14df11ecfe868eeb7d164afff0e1ef10.ppt
- Количество слайдов: 42



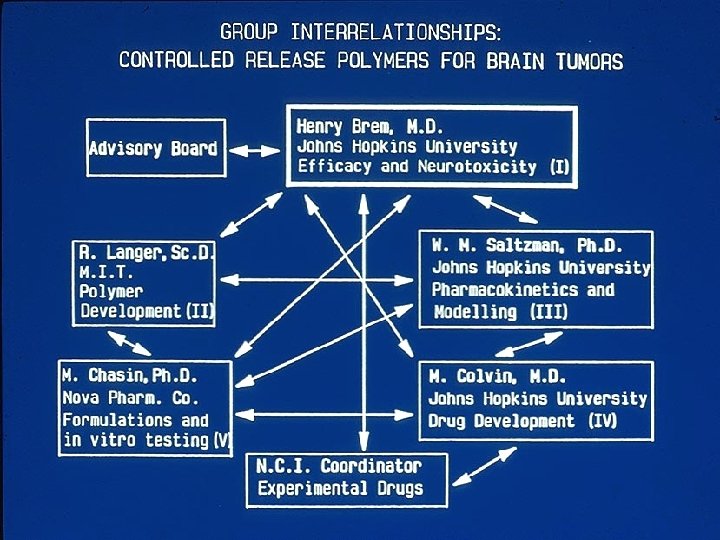
INNOVATION AND ENTREPRENEURSHIP NEW BRAIN TUMOR TREATMENTS Henry Brem, M. D. Harvey Cushing Professor and Chairman Department of Neurosurgery Johns Hopkins University NATIONAL SCIENCE FOUNDATION I/UCRC Biennial Meeting Hyatt Regency Crystal City, Arlington, VA JULY 27, 2017

Disclosures • Research Funding from NIH, Johns Hopkins University, Arbor Pharmaceuticals, Bristol Myers Squib, and Accurexa* and philanthropy • Consultant for Asclepi. X Therapeutics, Celsion. EGEN, Perosphere Inc, Stem. Gen, Accelerating Combination Therapies*, Camden Partners, Like. Minds, Inc, Acuity Bio Corp (*includes equity)

BRAIN TUMORS • OPPORTUNITIES VS OBSTACLES

BRAIN TUMORS • In 1984 – many systemic treatments had been tried with no benefit. • The FDA had not approved any new therapy in over 20 years. • NOR HAD THE MEDIAN SURVIVAL!

Percent of Survivors Malignant Astrocytoma: Survival Months
 12 10 9. 25 10 8 6 4")
Glioblastoma: Treatment Outcome Median Survival (Months) 12 10 9. 25 10 8 6 4 4 2 0 Surgery Only Surgery + Radiotherapy + Chemotherapy Mc. Donald JD, Rosenblum ML: In: Rengachary SS, Wilkins RH, eds. Principles of Neurosurgery. St Louis, MO: Mosby-Wolfe; 1994: chap 26.

BRAIN TUMOR OPPORTUNITY • THE QUESTION, IN 1984, WAS COULD ANYTHING, ANYTHING AT ALL, BE DONE TO CHANGE THE DISMAL OUTCOMES FOR GLIOBLASTOMA! • NOT A SINGLE DRUG HAD SHOWN STATISTICALLY SIGNFICANT IMPROVEMENT, NOR HAD THE MEDIAN SURVIVAL OF 9 MONTHS CHANGED

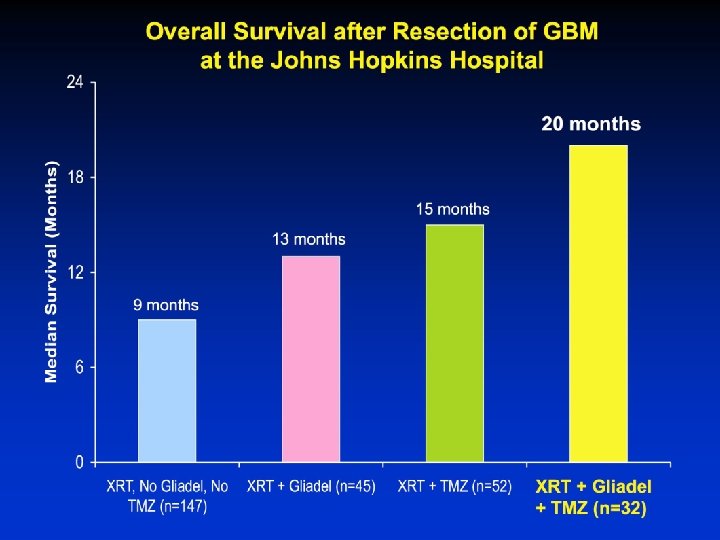
BRAIN TUMOR OBSTACLES IN 2017, WE HAVE GLIADEL, TEMODAR, AVASTIN DRAMATIC IMPROVEMENTS IN IMAGING AND SURGERY, ICU & MEDICAL CARE GLIASITE, NOVOCURE MORE THEN DOUBLING OF MEDIAN SURVIVAL FOR GBM (9 MONTHS TO 20 MONTHS!) AND MORE LONG TERM SURVIVORS AND AN EVER GROWING PIPELINE OF NEW THERAPIES!

OPPORTUNITY VS BARRIERS in 2017 • THE QUESTION IN 2017, IS GIVEN THE EXTRAORDINARY PIPELINE OF NEW APPROACHES IN THE LABORATORY AND IN CLINICAL TRIALS…. . • HOW DO WE OVERCOME THE BARRIERS THAT PREVENT THESE NOVEL TREATMENTS FROM BENEFITING OUR PATIENTS? ? ?

BARRIERS TO NEW TREATMENTS • IDEAS – LABORATORY EXPLORATION & VALIDATION – DELIVERY TO TARGET – FUNDING! – CLINICAL TRIALS: SAFETY, EFFICACY – FDA APPROVAL (INCREDIBLE FOR DRUGS, EASIER FOR DEVICES) – WHO PAYS FOR NEW TREATMENT? (CMS, Insurance, Patient) – MARKETING INVESTMENT – CLINICAL JUDGEMENTS AND BIASES

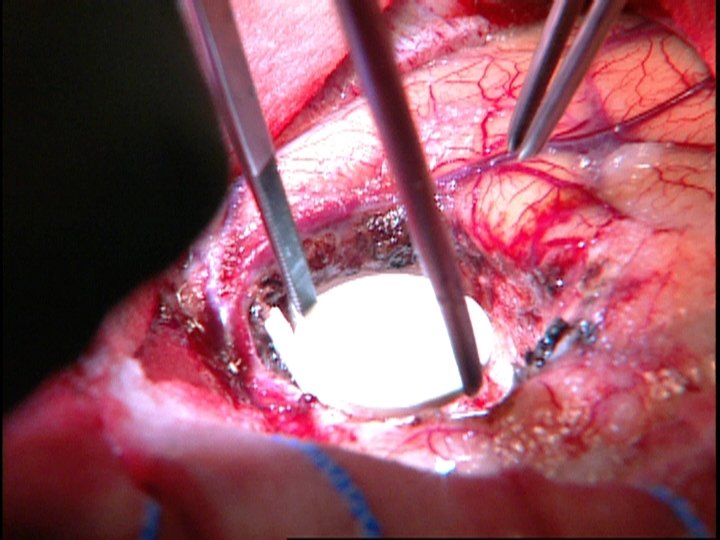
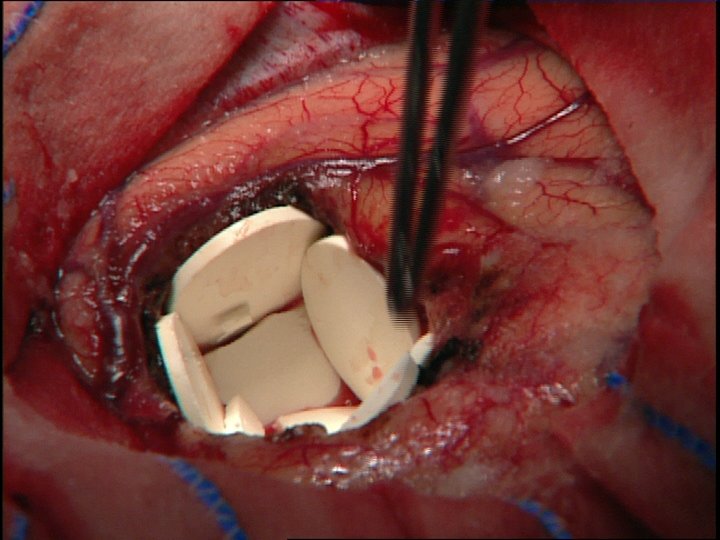
Problem: Clinical effectiveness of new cancer therapies Hypothesis: Better delivery of agents to target sites would improve outcome Solution: Targeted controlled delivery (polymers)

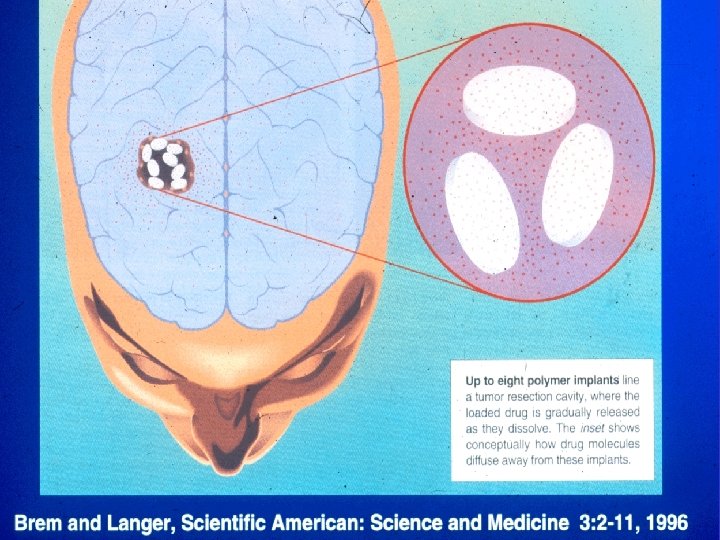
Robert Langer and colleagues described use of polyanhydrides Polifeprosan

Commercial finding: this polymer was useless for clothing because it dissolved when it rained


Preclinical Studies • Safety - Implantation in cornea and brain - Rats, Rabbits, and Monkeys • Drug Distribution - Autoradiography: rats, rabbits, monkeys • Efficacy - Rodent models

1. 45 cm/disc x 8 = 11. 6 cm diameter ~3 mm diameter Human Monkey Dog Rat Rabbit

This approach will not work because: • The polymer drug system would be toxic (1987) • Drugs would not diffuse far enough (1989) • Models do not reflect clinical reality (1991) • BCNU is a very poor drug (1993) • FDA approval would be impossible (1995) • How will it be paid for? (1997) • Which patients will maximally benefit? (1999) • Would the FDA broaden the indications? (2003) • Precludes phase I studies (2005) • Need better targeted drugs! & combinations ((2007. . ) • Need more sophisticated delivery approaches (Microchips, Ultrasound and nano-technology) (2017)

GLIADEL DEVELOPMENT 1985 – 2017 • • • Nova Scios Nova Guilford Rhone Poulenc Rhorer Aventis Guilford MGI PHARMA Eisai Co, LTD Arbor Pharmaceuticals (Dec 19, 2012) • Bristol Myers Squibb + Arbor

2017 21 YEARS AFTER FDA APPROVAL GLIADEL IS USED WIDELY THROUGHOUT THE WORLD 30 COUNTRIES and over 1500 ACADEMIC & COMMUNITY MEDICAL CENTERS
 Glioblastoma: Treatment Outcome 12 10 9. 25 10 8 6 4")
Median Survival (Months) Glioblastoma: Treatment Outcome 12 10 9. 25 10 8 6 4 4 2 0 Surgery Only Surgery + Radiotherapy + Chemotherapy Mc. Donald JD, Rosenblum ML: In: Rengachary SS, Wilkins RH, eds. Principles of Neurosurgery. St Louis, MO: Mosby-Wolfe; 1994: chap 26.
 0")
100 % Overall survival 80 60 40 20 62 publications (60 clinical trials) 0 4, 898 patients; p = 0. 043 1 2 Years Newly diagnosed high grade glioma Chowdhary et al, J. Neurooncol. , 2015

Drug Eluting Stents

Ventriculoperitoneal shunt system Sciubba et al. , 2005

Antibiotic-impregnated catheters for Hydrocephalus • Ventricular shunt infection: • High patient morbidity as well as cost • Antibiotic-impregnated catheters • Prevention of bacterial colonization • Specifically targets grampositive bacteria • 12% to 1. 4% Sciubba et al. , 2005 J Neurosurgery 103: 131 -6

IMMUNOTHERAPY • CHECKPOINT INHIBITORS -IS CHEMOTHERAPY BENEFICIAL OR DETRIMENTAL? ?

Science Translational Medicine, Dec 21, 2016

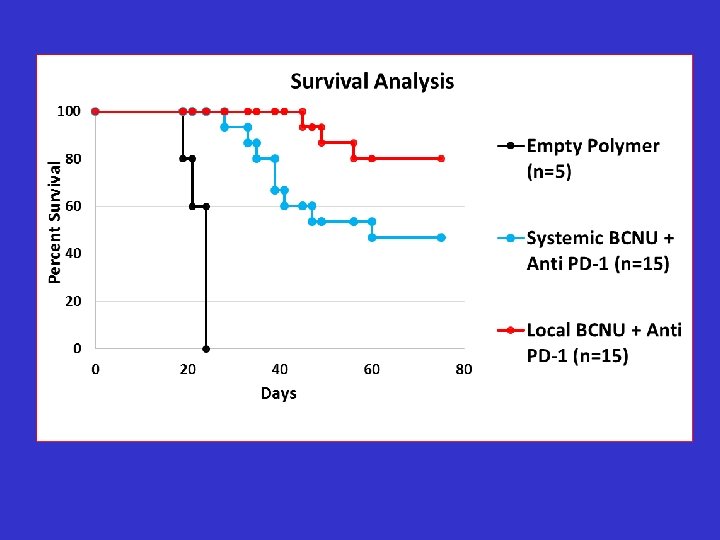
Question Is immunotherapy affected by local vs systemic concentrations of chemo?

Question IS IMMUNOLOGIC MEMORY AFFECTED BY LOCAL VS SYSTEMIC CHEMOTHERAPY?

Re-challenged mice Anti-PD-1 i. p. BCNU +anti-PD-1 Day 7 Day 17 Mathios et al. Sci Transl Med Dec 21, 2016 LC+anti-PD-1

IMMUNOLOGIC MEMORY IS LOST WITH PD-1 + SYSTEMIC CHEMOTHERAPY BUT NOT WITH PD-1 + LOCAL CHEMOTHERAPY

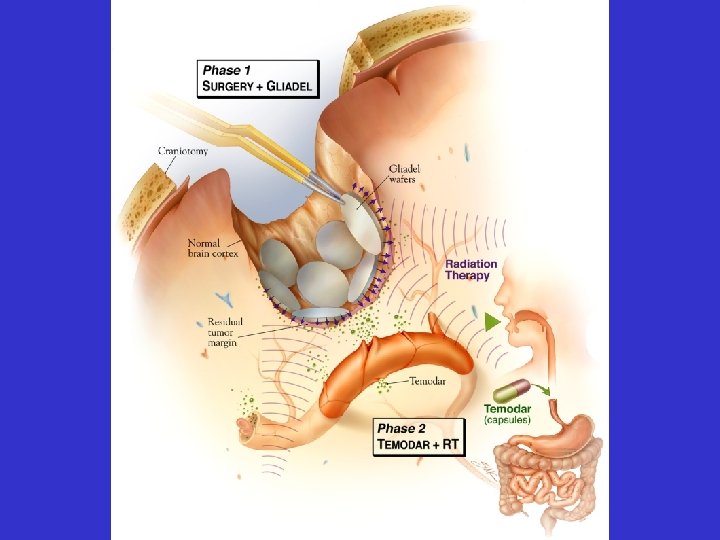
A Randomized Safety and Efficacy Study of Gliadel® in Combination with Standard Radiation Therapy with or without Anti-PD-1 (nivolumab) in Newly Diagnosed Adult Subjects with MGMT (tumor 06 -methylguanine DNA methyltransferase) Unmethylated Glioblastoma Anti-PD-1 + Standard RT Newly Diagnosed Unmethylated MGMT With Gliadel Anti-PD-1 + Standard RT + TMZ FUNDED BY ARBOR PHARMACEUTICALS AND BRISTOL MEYER SQUIBB

Brain Tumor Therapy • These improvements are only the beginning and there is much more now in the “pipeline” • However, none of this would have been possible if not for reaching across borders between specialties, academic centers, industry, NIH, FDA, Patient Advocate Groups, Congress and CMS as well as international regulatory agencies!

Brain Tumor Therapy • The opportunities have never been greater!!!! • but their will always be barriers!!!!

The Treatment of Brain Tumor “Scientific accuracy must supplant guesswork in diagnosis and directing the treatment” W. E. Dandy JAMA 77: 1858 -1859 (1921)
14df11ecfe868eeb7d164afff0e1ef10.ppt