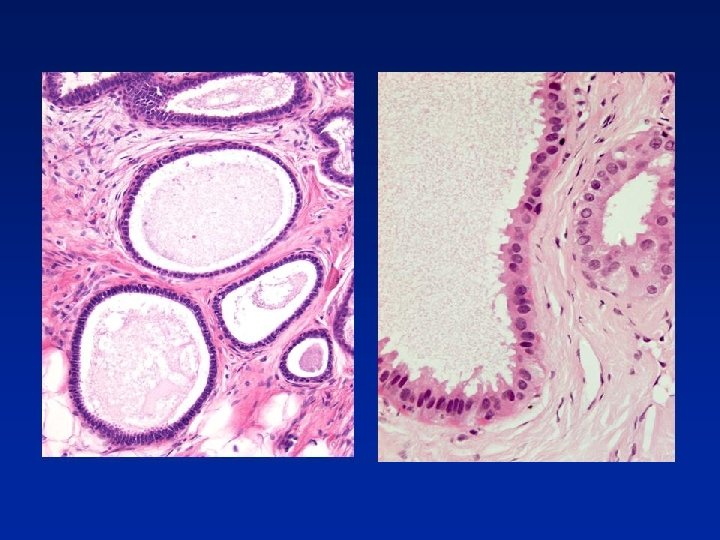
Columnar Cell Change • Columnar epithelial cells (1 or 2 cell depth) line • • • TDLU, often mildly dilated Uniform, ovoid nuclei Perpendicular to basement membrane Cytologically bland Mitotic figures rare Apical snouts often present Secretions may be present in lumen with Ca 2+
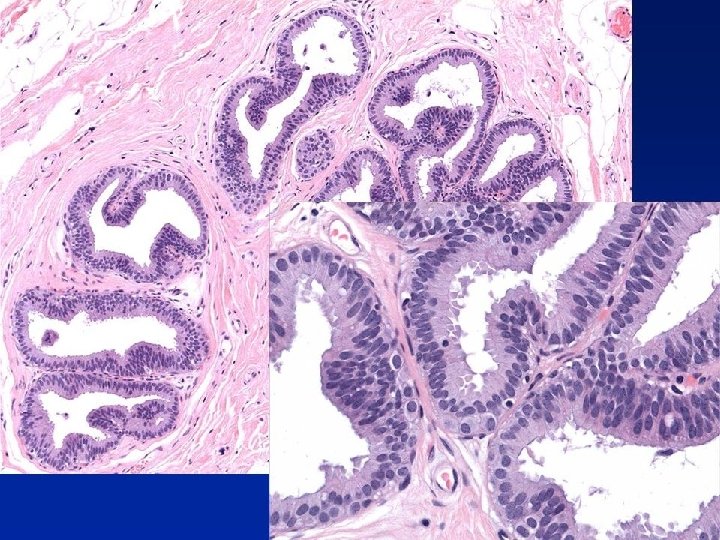
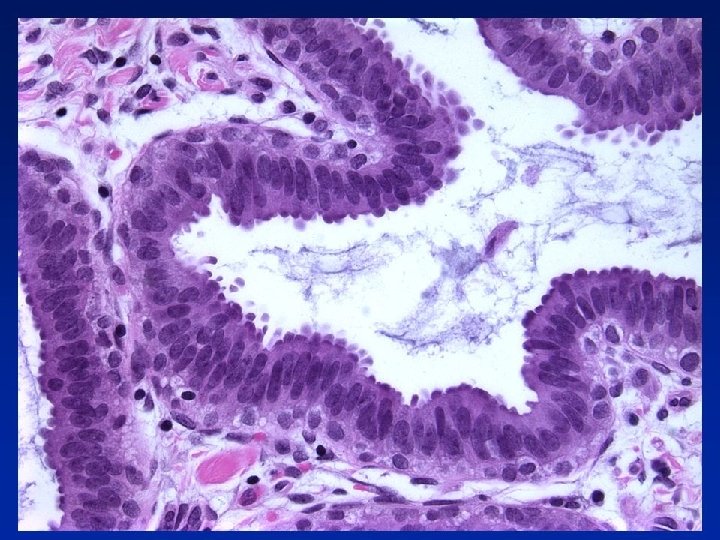

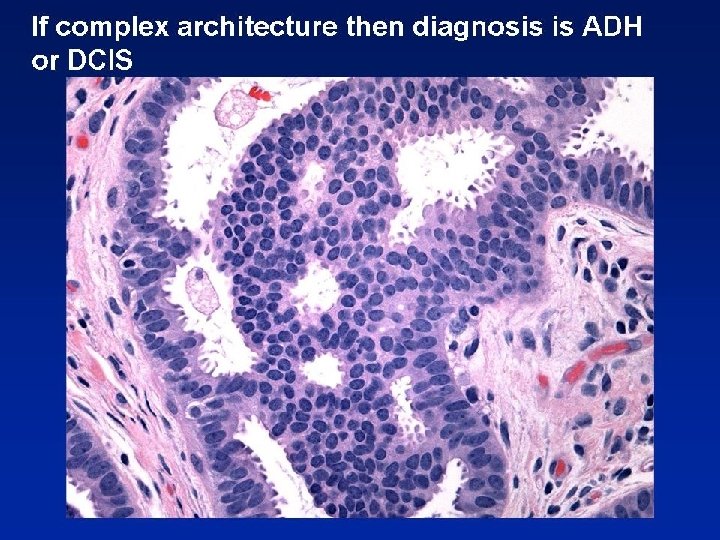
Columnar Cell Hyperplasia • Similar to CCC, but stratification > 2 cells depth • Nuclei morphology as in CCC • May be more crowding & overlapping of nuclei • Tufts or hummocks mimicking micropapillae • Exaggerated apical snouts - hobnail appearance • Intraluminal secretions often with Ca 2+ N. B. If true micropapillae, bridges, cribriform pattern etc = consider as ADH/DCIS

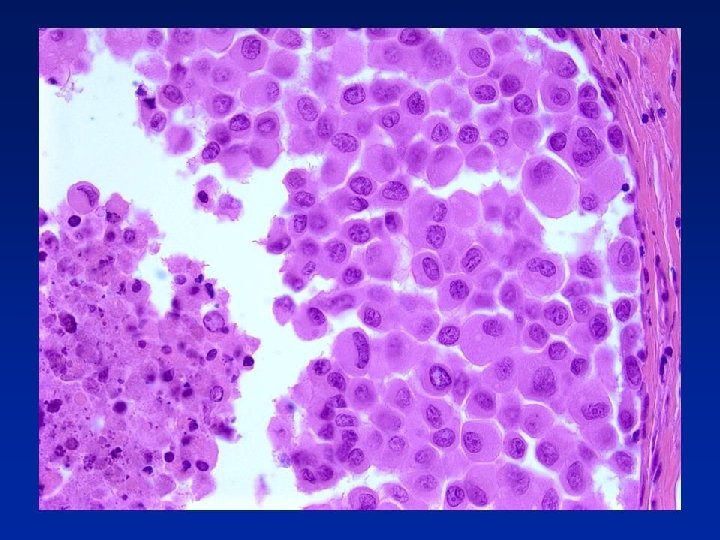
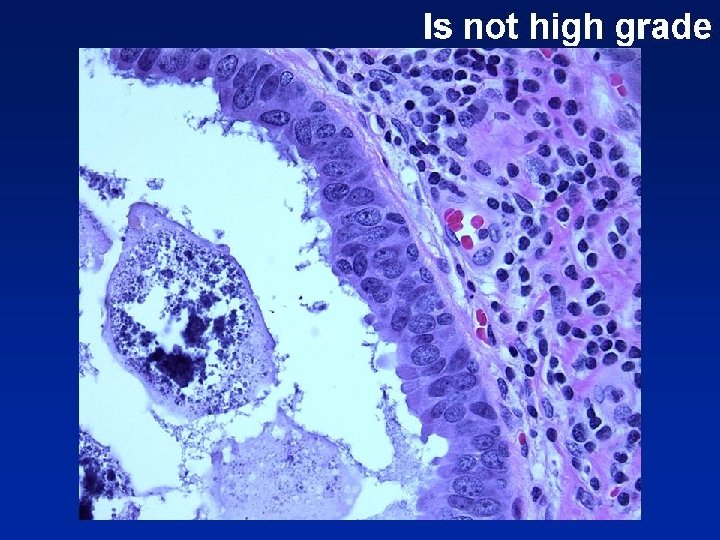
Flat Epithelial Atypia • TDLUs often darker than normal at low power • 1 or more layers of monotonous, cuboidal to • • • columnar cells, resembling LG DCIS Round nuclei Mild increase in nuclear/cytoplasmic ratio Dispersed or marginated chromatin Nucleoli sometimes more prominent Mitotic figures rare May be scattered lymphoid cells


Not necessarily flat
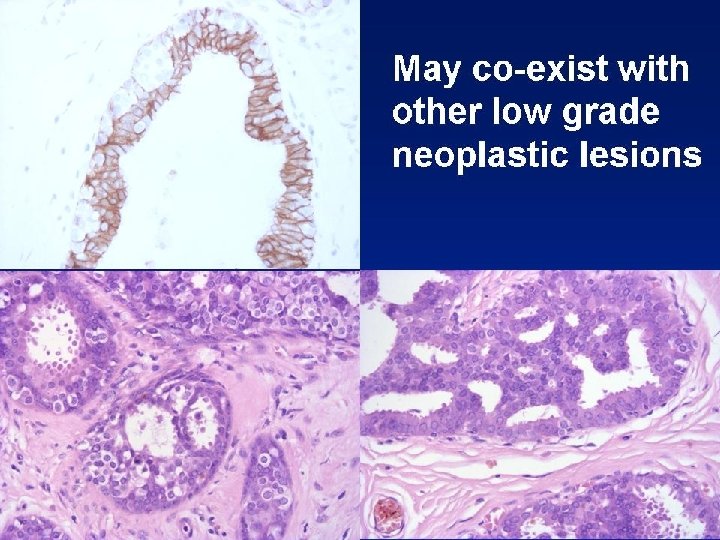

Columnar Cell Lesions • Cells of columnar cell lesions show luminal • • cytokeratin (e. g. CK 19) positivity No expression with cytokeratins 5 or 14 Strong homogeneous nuclear oestrogen & progesterone receptor & bcl-2 positivity IHC not helpful in distinguishing FEA from CCC or CCH May be helpful if apocrine change or microcysts are differential diagnoses
f9de59b72888cbfeca730643543dcae0.ppt