

02deb6d2932f97f55c275d2e81c1e3ce.ppt
- Количество слайдов: 54
 Interesting Case Rounds Nadim J Lalani 20. 07. 2006
Interesting Case Rounds Nadim J Lalani 20. 07. 2006
 Patient C. B : 53 y. o. ♀ n Transferred to FMC CCU from Red Deer with Acute MI n PMHx: HTN Depression Etoh Abuse COPD on home O 2 VP shunt 1996 [Obtructive Hydrocephalus due to benign mass] shunt revision ‘ 98
Patient C. B : 53 y. o. ♀ n Transferred to FMC CCU from Red Deer with Acute MI n PMHx: HTN Depression Etoh Abuse COPD on home O 2 VP shunt 1996 [Obtructive Hydrocephalus due to benign mass] shunt revision ‘ 98
 Pt C. B. Meds: Avalide Wellbutrin Imipramine Effexor Tryptophan n Smoker has many cats n
Pt C. B. Meds: Avalide Wellbutrin Imipramine Effexor Tryptophan n Smoker has many cats n
 HPI: n March 17 n experiencing chest pain and HA Agitated, was pacing & collapsed EMS to Innisfail Hospital In ED: Vitals: 369, hr 119, 35, 106/80, Some respiratory distress. Neuro: “Confused but following commands” R pupil 5 mm > L 4 mm plantar response: ↑ ↑ Agitated
HPI: n March 17 n experiencing chest pain and HA Agitated, was pacing & collapsed EMS to Innisfail Hospital In ED: Vitals: 369, hr 119, 35, 106/80, Some respiratory distress. Neuro: “Confused but following commands” R pupil 5 mm > L 4 mm plantar response: ↑ ↑ Agitated
![Innisfail ED [cont’d]: n Given: Asthma cocktail Ativan for agitation n Transferred to Red](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-5.jpg "Innisfail ED [cont’d]: n Given: Asthma cocktail Ativan for agitation n Transferred to Red") Innisfail ED [cont’d]: n Given: Asthma cocktail Ativan for agitation n Transferred to Red Deer: Confusion / agitation / sob
Innisfail ED [cont’d]: n Given: Asthma cocktail Ativan for agitation n Transferred to Red Deer: Confusion / agitation / sob
 Red Deer Hospital: Confused, agitated, restless, intermittent fevers n Vitals: Afeb 120, 24, 100/75, 93% Altered LOC, GCS 6, pupils variable ? ↑ tone, rambling speech n
Red Deer Hospital: Confused, agitated, restless, intermittent fevers n Vitals: Afeb 120, 24, 100/75, 93% Altered LOC, GCS 6, pupils variable ? ↑ tone, rambling speech n
![Red Deer Hospital [cont’d] n Initial Labs: ABG: 7. 37/41/116/24 Hb 137, WBC 15.](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-7.jpg "Red Deer Hospital [cont’d] n Initial Labs: ABG: 7. 37/41/116/24 Hb 137, WBC 15.") Red Deer Hospital [cont’d] n Initial Labs: ABG: 7. 37/41/116/24 Hb 137, WBC 15. 2, Plt 264 CK 559 (< 140 u/L) Acetominophen/ ETOH/ ASA: all NEG
Red Deer Hospital [cont’d] n Initial Labs: ABG: 7. 37/41/116/24 Hb 137, WBC 15. 2, Plt 264 CK 559 (< 140 u/L) Acetominophen/ ETOH/ ASA: all NEG
 n n n CXR: Hyperinflation EKG: N Admitted with the following issues: COPD ? Seratonin Syndrome ? Etoh Withdrawal
n n n CXR: Hyperinflation EKG: N Admitted with the following issues: COPD ? Seratonin Syndrome ? Etoh Withdrawal
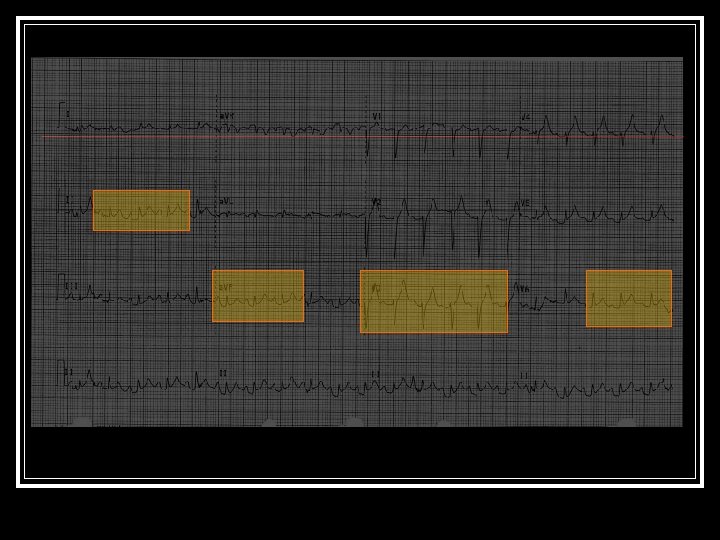
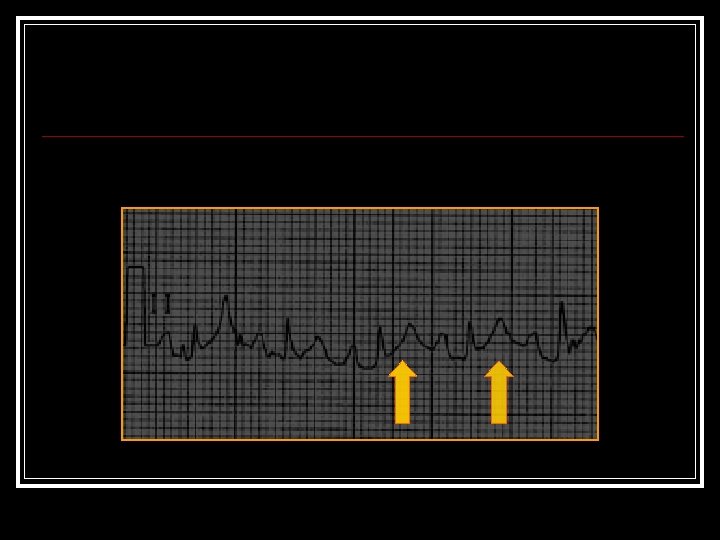
![Red Deer Hospital [Cont’d] n n Next 24 - 48 H: Improved on IV](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-9.jpg "Red Deer Hospital [Cont’d] n n Next 24 - 48 H: Improved on IV") Red Deer Hospital [Cont’d] n n Next 24 - 48 H: Improved on IV fluids, multi-vits Solu-medrol & withholding psyc meds. March 20: breathlessness, ↓ LOC CXR: mild oedema ABG: 7. 35/72/135/40 Intubated had following EKG:
Red Deer Hospital [Cont’d] n n Next 24 - 48 H: Improved on IV fluids, multi-vits Solu-medrol & withholding psyc meds. March 20: breathlessness, ↓ LOC CXR: mild oedema ABG: 7. 35/72/135/40 Intubated had following EKG:
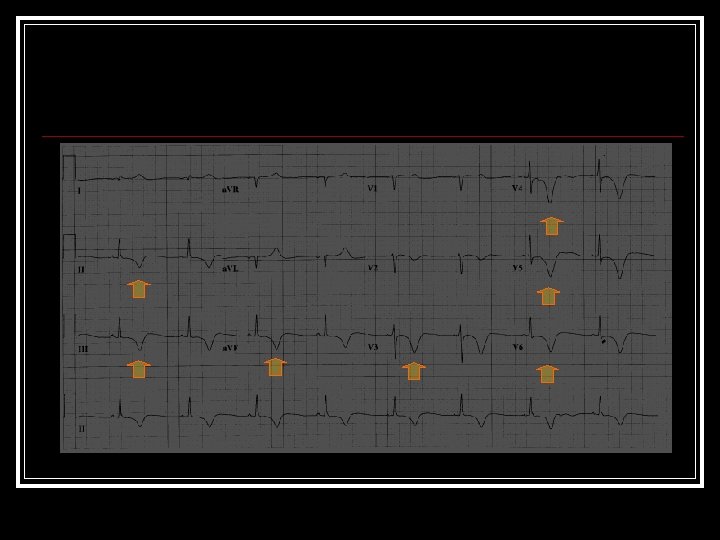
![Red Deer Hospital [cont’d] n n n Next 24 H: extubated, more alert &](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-13.jpg "Red Deer Hospital [cont’d] n n n Next 24 H: extubated, more alert &") Red Deer Hospital [cont’d] n n n Next 24 H: extubated, more alert & lucid EKG: T-wave changes Echo: akinetic apex TNi 7. 11 (0 -0. 10 ug/L) (>1. 5 ug/L= MI) CK 1751 CT head: Reported as Normal Pt transferred to FMC Cardiology Dx: MI on Nitro drip and Heparin
Red Deer Hospital [cont’d] n n n Next 24 H: extubated, more alert & lucid EKG: T-wave changes Echo: akinetic apex TNi 7. 11 (0 -0. 10 ug/L) (>1. 5 ug/L= MI) CK 1751 CT head: Reported as Normal Pt transferred to FMC Cardiology Dx: MI on Nitro drip and Heparin
 En route to Foothills Hospital: n Patient: became lethargic, gasping GCS decreased to 8 pupils unequal intubated (again)
En route to Foothills Hospital: n Patient: became lethargic, gasping GCS decreased to 8 pupils unequal intubated (again)
![Foothills Hospital CCU [Mar 22]: n Exam: VSS Intubated, withdrawing, opens eyes to pain](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-15.jpg "Foothills Hospital CCU [Mar 22]: n Exam: VSS Intubated, withdrawing, opens eyes to pain") Foothills Hospital CCU [Mar 22]: n Exam: VSS Intubated, withdrawing, opens eyes to pain reflexes 4+ LE’s ? ↑↑ tone , 4 beat clonus shunt depresses and fills completely
Foothills Hospital CCU [Mar 22]: n Exam: VSS Intubated, withdrawing, opens eyes to pain reflexes 4+ LE’s ? ↑↑ tone , 4 beat clonus shunt depresses and fills completely
 What’s going on?
What’s going on?
 CCU: n Gets Repeat CT
CCU: n Gets Repeat CT
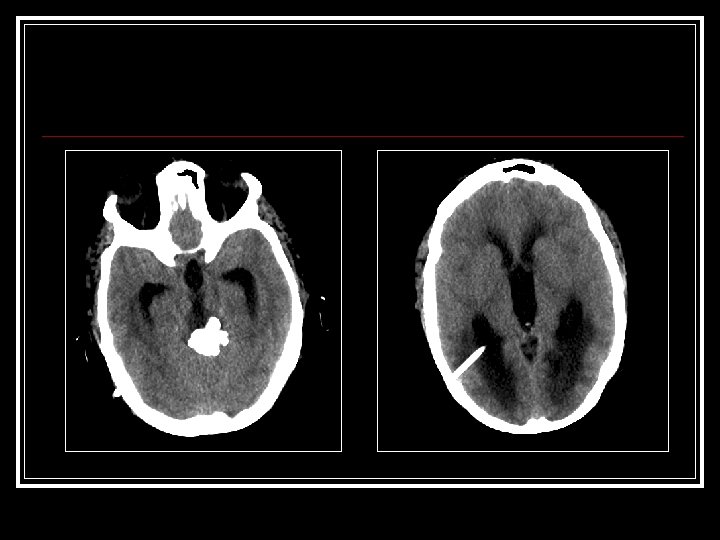
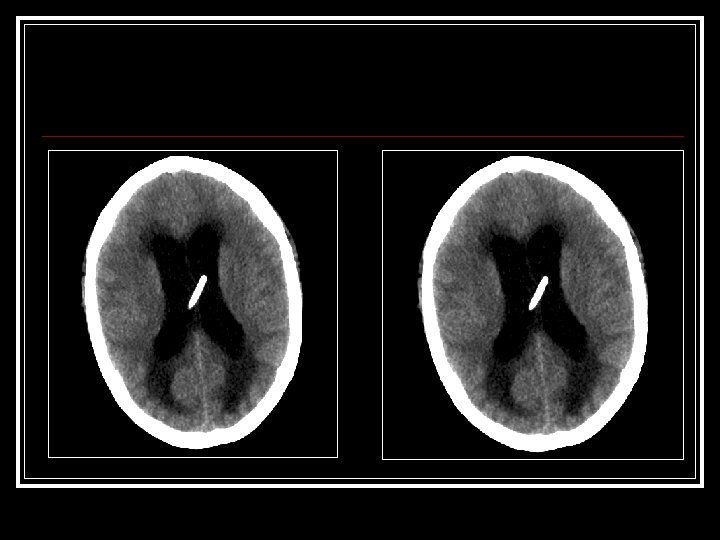
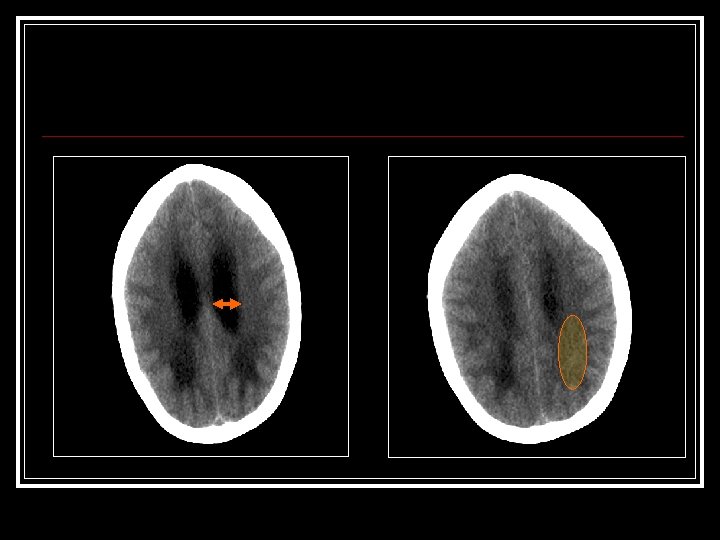
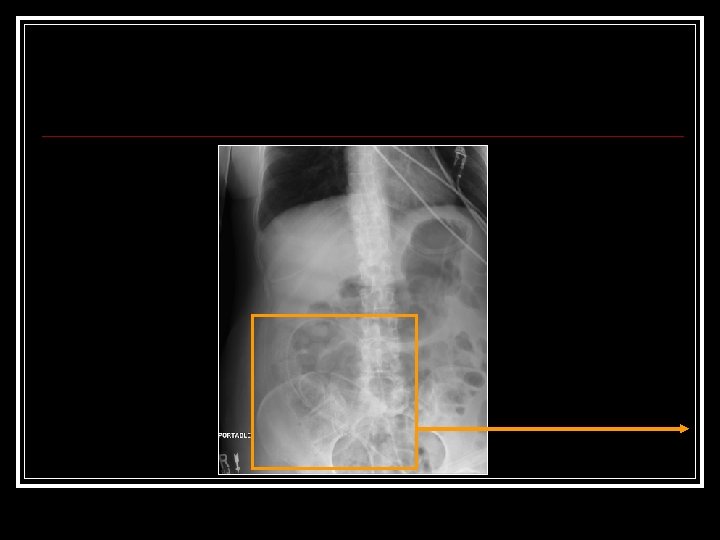
![March 22 [cont’d] n n n Neuro. Surgery Consulted ? Shunt Malfxn Initial exam:](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-21.jpg "March 22 [cont’d] n n n Neuro. Surgery Consulted ? Shunt Malfxn Initial exam:") March 22 [cont’d] n n n Neuro. Surgery Consulted ? Shunt Malfxn Initial exam: Intub, withdrawing disconjugate gaze Drain off 20 cc via shunt reservoir Pt immediately awakes, begins reaching for ETT Cannot palpate distal shunt got AXR:
March 22 [cont’d] n n n Neuro. Surgery Consulted ? Shunt Malfxn Initial exam: Intub, withdrawing disconjugate gaze Drain off 20 cc via shunt reservoir Pt immediately awakes, begins reaching for ETT Cannot palpate distal shunt got AXR:
![March 23 -26: Further 20 cc drained off [02: 00 am] n In a.](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-24.jpg "March 23 -26: Further 20 cc drained off [02: 00 am] n In a.") March 23 -26: Further 20 cc drained off [02: 00 am] n In a. m Cardiac cath: Normal Coronaries n Echo: Mild LV hypokinesis n Pt had shunt studies n went to OR third ventriculostomy n Pt does well. Discharged home n
March 23 -26: Further 20 cc drained off [02: 00 am] n In a. m Cardiac cath: Normal Coronaries n Echo: Mild LV hypokinesis n Pt had shunt studies n went to OR third ventriculostomy n Pt does well. Discharged home n
 Hydro. Cephalus First described by Hippocrates n Epidemiology: 1. 2/1000 live births n Disturbance of CSF flow n
Hydro. Cephalus First described by Hippocrates n Epidemiology: 1. 2/1000 live births n Disturbance of CSF flow n
![CSF physiology n n n Secreted by Choroid Plexus [20 ml/h] Passive absorption: SA](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-27.jpg "CSF physiology n n n Secreted by Choroid Plexus [20 ml/h] Passive absorption: SA") CSF physiology n n n Secreted by Choroid Plexus [20 ml/h] Passive absorption: SA space venous system Mostly obstruction [except choroid papilloma]
CSF physiology n n n Secreted by Choroid Plexus [20 ml/h] Passive absorption: SA space venous system Mostly obstruction [except choroid papilloma]
 Myelomeningocoele Other congenital (Aqueductal stenosis &c. ) Brain tumor") Causes of Hydrocephalus Prematurity (posthemorrhagic) Myelomeningocoele Other congenital (Aqueductal stenosis &c. ) Brain tumor Subarachnoid hemorrhage Meningitis
Causes of Hydrocephalus Prematurity (posthemorrhagic) Myelomeningocoele Other congenital (Aqueductal stenosis &c. ) Brain tumor Subarachnoid hemorrhage Meningitis
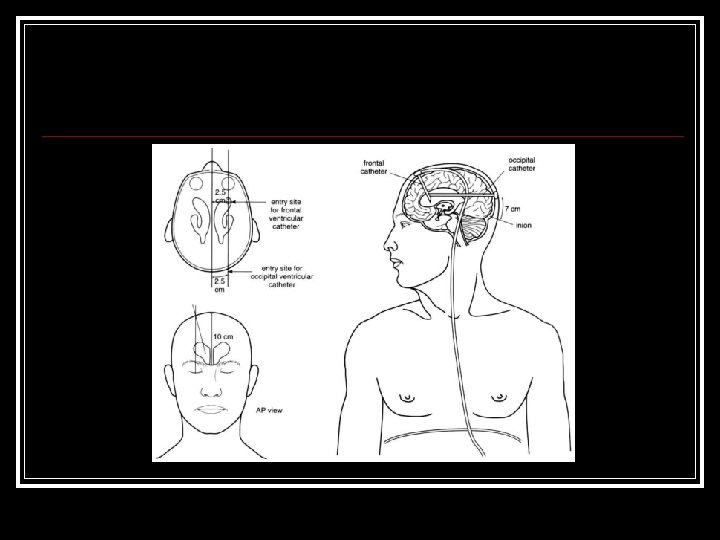
 Shunts n Three Parts: n n Diverted to: n n Ventricular catheter Valve Distal Catheter Peritoneum Pleural Cavity GB, RA, IJ Lumbar CSF Shunts
Shunts n Three Parts: n n Diverted to: n n Ventricular catheter Valve Distal Catheter Peritoneum Pleural Cavity GB, RA, IJ Lumbar CSF Shunts
 Shunts
Shunts
 Shunt Malfunction n Two categories : n n n Shunt Failure Infection : n n n Coag negative Staph Fevers/malaise meningitis Important to r/o in paeds presentation
Shunt Malfunction n Two categories : n n n Shunt Failure Infection : n n n Coag negative Staph Fevers/malaise meningitis Important to r/o in paeds presentation
 Shunt Failure n Shunt Failure: n n n Debris Component failure Fracture/ separation/ migration 30 -40% fail within 1 st year n 15% failure in 2 nd year n After 2 nd year 1 -5% failure /year n Mortality 1 -4% n
Shunt Failure n Shunt Failure: n n n Debris Component failure Fracture/ separation/ migration 30 -40% fail within 1 st year n 15% failure in 2 nd year n After 2 nd year 1 -5% failure /year n Mortality 1 -4% n
![Assessment n Hx: [ incr ICP] n n HA [morning], neck pain N/V Irritability,](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-33.jpg "Assessment n Hx: [ incr ICP] n n HA [morning], neck pain N/V Irritability,") Assessment n Hx: [ incr ICP] n n HA [morning], neck pain N/V Irritability, gait problems, recent VP shunt P/E: n n n Papiloedema CN VI palsy , CN III palsy “Sunsetting” ALOC / Coma Don’t forget to palpate the shunt
Assessment n Hx: [ incr ICP] n n HA [morning], neck pain N/V Irritability, gait problems, recent VP shunt P/E: n n n Papiloedema CN VI palsy , CN III palsy “Sunsetting” ALOC / Coma Don’t forget to palpate the shunt
 Hx & P/E not very sensitive Sens Nausea /Vomit HA ALOC Papilloedema Spec 36 97 15 10 3 97 100
Hx & P/E not very sensitive Sens Nausea /Vomit HA ALOC Papilloedema Spec 36 97 15 10 3 97 100
 Usefulness of balloting the shunt? n Rationale: n n n If it depresses patent distally If it refills patent proximally Reality: n n Sensitivity only 20% in the hands of Nsx! Even “positive” test not useful [25% false]
Usefulness of balloting the shunt? n Rationale: n n n If it depresses patent distally If it refills patent proximally Reality: n n Sensitivity only 20% in the hands of Nsx! Even “positive” test not useful [25% false]
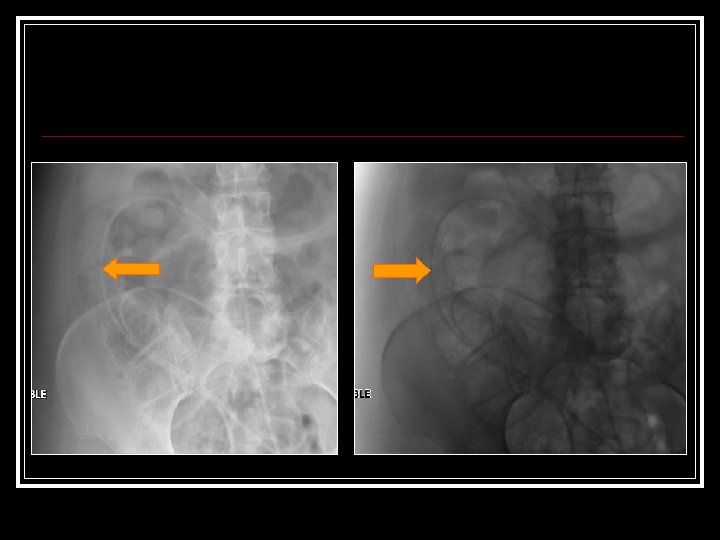
![Radiography? n Shunt Survey [XR skull, Chest , KUB]: n n n CT: n](https://present5.com/presentation/02deb6d2932f97f55c275d2e81c1e3ce/image-37.jpg "Radiography? n Shunt Survey [XR skull, Chest , KUB]: n n n CT: n") Radiography? n Shunt Survey [XR skull, Chest , KUB]: n n n CT: n n Sensitivity 20% LR –ve 0. 82 83% sens LR –ve 0. 21 Combined : 88 sens BUT! n 1 in 8 pts with obstruction have normal studies
Radiography? n Shunt Survey [XR skull, Chest , KUB]: n n n CT: n n Sensitivity 20% LR –ve 0. 82 83% sens LR –ve 0. 21 Combined : 88 sens BUT! n 1 in 8 pts with obstruction have normal studies
 Diagnostics n Shunt study: n n n Test of choice Usually NSx has to order Tapping the shunt: n n n Easy to do / therapeutic Can send CSF [Can measure ICP]
Diagnostics n Shunt study: n n n Test of choice Usually NSx has to order Tapping the shunt: n n n Easy to do / therapeutic Can send CSF [Can measure ICP]
 Tapping the Shunt n n Sterile Prep 25 gge Butterfly Tubing/syringe Take off 20 cc at a time
Tapping the Shunt n n Sterile Prep 25 gge Butterfly Tubing/syringe Take off 20 cc at a time
 What about the “MI” ? :
What about the “MI” ? :
 Neuro-mediated Cardiac Stress: n n n Electrocardiographic abnormalities well described for SAH TWi, ST ↑ Long QT &c. Originally thought to be benign SAH now known to cause: significant increases in ICP, Increased cardiac output Significant changes in creatine kinase and catecholamines
Neuro-mediated Cardiac Stress: n n n Electrocardiographic abnormalities well described for SAH TWi, ST ↑ Long QT &c. Originally thought to be benign SAH now known to cause: significant increases in ICP, Increased cardiac output Significant changes in creatine kinase and catecholamines
 Furthermore, Pts with SAH and ST ↑have been shown to have impaired contractility “neurogenic stunned myocardium” n One other Report of this related to hydrocephalus from choroid cyst n But now recognise that both psychiatric physiologic stressors can cause an “MI” picture. n
Furthermore, Pts with SAH and ST ↑have been shown to have impaired contractility “neurogenic stunned myocardium” n One other Report of this related to hydrocephalus from choroid cyst n But now recognise that both psychiatric physiologic stressors can cause an “MI” picture. n
 Transient LV dysfunction n Clinically resembles acute myocardial infarction n Characteristics of: transient/reversible LV dysfunction with chest pain EKG changes release of cardiac enzymes hypokinesis of LV on echo Normal coronary arteries
Transient LV dysfunction n Clinically resembles acute myocardial infarction n Characteristics of: transient/reversible LV dysfunction with chest pain EKG changes release of cardiac enzymes hypokinesis of LV on echo Normal coronary arteries
 Clinically: elderly women over 60 years of age n some physical or mental stress precedes the onset of the symptom n Most common presenting symptom is chest pain or dyspnea n Often CHF from decreased left ventricular systolic function n
Clinically: elderly women over 60 years of age n some physical or mental stress precedes the onset of the symptom n Most common presenting symptom is chest pain or dyspnea n Often CHF from decreased left ventricular systolic function n
 Diagnostics: EKG findings classically initial ST elevation n ST depression n Deep symetric T wave inversion n Abnormal QT n Small or moderate elevation of cardiac enzymes (large elevations unusual) n
Diagnostics: EKG findings classically initial ST elevation n ST depression n Deep symetric T wave inversion n Abnormal QT n Small or moderate elevation of cardiac enzymes (large elevations unusual) n
 n Pneumothorax, resp distress,") Etiology/Associated Events: Emotional stress (death of loved one, panic d/o) n Pneumothorax, resp distress, n subarachnoid haemorrhage n Trauma n Phaeochromocytoma n Guillain-Barré syndrome n
Etiology/Associated Events: Emotional stress (death of loved one, panic d/o) n Pneumothorax, resp distress, n subarachnoid haemorrhage n Trauma n Phaeochromocytoma n Guillain-Barré syndrome n
 Pathophysiology: Animal/perfusion models support idea that it is likely the result of catecholamine surge n involves microvascular perfusion Ab. N n In some it involves coronary artery spasm n
Pathophysiology: Animal/perfusion models support idea that it is likely the result of catecholamine surge n involves microvascular perfusion Ab. N n In some it involves coronary artery spasm n
 Pt C. B: Psych Hx n Female, Over 50 n Chest pain and dyspnea n Echo that had apical hypokinesis n ST↑ that progressed to deep TWi and ↑QT n Normal Cath n
Pt C. B: Psych Hx n Female, Over 50 n Chest pain and dyspnea n Echo that had apical hypokinesis n ST↑ that progressed to deep TWi and ↑QT n Normal Cath n
 Voila!
Voila!
 Questions?
Questions?
 References: 1. Physical examination of Patients With cerebrospinal Fluid Shunts: Is There Useful Information in Pumping the Shunt? Joseph H. Piatt Pediatrics 1992; 89(3): 470 -473. 2. Pitfalls in the diagnosis of ventricular shunt dysfunction: radiology reports and ventricular size. Iskandar BJ, Mc. Laughlin C, Mapstone TB, Grabb PA Oakes WJ Pediatrics 1998; 101 (6): 1031 -6 3. Evaluation of Hydrocephalus Shunts in the Emergency Room Robert C Dauser Emergency Medicine Clinics of North America 1987; 5 (4): 709 -717
References: 1. Physical examination of Patients With cerebrospinal Fluid Shunts: Is There Useful Information in Pumping the Shunt? Joseph H. Piatt Pediatrics 1992; 89(3): 470 -473. 2. Pitfalls in the diagnosis of ventricular shunt dysfunction: radiology reports and ventricular size. Iskandar BJ, Mc. Laughlin C, Mapstone TB, Grabb PA Oakes WJ Pediatrics 1998; 101 (6): 1031 -6 3. Evaluation of Hydrocephalus Shunts in the Emergency Room Robert C Dauser Emergency Medicine Clinics of North America 1987; 5 (4): 709 -717
 References : 4. Radiographic evaluation for suspected cerebrospinal fluid shunt obstruction. Zorc JJ, Krugman SD, Ogborn J, Benson J. Pediatr Emerg Care. 2002 Oct; 18(5): 337 -40 5. Ventriculoperitoneal shunt block: what are the best predictive clinical indicators? Barnes NP, Jones SJ, Hayward RD, Harkness WJ, Thompson D. Arch Dis Child. 2002 Sep; 87(3): 198 -201. 6. Akashi et al. The clinical features of takotsubo cardiomyopathy. Q J Med. 2003: 96: 563 -573
References : 4. Radiographic evaluation for suspected cerebrospinal fluid shunt obstruction. Zorc JJ, Krugman SD, Ogborn J, Benson J. Pediatr Emerg Care. 2002 Oct; 18(5): 337 -40 5. Ventriculoperitoneal shunt block: what are the best predictive clinical indicators? Barnes NP, Jones SJ, Hayward RD, Harkness WJ, Thompson D. Arch Dis Child. 2002 Sep; 87(3): 198 -201. 6. Akashi et al. The clinical features of takotsubo cardiomyopathy. Q J Med. 2003: 96: 563 -573
 7. Characterization of the cardiac effects of acute subarachnoid hemorrhage in dogs. Elrifai AM, Bailes JE, Shih SR, Dianzumba S, Brillman J. Stroke. 1996 Apr; 27(4): 737 -41 8. Left ventricular wall motion abnormalities in patients with subarachnoid hemorrhage: neurogenic stunned myocardium. Kono T, Morita H, Kuroiwa T, Onaka H, Takatsuka H, Fujiwara A. J Am Coll Cardiol. 1994 Sep; 24(3): 636 -40. 9. Myocardial injury and left ventricular performance after subarachnoid hemorrhage. Mayer SA, Lin J, Homma S, Solomon RA, Lennihan L, Sherman D, Fink ME, Beckford A, Klebanoff LM. Stroke. 1999 Apr; 30(4): 780 -6.
7. Characterization of the cardiac effects of acute subarachnoid hemorrhage in dogs. Elrifai AM, Bailes JE, Shih SR, Dianzumba S, Brillman J. Stroke. 1996 Apr; 27(4): 737 -41 8. Left ventricular wall motion abnormalities in patients with subarachnoid hemorrhage: neurogenic stunned myocardium. Kono T, Morita H, Kuroiwa T, Onaka H, Takatsuka H, Fujiwara A. J Am Coll Cardiol. 1994 Sep; 24(3): 636 -40. 9. Myocardial injury and left ventricular performance after subarachnoid hemorrhage. Mayer SA, Lin J, Homma S, Solomon RA, Lennihan L, Sherman D, Fink ME, Beckford A, Klebanoff LM. Stroke. 1999 Apr; 30(4): 780 -6.
 Roberts: Clinical Procedures in Emergency Medicine, 4 th ed. , Copyright © 2004 Garton HJL and Piatt JH Hydrocephalus. Pediatr Clin N Am 51 (2004) 305 -325
Roberts: Clinical Procedures in Emergency Medicine, 4 th ed. , Copyright © 2004 Garton HJL and Piatt JH Hydrocephalus. Pediatr Clin N Am 51 (2004) 305 -325