ae51c33f979b3c6c54c87720a60a4c70.ppt
- Количество слайдов: 58



International Seminar on the Public Health Aspects of Noncommunicable Diseases Lausanne -Geneva Finland’s experience in implementing NCD prevention Dr. Tiina Laatikainen, Director Department of Chronic Disease Prevention Erkki Vartiainen, MD, Professor, Assistant Director General 18/03/2018 CVD prevention/ Tiina Laatikainen 1

5

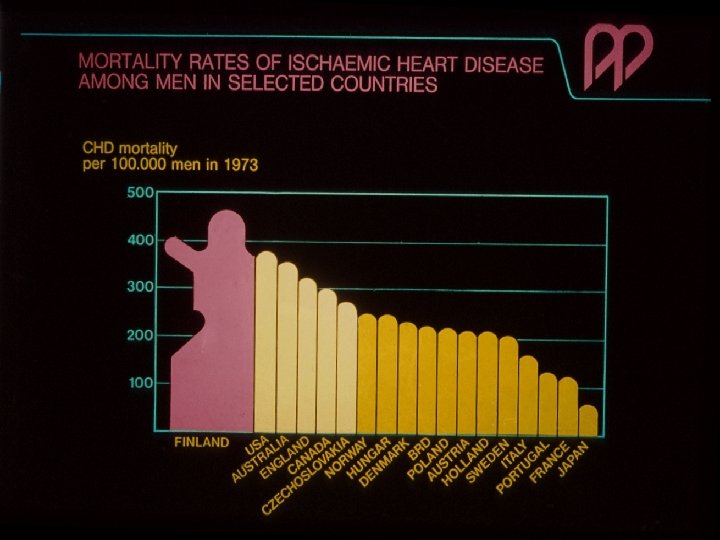
In the 1970’s • • • Statistics showed very bad public health situation CHD mortality rates among men highest in the world Short life expectancy Increasing public discussion General opinion related CHD to stress, ageing and genetics (but little to lifestyle) • CHFD also referred to as “Disease of the Executives” • Cardiologists were aware that there are numerous “Statistical Associations”

Frequency % Serum cholesterol distribution in Finland Japan in the 1970 s mmol/l

Two main questions in 1970 s • Can risk factors and behaviors be changed on population level ? • If risk factors reduce what will happen to the mortality?

North Karelia Project Aims of the North Karelia Project MAIN OBJECTIVE: – Initially: – Later: To reduce CVD mortality To reduce major chronic disease mortality and promote health INTERMEDIATE OBJECTIVES: – To reduce the population levels of main risk factors, emphasizing lifestyle changes and to promote secondary prevention NATIONAL OBJECTIVE: – Initially: – Later: To be pilot for all Finland To be demonstration and model program

Main Principles of the North Karelia Project • Primary prevention is the only sustainable approach • Community based preventive programme 1 Target: the community (not individuals) 2 Intervention: through changes in the community organization/structures (not external intervention) • Risk factors identified by prospective studies, closely linked with certain behaviours - deeply enrooted in the community • - smoking - elevated serum cholesterol (diet) - elevated blood pressure

CLINICAL INTERVENTION RISK FACTORS PUBLIC HEALTH INTERVENTION

5% People with low risk factor level 70 % People with average risk factor level 25 % People with clinically high risk factor level Individual risk of CHD Distribution of people according to risk factor level Theoretical presentation of the difference between individual risk and the proportional attributable risk

Constraints • • Suspicions from the scientific community of cardiologists Medical knowledge on prevention questionable: community prevention new concept North Karelia socially deprived area, poor and with many social problems (unemployment, migration, shortage of doctors etc) Post war years: great poverty, then increase in consumption Dairy farming main agriculture: butter and animal fat culturally highly valued Strong commercial pressures (“FAT WAR”), supported by political pressures Raising the funding (intervention and evaluation research) To maintain interest and funding over decades

Advantages • Magnitude of problem, concern of people • Relatively homogenous population, traditions of community action • Trust in experts and in public action • Good information system • Good collaboration with people • Good leadership

Community intervention model of the North Karelia Project

North Karelia Project Practical intervention • • • Emphasis on persuasion, practical skills, social & environmental support for change Research team & local project office with comprehensive community involvement Main areas: 1. Media activities (materials, mass media, campaigns) 2. Preventive services (primary health care etc. ) 3. Training of professional and other workers 4. Environmental changes (smoke-free areas, supermarkets, food industry etc. ) 5. Monitoring and feed-back

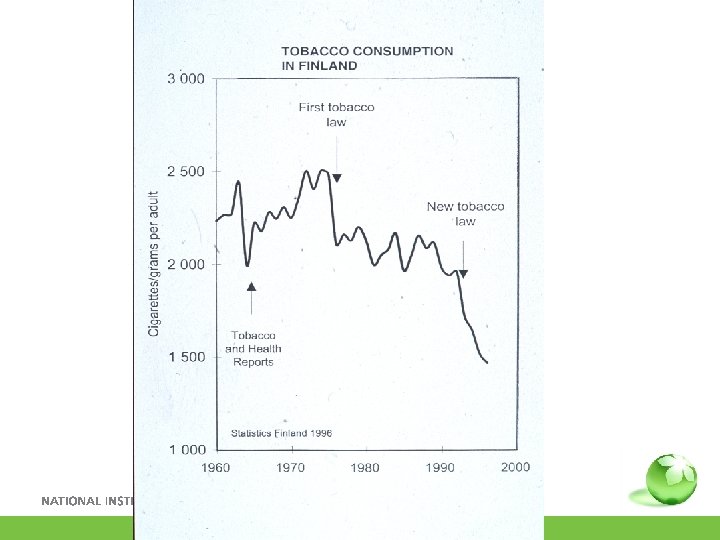
ANTISMOKING LEGISLATION IN FINLAND IN 1977: • Prohibition of all forms of advertising • Restrictions in smoking in public places • Health warnings etc. • 1/2% level of tobacco tax for antismoking activities • Prohibition of sale to under 16 years old ANTISMOKING LEGISLATION IN FINLAND IN 1995, 2000 AND 2007: • Worksite smoking policy • Sales to persons under 18 years of age prohibited • Restaurant, bar smoking policy

Smoking control programmes • • • Worksite programmes School programmes TV programmes Radio programmes Smoke Free Class Competition Quit and Win - Do Not Start and Win for Young People

A comprehensive television smoking cessation programme in Finland • • Voluntary smokers in TV studio tried to stop smoking 6 sessions + 2 follow-up sessions Intensified field activity in North Karelia 250 000 saw at least 4 sessions 30 000 attempted to quit 20 000 quitted 10 000 remained non-smokers

North Karelia Project Cholesterol programme • SPECIAL INTENSIFIED PROGRAM - New consensus recommendations - New reference values (< 5 mmol/L = “normal”) - Fingertip determination method - Interest of food industry - Finnish rapeseed oil • MAIN COMPONENTS - Population-wide cholesterol measurements - Dietary counseling - Mass media and many campaigns (incl. Village competition) - Collaboration with industry and supermarkets
 organization • Active co-operation since 1972 • Several hundred")
Co-operation with the Martta (housewifes’) organization • Active co-operation since 1972 • Several hundred clubs and many thousand members • Promotion of healthy cooking = dietary habits • Many special campaigns, notably: - “Parties for longlife” 1976 -77 - Evenings of “Happy Heart” 1990 -91

Use of lay opinion leaders to promote health innovations in community • • Innovation-diffusion theory Training seminars in municipalities Discuss health issues in normal life 805 persons participated Recruitment by local people and Heart Association 1975 -1982 Evaluation in 1982: 399 (50%) still active

Fruits And Vegetables – Supermarkets

Village competition to lower cholesterol • • • 1991: 7 villages, population 105 -210 1997: 16 villages, population 85 -420 Village committees organized 2 months competition Baseline and follow-up cholesterol measurement Best village won 2000 €

Cholesterol changes in 1991 competition Village Baseline % Change 1 5. 9 -10. 8 2 5. 8 -9. 2 3 5. 9 -8. 9 4 5. 9 -6. 8 5 6. 0 -4. 0 6 5. 7 -2. 3 7 5. 7 +1. 4 Mean 5. 8

North Karelia Project Berry project • Aim to increase the consumption of eastern Finnish berries • Rationale: 1) Berries are healthy 2) Enhances switch from dairy farming • First Berry Project 1985 -90 • Second Berry Project 1992 • Methods: various co-operative and innovative interventions • Funding from government

Examples of intersectoral work 1. Development of Finnish Rapeseed oil Change in SFA content of Finnish cow milk
: • Leading Finnish biscuit manufacturer")
Examples of intersectoral work 2 Biscuit example (trans fat): • Leading Finnish biscuit manufacturer (LU Finland Ltd) has removed some 80. 000 kg of SFA by changing the fats used • All trans fats removed and major transfer to rapeseed oil Meat product example (SFA): HK (Leading Finnish meat company) since 2007 annually: • 60. 000 kg less salt • 100. 000 kg less SFA in their products (will be increased to 500 000 kg due to change in pig feeding) The average salt content of HK products

Changes in Finnish food habits Year

Fat used for cooking at home in Finland in 1978 -2006 Health Behaviour among the Finnish Adult Population 1978– 2006

Cholesterol distribution in North Karelia in 1972 and 2007, men 4 6 8 10 12 mmol/l

Salt intake in Finland 1977 -2007 g/day The FINDIET Study
 mm. Hg North Karelia project evaluation")
Systolic blood pressure in men (30– 59 y) mm. Hg North Karelia project evaluation and FINMONICA and the National FINRISK Studies 1972 - 2007

Decline in CHD mortality in men aged 35 -64 per 100 000 North Karelia All Finland

Observed and Predicted Decline in CHD mortality 35 -64 year old men Vartiainen E et al.

CHD mortality fall in Finland 1982 – 1997 Risk Factors Cholesterol Smoking Blood pressure Treatments - 53% - 11% - 7% -24% AMI treatments - 4% Secondary prevention - 8% Heart failure - 2% Angina: CABG & PTCA - 8% Angina: Aspirin etc - 2% 373 fewer deaths 1982 -71% Other Factors 1997 T Laatikainen et al Am J Epid 2005 -5%

Finland Has Shown • Prevention of major chronic diseases is possible and pays off • Population based prevention is the only cost effective and sustainable public health approach to chronic disease control • Prevention of CVD calls for simple changes in some lifestyles (individual, family, community, national and global level action) • Many results of prevention occur surprisingly quickly (CVD, diabetes) • Comprehensive action, broad collaboration with dedicated leadership and strong government policy support are crucial

Why success in North Karelia • Appropriate epidemiological and behavioural framework • Restricted, well defined targets • Good monitoring of immediate targets (behaviours, processes) • Emphasis in changing environment and social norms • Working closely with the community • Work with media • International collaboration, support from WHO • Close interaction with national health policy, integration with National Public Health Institute • Long term, dedicated leadership

Major Elements of Finnish National Action • • Research & international research collaboration Health services (especially primary health care) North Karelia Project, other demonstration programmes Health Promotion Programs (coalitions, NGOs, media, etc) Schools, educational institutions Collaboration with industry, business Policy decisions, intersectoral collaboration, legislation Monitoring system: health behaviours, risk factors, nutrition

Work sites Education Food industry Taxation Working intersectorally Media Business Legislation Research Agriculture Third sector Health services

PUBLIC POLICY POPULATION PRIVATE SECTOR HEALTH PROGRAMME

North Karelia Project Conclusions • A comprehensive, determined and theory-based community program can have a meaningful positive effect on risk factors and life styles • Such changes are associated with respective favorable changes in chronic disease rates and health of the population • A major national demonstration program can be a strong tool for favourable national development in chronic disease prevention and health promotion

New textbook on North Karelia project Pekka Puska, Erkki Vartiainen, Tiina Laatikainen, Pekka Jousilahti, Meri Paavola (eds. ) The North Karelia project: from North Karelia to national action http: //www. thl. fi/thlclient/pdfs/731 beafd-b 544 -42 b 2 b 853 -baa 87 db 6 a 046 Also available in Russian

Training seminar on NCD prevention www. thl. fi/ncdseminar Helsinki, Finland in North Karelia 12 -16 March, 2012 11 -15 March, 2013

18/03/2018 Presentation name / Author 44

Fat intake Recommendations EN% Year The FINDIET Study
 in cholesterol value by village activity")
Change (%) in cholesterol value by village activity

Serum cholesterol in men aged 30 -59 years mmol/L
 Occasionally(%) Family 43 41 Neighbors")
Discussions with target groups Target group Very often (%) Occasionally(%) Family 43 41 Neighbors 18 60 Work 16 31 Relatives 20 48 Friends 18 46 NGO meetings 13 28 Shopkeepers 8 27 Media 0 15
 association")
NGO’s role • Heart Association • Martta (house wife’s) association
 % North Karelia project evaluation and FINMONICA and")
Smoking in men (30– 59 y) % North Karelia project evaluation and FINMONICA and the National FINRISK Studies 1972 - 2007

Cholesterol change in 1997 competition Baseline End Change% N 6. 19 5. 59 -0. 60 -9. 0 16

18/03/2018 Presentation name / Author 52

Health in All Policies – The Finnish Initiative
 approach? – Horizontal, complementary policy related")
What is Health in All Policies (Hi. AP) approach? – Horizontal, complementary policy related strategy – The core of Hi. AP is to examine determinants of health -> are mainly controlled by policies of sectors other than health – Addresses policies in the context of policy-making at all levels of governance (global, European, national, regional and local levels) – The ultimate aim of Hi. AP is to improve evidence informed policy-making Ståhl et al. (eds). Health in All Policies – Prospects and potentials, 2006

Focus on policies • Key concern: policies – The broad economic, social, environmental and cultural health determinants are the bridge between policies and health outcomes – For example, alcohol policy (tax) influences the price of alcohol that has an effect on alcohol consumption that (alcohol abuse) in turn has an effect on harms, both health and social alcohol policy tax on alcohol consumption health and social harms – Less concerned with single programmes and projects

Broad determinants of health § § Social, economic, structural, environmental, cultural Present everywhere in the society Often beyond the control of individuals Same determinants are linked with many major public health problems (nutrition, physical activity, tobacco, alcohol, psychosocial situation, stress) § Mostly a responsibility of other government sectors § Impossible to target effectively through sectorial health policies alone

Intersectoral mechanisms/tools for implementing Hi. AP – – – Formal consultations on e. g. legislation Horizontal public health committees Ad hoc committees on specific initiatives Cross-sectorial programmes Public health reporting (with co-operation of other sectors) Formal communication between sectors (e. g. bilateral meetings of Permanent Secretaries) – Informal contacts at desk level – EU co-ordination – Health impact assessment Stahl T (2009) Is health recognized in the EU's policy process? An analysis of the European Commission's impact assessments. The European Journal of Public Health 2009; doi: 10. 1093/eurpub/ckp 082
 kg 140 Whole")
Milk Consumption in Finland in 1970 and 2006 (kg per capita) kg 140 Whole milk 120 100 Low fat milk 80 60 Whole form milk 40 20 0 1960 Skim milk 1970 1980 1990 2000 2010
ae51c33f979b3c6c54c87720a60a4c70.ppt