7b5053f5cd1bed9d0d19cb83a7146629.ppt
- Количество слайдов: 57



Integrative Approach to Low Back Pain Wendy Kohatsu, MD Director, Integrative Medicine Fellowship Santa Rosa Family Medicine Residency Program Sept 2011

Goals of this talk: • Review key history elements • Learn how to do better hands-on back exam • Focus on practical & effective lifestyle therapies • Not ‘overmedicalize” LBP via diagnostic tests, drug therapies, surgical interventions. • Later: myriad of mindbody therapies • Talk about something other than food for a change….

Low back pain • 70 -84% of the population affected at some point in their lives • 14 -50% of adults have LBP each year • Cost of > $100 billion/ year • Quality of life impact of acute LBP – 60% unable to perform some daily activity – 72% gave up exercising – 46% gave up sex Spine 12: 264, 1987 Amer Acad Ortho Surg, 2006 Ann Rheum Dis 57: 13, 1998

Posture

Patient case #1: 52 yo female, cc: “sciatica” bilateral numbness hip to knees, since 1999. h/o prior LBP. • 30 years ago fell down flight of stairs at Fisherman’s wharf, landing on tailbone. • Currently works part-time at family business. • On 800 mg ibuprofen. Took friend’s percocet. Flexeril does “nothing”.

Patient case #2 • 86 yo Vietnamese male, DM 2, reluctant to see MD. • Ambulates with 4 -prong cane • c/o LBP, radiating to back of legs, doesn’t like to take medicine, uses analgesic balm • ROS: urinary retention, feels more tired, recent weight loss.

History-taking

History-taking • • • Onset/first episode? Occupational risk Co-morbidities Activity & exercise level Psychosocial stress/ diagnoses Other?

3 main questions for LBP: 1. Is systemic disease causing the pain? 2. Is there social or psychological distress that may amplify or prolong the pain? 3. Is there neurologic compromise that may require surgical evaluation? Deyo & Weinstein NEJM 344: 363, 2001

“Red flags” ACR Criteria - Low Back Pain, 2005

“Red flags” • Hx of trauma • Focal neurologic signs - incontinence, weakness, numbness • Hx of cancer • Age of first onset after 50 years • Hx of IVDA • Osteoporosis • Signs of systemic disease - fever, wt loss, lymphadenopathy ACR Criteria - Low Back Pain, 2005

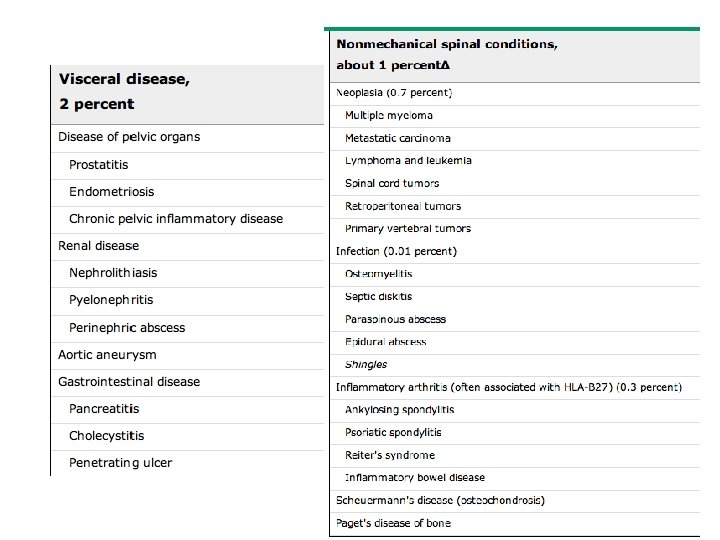
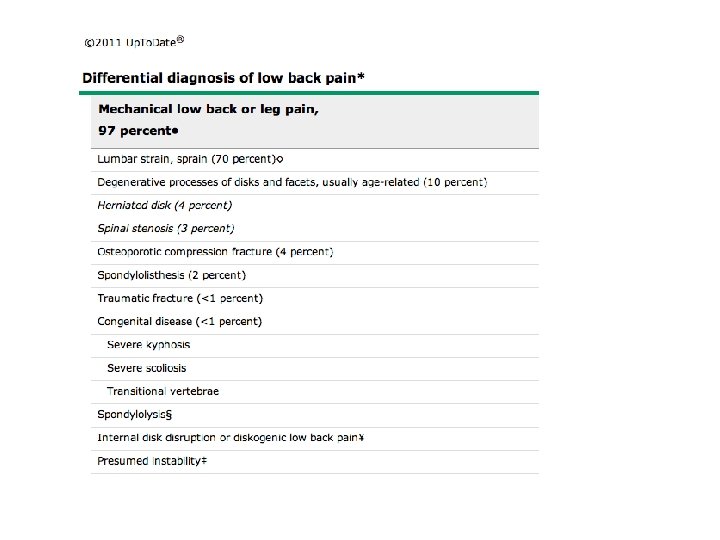
Perspective • Among all primary care patients with LBP, < 5% will have serious systemic pathology. • 97% will have LBP w/o radiculopathy – 60% Simple back pain – 37% Complex back pain w/o radiculopathy • 3% will have LBP with radiculopathy – Sx of radiculopathy – 1% with acute neuro sx – loss of bladder fxn, saddle anesthesia, motor weakness N Engl J Med. 2001; 344(5): 363 Up To Date –June 2011
: 478. JAMA. 2010;")
To image or not to image… Ann Intern Med. 2007; 147(7): 478. JAMA. 2010; 303(13): 1295. • MRI evaluation to provide reassurance for chronic LBP does NOT lead to better prognosis. • Psychosocial variables are stronger predictors of longterm disability than anatomic findings found on imaging studies. • Radicular sx > 4 -6 weeks, severe enough to consider surgery.

So, let’s examine our patients…

2 1/2 -minute focused neuro exam Position Test/feature Findings All Observe Behavior Standing • Posture & gait • Toe / heel walking • Asymmetry • Straight leg raise • Neurologic testing • Posture habits • L 5 or S 1 deficiency* • Scoliosis • Leg length • Straight leg raise • Fabere’s sign • Mech contribution • Palpation • Hip Extension 5 -20 • Prone prop • Muscle dysfxn • L 2 -4 radiculopathy • Facet jt dysfxn Sitting Supine Prone • Radicular pain • Sensory defect • Radicular pain • Hip involvement Biewen PC Postgrad Med 106: 102, 1999
* • *Except Natasha, Trang,")
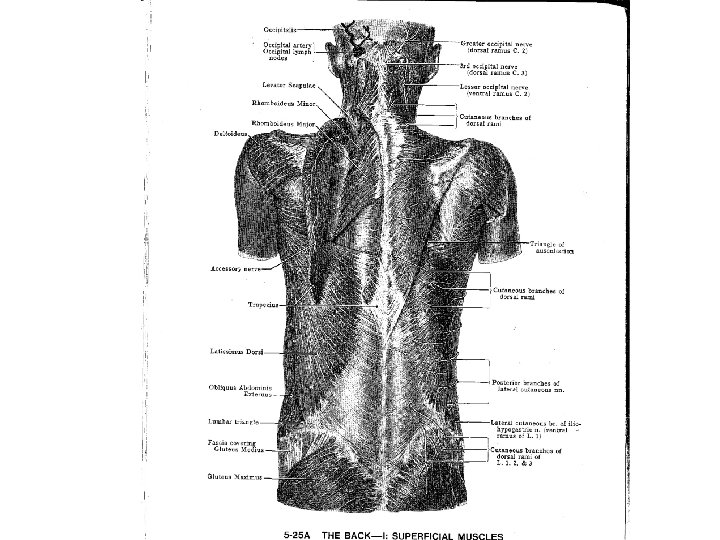
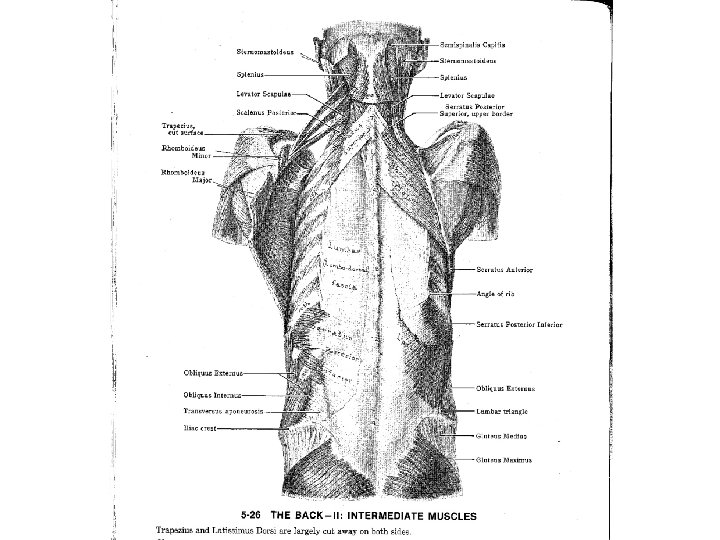
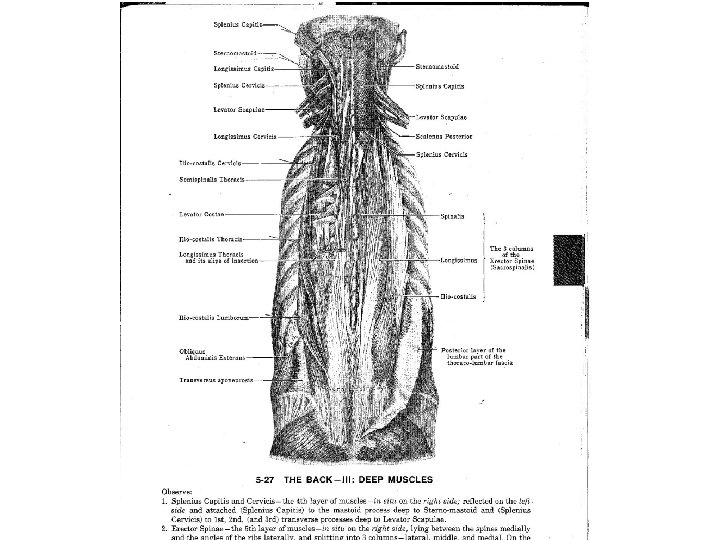
EXAM! - Anatomy Review (what med school never taught you…)* • *Except Natasha, Trang, Sarah W & Hana C. • OMT basic evaluation • 3 layer muscle palpation • Skeletal survey -- L-spine, pelvic girdle, lower extremities (joint above/below) • Common culprits: Erector spinae spasm, Lumbar rotation, SI joint dysfxn, psoas, piriformis spasm, muscle imbalance, myofascial syndrome!

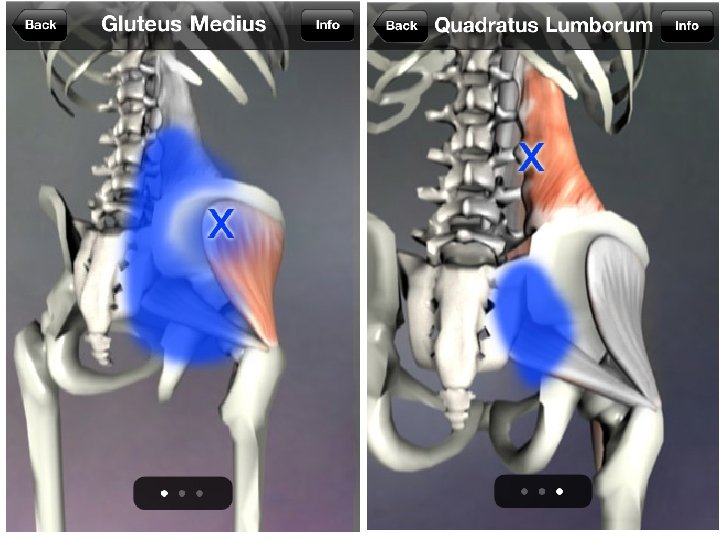
OMT Common Culprits: • • Erector spinae spasm Lumbar rotation SI joint dysfxn Psoas Piriformis spasm Muscle imbalance Myofascial syndrome!

Psoas located deep in abdomen, but major hip flexor. Radiates to: - Lumbar region - Front of hip

The “Dirty Half-Dozen” of Refractory LBP OMT diagnosis Trunk-thigh imbalance Lumbar dysfxn Pubic dysfxn Short leg/pelvic tilt Posterior sacral base Innominate shear Frequency 100% 88% 76% 65% 60% 24% n = 183 ‘untreatable’ pts with refractory LBP 75% restored to normal activity after OMT* Phys Med Rehab Clin NA 7: 773, 1996

Patient #1 - Exam • 52 yo woman with sciatica • Exam: Wt 151, BMI 25. 5, anxious • Neuro: 4+/5 left hip flexion, knee extension. Preserved gait and balance walking in hallway. • MSK: level iliac crest heights, ++ 4 cm left posterior hip rotation, ++ right sacral torsion, L > R SI join tenderness, LEFT glut max, min + piriformis spasm. • Imaging: NONE.

Patient # 2 - Exam 86 yo Vietnamese male with LBP • Very stoic, pleasant, NAD • Wt 111 (down from 129 lbs 4 mos prior) • Thin frame, + increased thoracic kyphosis, tight lumbar paraspinal muscles. • Rectal: Enlarged prostate.

Posture

What next?

Principle Based Treatment Pyramid en re m so on ur ce s vir en t relationship

Principle Based Treatment Pyramid resources environment relationship

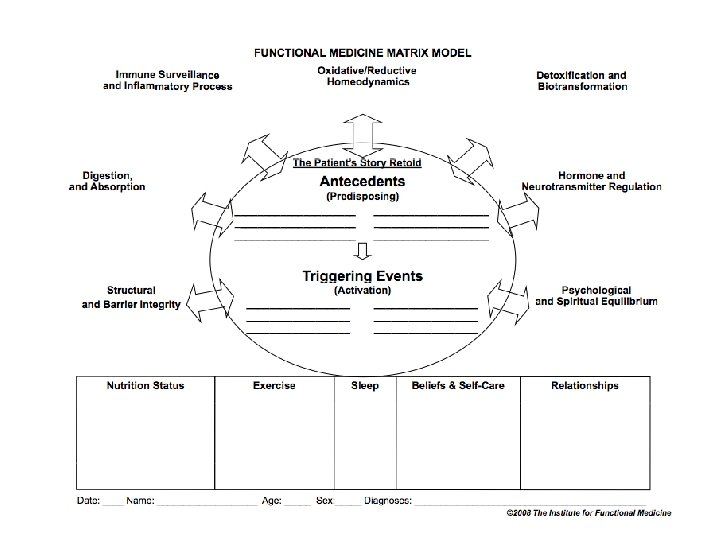
Treatment Options • “Internal Environment” • Lifestyle • CAM therapies • Drugs

Treatment Options • “Internal Environment” – Pain is a signal for change – John Sarno, MD ~ (TMS)Tension Myositis Syndrome • Lifestyle • CAM therapies • Drugs

Treatment Options • “Internal Environment” • Lifestyle • CAM therapies • Drugs – NSAIDs – Analgesics – Muscle relaxants

NSAIDs • For acute LBP – Ibuprofen 400 -600 mg up to qid – Naproxen 220 -500 mg bid • Side effect and risks limit use Cochrane Database NSAIDS for LBP, 2008 ACP and Amer Pain Soc Guidelines 2007

Analgesics • Acetaminophen – Up to 2. 6 grams/d as first line therapy – Side efx - hepatoxicity • Opioids – Surprisingly little data • One meta-analysis = not significantly reduce chronic low back pain – Inadequate data re: functional improvement correlating to pain relief – Reports of opioid abuse ~ 30 -45% in LBP CMAJ 174: 1589, 2006 Ann Intern Med 146: 166, 2007 Cochrane Database Syst Rev -Opioids for Chronic LBP, 2008 FDA guidelines June 2009

Muscle relaxants • “Insufficient evidence” for chronic use • CNS side effects - sedation • Carisoprodol metabolized --> meprobamate, abuse and addiction potential • Limit to short-term use only in conjunction with analgesics van. Tulder et al. Spine 28: 1978; 2003

Drug-Nutrient Interactions • NSAIDS deplete… • Folic Acid Synthesis of folic acid is competitively - inhibited by NSAIDs -Rx: eat your leafy greens! (“foliage”)

Treatment Options • “Internal Environment” • Lifestyle • CAM therapies – Acupuncture – Massage – Chiropractic or osteopathic manipulation • Drugs

Acupuncture for LBP • Like massage, data show acupuncture is moderately more effective than no treatment • Short-term outcomes > long-term • More likely to benefit those who expect more out of acupuncture. Cochrane Database Syst Rev - Acu for LBP, 2005 Spine 26: 1418, 2001

Massage • Appears to be better for acute vs chronic back pain • Studies inconclusive due to varying styles, practitioner skill, duration of treatment

Manipulation • “Moderately superior” to sham Rx, null therapies • But equal to analgesics, exercises, back school • Mixed bag of techniques studied --Most studies on HVLA techniques used in chiropratic Rx Ann Intern Med (meta-analysis)138: 871 2003 Ann Intern Med 138: 989, 2003

Treatment Options • “Internal Environment” • Lifestyle – Exercise • Stretching, strengthening, yoga – Stress management • CAM therapies • Drugs

Low Back Pain - Exercise Rx • 2005 Systematic Review – 43 trials of 72 exercise treatments – Improvement seen esp. with • High-dose exercise programs • Interventions that included conventional care • Stretching and strengthening demonstrated the largest improvements. (vs passive treatments) Ann Intern Med 142(9): 776 -85, 2005

Low back pain - Exercise Rx • BMJ study 1995 with “moderately disabled” pts. – 81 chronic LBP patients, referred from ortho • Control – home exercises + ref’d to back school • Intervention – above + 8 exercise classes/4 wks – Two hour sessions • Warm up, stretching • 15 systematic progressive exercises • Lite aerobic activity and stretching • Signif. improvements in pain reduction, self-efficacy, and walking distance noted at 4 weeks, and 6 month f/u Frost, H, et al. 1995 BMJ 310(6973): 151 -4.

Low back pain Exercise Rx • Study by Carpenter & Nelson, 60 pts considering neurosurgery – 10 week back-strengthening program • Progressive resistance exercise • Isolated lumbar extensions (with pelvis neutral) • One set of 8 -15 reps to volitional fatigue 1 x/week – 57/60 pain-free, no longer needed surgery! Med Sci Sports Exerc 1999 31(1): 18 -24.

Best outcomes for exercise therapy Best outcomes achieved when these 4 elements included: • Individualized regimens • Stretching • Strengthening • Supervision Hayden, Van Tulder et al. Ann Int Med 142: 776, 2005

Home exercise Rx • Tennis ball* -- myofascial and erector spinae column • Abdominal strengthening • Quad strengthening • Spinal twist • Piriformis stretching • Hamstring stretching

Pelvic Clock Technique • Created and researched by Phil Greenman, DO • No prior training required • Dx and Rx at same time • Patient can do at home

Take home points • Ask the 3 questions - are systemic dx, neurol red flags, or psychosocial fx present? • DO THE EXAM! – Focused neuro exam – Musculoskel exam – Be judicious when ordering imaging • Rx: Improve function, not just blunt pain • Teach exercise therapies, can tailor to individual patient

Strength training • Why? – Muscle strength declines rapidly after 50 in sedentary people. REVERSIBLE! – Increase bone density – Improves strength & ability to perform aerobic exercise. – INCREASE BASAL METABOLIC RATE (BMR) by increasing lean body mass. Life, J. CAM Secrets (2002)

“Core Four” Weight Training Program – Hewitt 2002
7b5053f5cd1bed9d0d19cb83a7146629.ppt