

29933dcbb7af7f3d84a73860603db926.ppt
- Количество слайдов: 78
 New Trends in Management Vahab") Increasing Diagnosis of Micro-Papillary Thyroid Cancer (<1 cm ) New Trends in Management Vahab Fatourechi MD Mayo Clinic Tehran EMRI 2015
Increasing Diagnosis of Micro-Papillary Thyroid Cancer (<1 cm ) New Trends in Management Vahab Fatourechi MD Mayo Clinic Tehran EMRI 2015
 Learning Objectives • Recognize different clinical presentations of micropapillary cancer • Be familiar with trends in less aggressive management of incidental occult papillary cancer • Short reference to 2015 ATA Guidelines
Learning Objectives • Recognize different clinical presentations of micropapillary cancer • Be familiar with trends in less aggressive management of incidental occult papillary cancer • Short reference to 2015 ATA Guidelines
 NOT ALL THYROID CANCERS ARE EQUAL THYROID CANCER FREQUENCY MORTALITY Papillary 85% 1 -2% at 20 years Follicular 11% 10 -20% at 10 years Medullary 3% 25 -50% at 10 years Anaplastic 1% 90% at 5 years • 1 patient in 100 with PTC will die due thyroid cancer at 20 years • 1 patient in 1000 with low-risk PTC will die at 20 years. Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html
NOT ALL THYROID CANCERS ARE EQUAL THYROID CANCER FREQUENCY MORTALITY Papillary 85% 1 -2% at 20 years Follicular 11% 10 -20% at 10 years Medullary 3% 25 -50% at 10 years Anaplastic 1% 90% at 5 years • 1 patient in 100 with PTC will die due thyroid cancer at 20 years • 1 patient in 1000 with low-risk PTC will die at 20 years. Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html
 Papillary Cancer Cell Types Associated with Aggressive Behavior • • • Columnar cell PTC Insular cell PTC Tall cell PTC Trabecular PTC Higher grades of PTC : Grade 2 -4 (majority are grade 1) Comment : Most of these present clinically and rarely micro-papillary
Papillary Cancer Cell Types Associated with Aggressive Behavior • • • Columnar cell PTC Insular cell PTC Tall cell PTC Trabecular PTC Higher grades of PTC : Grade 2 -4 (majority are grade 1) Comment : Most of these present clinically and rarely micro-papillary
 RELATIVE SURVIVAL RATES AT 5 YEARS Thyroid 97. 5% Low Risk 99. 9% 1 patient in 1000 affected with low-risk thyroid cancer and treated will die due to thyroid cancer Surveillace Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html Slow progression or regression
RELATIVE SURVIVAL RATES AT 5 YEARS Thyroid 97. 5% Low Risk 99. 9% 1 patient in 1000 affected with low-risk thyroid cancer and treated will die due to thyroid cancer Surveillace Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html Slow progression or regression
 Cause-Specific Mortality Rates in FCDC Mayo Data 90") Dying of thyroid carcinoma (cumulative %) Cause-Specific Mortality Rates in FCDC Mayo Data 90 ATC FTC HCC PTC Years after initial treatment
Dying of thyroid carcinoma (cumulative %) Cause-Specific Mortality Rates in FCDC Mayo Data 90 ATC FTC HCC PTC Years after initial treatment
 PTC Survival by TNM Stage Mayo Data n=2, 284") Surviving papillary thyroid carcinoma (%) PTC Survival by TNM Stage Mayo Data n=2, 284 1940 -97 P=0. 0001 TNM stage I 1, 360 II 493 III 399 IV 32 Years after initial treatment
Surviving papillary thyroid carcinoma (%) PTC Survival by TNM Stage Mayo Data n=2, 284 1940 -97 P=0. 0001 TNM stage I 1, 360 II 493 III 399 IV 32 Years after initial treatment
 •") No Change in Mortality over 6 Decades in PTC (Mayo Clinic Data) • • • 2444 cases 1940 -1999 No change in cause specific mortality No change in tumor recurrence rate Remnant RA ablation did not change outcome For low risk (MACIS <6) CSM 1% and recurrence 15% Hay ID, World J Surg 2002: 26; 879 Endo Pract 2007 : 13 521
No Change in Mortality over 6 Decades in PTC (Mayo Clinic Data) • • • 2444 cases 1940 -1999 No change in cause specific mortality No change in tumor recurrence rate Remnant RA ablation did not change outcome For low risk (MACIS <6) CSM 1% and recurrence 15% Hay ID, World J Surg 2002: 26; 879 Endo Pract 2007 : 13 521
 Thyroid Carcinoma: 1992 - 2014 Estimates • Incidence increased from 20, 000 to 62, 800 • 1992 5/100, 000 • 2014 15 /100, 000 • Almost all of increase is papillary thyroid cancer: over 95% of all thyroid cancers • Deaths n=1850 , Not changed Davis L, eta l JAMA Otolaryngol Head Neck Surg 2014; 140: 317
Thyroid Carcinoma: 1992 - 2014 Estimates • Incidence increased from 20, 000 to 62, 800 • 1992 5/100, 000 • 2014 15 /100, 000 • Almost all of increase is papillary thyroid cancer: over 95% of all thyroid cancers • Deaths n=1850 , Not changed Davis L, eta l JAMA Otolaryngol Head Neck Surg 2014; 140: 317
 Increasing Incidence of Thyroid Cancer Worldwide • .
Increasing Incidence of Thyroid Cancer Worldwide • .
 • • Comparesd 1990 -1999") Rising Thyroid Cancer Incidence Olmsted County Minnesota (Mayo data) • • Comparesd 1990 -1999 to 2000 -2012 7. 1 /100000 Increased rate to 13. 7 53% asymptomatic incidental finding Neck imaging 36%, incidental for thyroid benign disease Surgery 26%, found on routine exam 20%, investigation for unrelated symptoms 12% • Exclusion of incidental brings rate to 6. 3% • Brio JP et. al, Abstract ATA meeting Oct 2014
Rising Thyroid Cancer Incidence Olmsted County Minnesota (Mayo data) • • Comparesd 1990 -1999 to 2000 -2012 7. 1 /100000 Increased rate to 13. 7 53% asymptomatic incidental finding Neck imaging 36%, incidental for thyroid benign disease Surgery 26%, found on routine exam 20%, investigation for unrelated symptoms 12% • Exclusion of incidental brings rate to 6. 3% • Brio JP et. al, Abstract ATA meeting Oct 2014
 Detection of Reservoir Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html
Detection of Reservoir Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html
 Detection of Reservoir Rate per 100 000 US-guided aspiration of thyroid nodules Increased in CT/MRI use Widespread use of thyroid ultrasound Fine-needle aspiration for thyroid nodule Brito JP. BMJ 2013; 347: f 4706
Detection of Reservoir Rate per 100 000 US-guided aspiration of thyroid nodules Increased in CT/MRI use Widespread use of thyroid ultrasound Fine-needle aspiration for thyroid nodule Brito JP. BMJ 2013; 347: f 4706
 South Korean Experience in n Routine Thyroid Cancer Screening • In 1999 In south korea national cancer screening program started thyroid was not a part but most provided added US of neck for small fee • Diagnosis of thyroid cancer increased 15 fold • 40, 000 diagnosed in 2011, death rate annually 300 -400 • Death from thyroid cancer did not change H. S Ahn et al NEJM Nov 2014 : 731: 1765
South Korean Experience in n Routine Thyroid Cancer Screening • In 1999 In south korea national cancer screening program started thyroid was not a part but most provided added US of neck for small fee • Diagnosis of thyroid cancer increased 15 fold • 40, 000 diagnosed in 2011, death rate annually 300 -400 • Death from thyroid cancer did not change H. S Ahn et al NEJM Nov 2014 : 731: 1765
 Thyroid-Cancer Incidence and Related Mortality in South Korea, 1993") Rate (per 100, 000 population) Thyroid-Cancer Incidence and Related Mortality in South Korea, 1993 -2011 Thyroid-cancer incidence Incidence of papillary thyroid cancer Thyroid-cancer mortality Ahn et al: NEJM 371; 19, 2004
Rate (per 100, 000 population) Thyroid-Cancer Incidence and Related Mortality in South Korea, 1993 -2011 Thyroid-cancer incidence Incidence of papillary thyroid cancer Thyroid-cancer mortality Ahn et al: NEJM 371; 19, 2004
 Thyroid Cancer Reservoir l l l Sectioned thyroids from 101 autopsy specimens, 1 -3 mm slices. Found PTC in 36% of glands, no prior history of thyroid disease. Speculated that if sectioned carefully enough, many more would have been found, perhaps all. Harach HR. Cancer 1985; 56: 531 -8.
Thyroid Cancer Reservoir l l l Sectioned thyroids from 101 autopsy specimens, 1 -3 mm slices. Found PTC in 36% of glands, no prior history of thyroid disease. Speculated that if sectioned carefully enough, many more would have been found, perhaps all. Harach HR. Cancer 1985; 56: 531 -8.
 Incidental Thyroid Micro-cancer In Autopsy • • Argentina ; n=100, 13. 6% men , 7. 3% women Spain 5. 3% Bellarus 9. 3% • Greece: 7. 7 % • Sweden: 8. 6% Cancer ; 1989; 64; 1888 Martinez – Tello Cancer 1003; 71; 4022 Fufrmanchuck AW Histopathology, 1993, 4; 319 Mitselou, A , Anticancer research 2002 22; 427
Incidental Thyroid Micro-cancer In Autopsy • • Argentina ; n=100, 13. 6% men , 7. 3% women Spain 5. 3% Bellarus 9. 3% • Greece: 7. 7 % • Sweden: 8. 6% Cancer ; 1989; 64; 1888 Martinez – Tello Cancer 1003; 71; 4022 Fufrmanchuck AW Histopathology, 1993, 4; 319 Mitselou, A , Anticancer research 2002 22; 427
 Incidental Thyroid Micro-cancer In Autopsy • • • Pub Med Search 2011 21 countries, 7897 autopsies English literature 0. 14 % MTC 7. 6% PTC all <0. 5 cm no lymph nodes • Conclusion : This should be considered in epidemiologic studies and screening recommendations Valle LE JCEM 2011 96: 109
Incidental Thyroid Micro-cancer In Autopsy • • • Pub Med Search 2011 21 countries, 7897 autopsies English literature 0. 14 % MTC 7. 6% PTC all <0. 5 cm no lymph nodes • Conclusion : This should be considered in epidemiologic studies and screening recommendations Valle LE JCEM 2011 96: 109
 Incidental Micro cancer in Thyroidectomy for Benign Disease • 15% Siassakos Singapore med J 2008 • 8. 8% Femando , Cylone Med J 2009 • 2. 2 % in GD Anilam. Rev Med Schir Soc Med Nallasi 2008 • • • 12% Bradley DP, Surgery 146: 2009 9. 3% Costamagna G , Surg 2013 5. 7 % Bombil I, S Afr J Surg 2014 26% Ergin AB, Amer J otolaryng, 2014, 16. 7% Fink, Mod path 1996, 9; 816 10%(GD) Karagulle E, Int Surg 2009; 94; 325 Mean 12%
Incidental Micro cancer in Thyroidectomy for Benign Disease • 15% Siassakos Singapore med J 2008 • 8. 8% Femando , Cylone Med J 2009 • 2. 2 % in GD Anilam. Rev Med Schir Soc Med Nallasi 2008 • • • 12% Bradley DP, Surgery 146: 2009 9. 3% Costamagna G , Surg 2013 5. 7 % Bombil I, S Afr J Surg 2014 26% Ergin AB, Amer J otolaryng, 2014, 16. 7% Fink, Mod path 1996, 9; 816 10%(GD) Karagulle E, Int Surg 2009; 94; 325 Mean 12%
 Thyroid Incidental Micro-cancer FDG- PET • • N= 2105 Focal uptake 1. 7% (35) Confirmed PTC 8 Malignancy 3 3% on PET Pos Prichard RS Ir med J , 2011: 104; 177
Thyroid Incidental Micro-cancer FDG- PET • • N= 2105 Focal uptake 1. 7% (35) Confirmed PTC 8 Malignancy 3 3% on PET Pos Prichard RS Ir med J , 2011: 104; 177
 Thyroid Cancer in Ultrasound Screening • • N=1140, Hong Kong No thyroid symptoms routine screening 44% nodules FNA in 258 patients 2. 3% FNA suspicious for malignancy 1. 2% Histologic PTC Conclusion: If routine screening is used 4. 2 million in USA Yuen AP Head and Neck 2011, 33; 453
Thyroid Cancer in Ultrasound Screening • • N=1140, Hong Kong No thyroid symptoms routine screening 44% nodules FNA in 258 patients 2. 3% FNA suspicious for malignancy 1. 2% Histologic PTC Conclusion: If routine screening is used 4. 2 million in USA Yuen AP Head and Neck 2011, 33; 453
 Detection of Reservoir • If we assume only 6% as prevalence of micro PTC: – Predicts 18 million cases in population – SEER database reports only 0. 5 million prevalence of all types and sizes of DTC – We have yet only seen the tip of the iceberg – In current practice, PTC will be the most rapidly growing cancer diagnosis for years to come. Ross and Tuttle. Thyroid 24: 3 -6 2013
Detection of Reservoir • If we assume only 6% as prevalence of micro PTC: – Predicts 18 million cases in population – SEER database reports only 0. 5 million prevalence of all types and sizes of DTC – We have yet only seen the tip of the iceberg – In current practice, PTC will be the most rapidly growing cancer diagnosis for years to come. Ross and Tuttle. Thyroid 24: 3 -6 2013
 Likelihood of Death from Histologic Thyroid Cancer • Estimated death 1780/year • with conservative estimate 7 % of USA population (22) million have micro PTC • Thus likelihood of death from all thyroid cancer is 79 per one million histologic thyroid cancer (0. 0079%) • Almost all mortality is from clinical thyroid cancer not occult. Mortality would be close to zero for occult undiagnosed thyroid cancer
Likelihood of Death from Histologic Thyroid Cancer • Estimated death 1780/year • with conservative estimate 7 % of USA population (22) million have micro PTC • Thus likelihood of death from all thyroid cancer is 79 per one million histologic thyroid cancer (0. 0079%) • Almost all mortality is from clinical thyroid cancer not occult. Mortality would be close to zero for occult undiagnosed thyroid cancer
 Possible Causes of Increasing Incidence • • Radiation Exposure Iodine intake Obesity/Diabetes Autoimmune Disease Estrogen/Progesterone Reduced smoking But most likely Increasing use of imaging technologies – Overdiagnosis
Possible Causes of Increasing Incidence • • Radiation Exposure Iodine intake Obesity/Diabetes Autoimmune Disease Estrogen/Progesterone Reduced smoking But most likely Increasing use of imaging technologies – Overdiagnosis
 Variable Presentation of Micro PTC • Found on thyroid surgery for benign disease • Occult nodule found on conventional imaging done for other purposes • PET positivity thyroid done for other purposes • Less than 1 cm nodule palpable on a lean neck , usually the isthmus • Evidence of neck node metastases with negative thyroid US or mica nodule • Evidence of distant metastases with benign appearing US or micro nodule in thyroid
Variable Presentation of Micro PTC • Found on thyroid surgery for benign disease • Occult nodule found on conventional imaging done for other purposes • PET positivity thyroid done for other purposes • Less than 1 cm nodule palpable on a lean neck , usually the isthmus • Evidence of neck node metastases with negative thyroid US or mica nodule • Evidence of distant metastases with benign appearing US or micro nodule in thyroid
 Case 1 Incidental PTC and benign thyroid nodule • . A B Lt Longitudinal FNA shows: A, PTC
Case 1 Incidental PTC and benign thyroid nodule • . A B Lt Longitudinal FNA shows: A, PTC
 Case-2 • old 66 year. lady a palpable level IIb Rt FNA positive for PTC US 4 mm hypoechoic nodule Rt lobe no suspicious features. 2. 3 cm nodule Rt upper neck with proven FNA shows PTC
Case-2 • old 66 year. lady a palpable level IIb Rt FNA positive for PTC US 4 mm hypoechoic nodule Rt lobe no suspicious features. 2. 3 cm nodule Rt upper neck with proven FNA shows PTC
 Rt upper neck PTC Mets RT lobe transverse Case-2 Rt lobe longitudinal
Rt upper neck PTC Mets RT lobe transverse Case-2 Rt lobe longitudinal
 Case-2 • Surgery: bilateral thyroidectomy 3 mm PTC Rt upper pole and 2 mm left lower pole. Other than palpable 2. 3 cm nodule 35 nodes IIa , II, II and IV, VI were negative • RAI therapy • No recurrence , Tg undetectable at one year F/U
Case-2 • Surgery: bilateral thyroidectomy 3 mm PTC Rt upper pole and 2 mm left lower pole. Other than palpable 2. 3 cm nodule 35 nodes IIa , II, II and IV, VI were negative • RAI therapy • No recurrence , Tg undetectable at one year F/U
 Case-3 • A female in 2000 at age 59 presented with multiple lung nodules biopsy was PTC • US of thyroid showed benign appearing less than 6 mm nodules, no lymphadenopathy • Bilateral thyroidectomy, only 5 mm Occult PTC Rt lobe • One central node compartment positive
Case-3 • A female in 2000 at age 59 presented with multiple lung nodules biopsy was PTC • US of thyroid showed benign appearing less than 6 mm nodules, no lymphadenopathy • Bilateral thyroidectomy, only 5 mm Occult PTC Rt lobe • One central node compartment positive
 Case -3 • Remnant ablation, 2 doses of 200 m. Ci I-131 • Good uptake in lung metastases in 2001 and 2002 • Last WBS negative in 2005 • Lung nodules stable less than 6 mm 20042014 • Excellent quality of life at last visit in Nov 2014
Case -3 • Remnant ablation, 2 doses of 200 m. Ci I-131 • Good uptake in lung metastases in 2001 and 2002 • Last WBS negative in 2005 • Lung nodules stable less than 6 mm 20042014 • Excellent quality of life at last visit in Nov 2014
 • • • Median") Outcome of 900 Micro PTC 1994 -2004 (Mayo Data) • • • Median size 7 mm 85% bilateral lobectomy, RAI in 17% 30% neck node positive 0. 3% distant mets, 0. 6% incomplete excision 0. 3% died of PTC, Recurrence rate in 40 Yrs 6% Higher recurrence in multifocal tumors, and node positives • 99% not at risk of distant spread or mortality • RAI or bilateral lobectomy did not change outcome Hay ID, surgery; 2008; 144: 980
Outcome of 900 Micro PTC 1994 -2004 (Mayo Data) • • • Median size 7 mm 85% bilateral lobectomy, RAI in 17% 30% neck node positive 0. 3% distant mets, 0. 6% incomplete excision 0. 3% died of PTC, Recurrence rate in 40 Yrs 6% Higher recurrence in multifocal tumors, and node positives • 99% not at risk of distant spread or mortality • RAI or bilateral lobectomy did not change outcome Hay ID, surgery; 2008; 144: 980
 14045 Micro Papillary Cancer in Korea Single Institution 1986 -2013 • • • Total thyroidectomy 47%, less than total 53% Central compartment node 27% lateral neck 4. 9% 10 -20 yrs. survivals 98% and 94% 10 -20 yrs. disease free survivals, 97% and 94% No difference between thyroidectomy total and less than total Lee c et. al. Presented in OCT 2014, ATA Meeting
14045 Micro Papillary Cancer in Korea Single Institution 1986 -2013 • • • Total thyroidectomy 47%, less than total 53% Central compartment node 27% lateral neck 4. 9% 10 -20 yrs. survivals 98% and 94% 10 -20 yrs. disease free survivals, 97% and 94% No difference between thyroidectomy total and less than total Lee c et. al. Presented in OCT 2014, ATA Meeting
 Reported Complications of Thyroid Surgery 30 Surgery 140: 1000 -1005, 2006 Arch Surg 383: 167 -169, 1998 Ann Surg 245: 604 -610, 2007 Cancer 115: 251 -258, 2009 25 20 LNI 15 HPT T LNI 10 5 0 T HPT % LB TT Brito JP, et. al. . BMJ 2014 in press. TT+PLND
Reported Complications of Thyroid Surgery 30 Surgery 140: 1000 -1005, 2006 Arch Surg 383: 167 -169, 1998 Ann Surg 245: 604 -610, 2007 Cancer 115: 251 -258, 2009 25 20 LNI 15 HPT T LNI 10 5 0 T HPT % LB TT Brito JP, et. al. . BMJ 2014 in press. TT+PLND
 Less-aggressive treatment options for Micro-papillary Thyroid Cancer • Lobectomy vs. bilateral surgery • Targeted ablative procedures – Percutaneous ethanol ablation – Radiofrequency ablation (RFA) – Cryoablation • Active surveillance
Less-aggressive treatment options for Micro-papillary Thyroid Cancer • Lobectomy vs. bilateral surgery • Targeted ablative procedures – Percutaneous ethanol ablation – Radiofrequency ablation (RFA) – Cryoablation • Active surveillance
 Observation for Micro PTC Better Active surveillance
Observation for Micro PTC Better Active surveillance
 AWARENESS ABOUT THE EXISTENCE OF TREATMENT OPTIONS Ito Y, World J Surg 2010; 34: 28 -35
AWARENESS ABOUT THE EXISTENCE OF TREATMENT OPTIONS Ito Y, World J Surg 2010; 34: 28 -35
 Active Surveillance for Micro-PTC Age of Patient • • • 1235 patient chose observation 1993 -2011 Progression lowest in over age 60 Highest in the younger
Active Surveillance for Micro-PTC Age of Patient • • • 1235 patient chose observation 1993 -2011 Progression lowest in over age 60 Highest in the younger
 Active Surveillance of Micro-PTC 20 years F/u >3 mm growth Age effect Ito Y, Thyroid 2014 Lymph node mets Age effect
Active Surveillance of Micro-PTC 20 years F/u >3 mm growth Age effect Ito Y, Thyroid 2014 Lymph node mets Age effect
 Distinct Types of Micro PTC Under Observation • I- Incidental finding – observed and no change in size • II- Increase in size during observation – Lobectomy is suggested • III- Clinically symptomatic, needs more aggressive management • 230 out of 244 accepted observation300 lesions: 5 year observation: 7% increase in size, 90% unchanged 3% decreased: Conclusion: Observation 95% are type I and can be observed Sugitani I etal World I surg 2010 ; 34: 1222
Distinct Types of Micro PTC Under Observation • I- Incidental finding – observed and no change in size • II- Increase in size during observation – Lobectomy is suggested • III- Clinically symptomatic, needs more aggressive management • 230 out of 244 accepted observation300 lesions: 5 year observation: 7% increase in size, 90% unchanged 3% decreased: Conclusion: Observation 95% are type I and can be observed Sugitani I etal World I surg 2010 ; 34: 1222
 Tumors not Candidate for Active Surveillance • • Peripheral and bulging Close to trachea with angle over 90 degrees Evidence of node or distance mets Multifocal? Family history of non medullary thyroid cancer History of radiation exposure PET positive tumors? Patient preference
Tumors not Candidate for Active Surveillance • • Peripheral and bulging Close to trachea with angle over 90 degrees Evidence of node or distance mets Multifocal? Family history of non medullary thyroid cancer History of radiation exposure PET positive tumors? Patient preference
 Minimally Invasive Intervention • • • Ethanol ablation Radio-frequency ablation Cryoablation
Minimally Invasive Intervention • • • Ethanol ablation Radio-frequency ablation Cryoablation
 Ethanol Ablation for Micro-papillary Thyroid Cancer –Mayo pilot study 13 patients, 9 F, 4 M, 5 with co-morbidity, ages 36 -86 Tumor sized 4 -13 mm, injection of 95% alcohol, 2 injections in subsequent days, Ethanol 0. 45 -1. 25 F/u 0. 3 -4. 4 yrs. Medium 1. 6 yrs. Median volium reduction 76 % all shrunk 4 disappeared Conclusion: For micropapilalry thyroid cancer, patients not comfortable with surgery or active survellance ethanol ablation may be a n attractive minimally invasive option Hay, ID et al , ITC 2015
Ethanol Ablation for Micro-papillary Thyroid Cancer –Mayo pilot study 13 patients, 9 F, 4 M, 5 with co-morbidity, ages 36 -86 Tumor sized 4 -13 mm, injection of 95% alcohol, 2 injections in subsequent days, Ethanol 0. 45 -1. 25 F/u 0. 3 -4. 4 yrs. Medium 1. 6 yrs. Median volium reduction 76 % all shrunk 4 disappeared Conclusion: For micropapilalry thyroid cancer, patients not comfortable with surgery or active survellance ethanol ablation may be a n attractive minimally invasive option Hay, ID et al , ITC 2015
 2015 ATA Guidelines Changing Diagnostic and Treatment Recommendation • • • Less aggressive detection Less aggressive surgery for low risk PTC Less RAI therapy for remnant ablation Lower dose RAI for remnant ablation Central compartment Node excision optional for Low risk PTC
2015 ATA Guidelines Changing Diagnostic and Treatment Recommendation • • • Less aggressive detection Less aggressive surgery for low risk PTC Less RAI therapy for remnant ablation Lower dose RAI for remnant ablation Central compartment Node excision optional for Low risk PTC
 Haugen et al Thyroid 2015
Haugen et al Thyroid 2015
 2015 ATA Guidelines for Thyroid Nodule Haugen et al, Thyroid, 2015 Nodule TSH normal or high US High suspicion Intermediate pattern FNA >1 cm Low suspicion FNA >1. 5 cm Pure cyst or benign pattern No FNA Very low suspicion FNA >2 cm
2015 ATA Guidelines for Thyroid Nodule Haugen et al, Thyroid, 2015 Nodule TSH normal or high US High suspicion Intermediate pattern FNA >1 cm Low suspicion FNA >1. 5 cm Pure cyst or benign pattern No FNA Very low suspicion FNA >2 cm
 2009 ATA Guidelines Recommendation • For >1 cm initial surgery bilateral near -or total unless contraindications • Lobectomy for <1 cm, uni-focal intra-thyroidal low risk PTC unless prior head and neck radiation or lymph node involvement (recommendation A) Thyroid ; Nov 2009
2009 ATA Guidelines Recommendation • For >1 cm initial surgery bilateral near -or total unless contraindications • Lobectomy for <1 cm, uni-focal intra-thyroidal low risk PTC unless prior head and neck radiation or lymph node involvement (recommendation A) Thyroid ; Nov 2009
 2015 ATA Guidelines for Micro-papillary Thyroid cancer • Less than 1 cm suspect nodule no FNA and observe particularly in older • When diagnosed R/O metastasis , if unifocal , no radiation history or syndromal PTC: lobectomy and no lymph node sampling • May consider active surveillance, in certain situations • 1 -4 cm no other risks lobectomy a Haugen et al. Thyroid 2015 consideration
2015 ATA Guidelines for Micro-papillary Thyroid cancer • Less than 1 cm suspect nodule no FNA and observe particularly in older • When diagnosed R/O metastasis , if unifocal , no radiation history or syndromal PTC: lobectomy and no lymph node sampling • May consider active surveillance, in certain situations • 1 -4 cm no other risks lobectomy a Haugen et al. Thyroid 2015 consideration
 Evaluate and Consider Less-aggressive Treatment Options • Lobectomy vs. bilateral surgery • Emerging targeted ablative procedures – Percutaneous ethanol ablation – Radiofrequency ablation – Cryoablation • Active surveillance
Evaluate and Consider Less-aggressive Treatment Options • Lobectomy vs. bilateral surgery • Emerging targeted ablative procedures – Percutaneous ethanol ablation – Radiofrequency ablation – Cryoablation • Active surveillance
 Management of Occult Papillary Thyroid Cancer • For unilateral incidental : Lobectomy if unifocal or multifocal Observation may be an option • For incidental found on surgery less than 1 cm Lobectomy and no radioactive iodine, No data if T 4 therapy is needed • With lymph node metastasis or distant metastases at presentation Near total thyroidectomy and RAI remnant ablation for stages II (younger than 45) and Stages III and IV (older than age 45) • For PET positive incidental PTC Perhaps more aggressive, but data is needed
Management of Occult Papillary Thyroid Cancer • For unilateral incidental : Lobectomy if unifocal or multifocal Observation may be an option • For incidental found on surgery less than 1 cm Lobectomy and no radioactive iodine, No data if T 4 therapy is needed • With lymph node metastasis or distant metastases at presentation Near total thyroidectomy and RAI remnant ablation for stages II (younger than 45) and Stages III and IV (older than age 45) • For PET positive incidental PTC Perhaps more aggressive, but data is needed
 Management of Occult Papillary Thyroid Cancer Special situations when more aggressive bilateral near total or total thyroidectomy may be needed • History of head and neck radiation • Non- medullary hereditary differentiated thyroid cancer or family history in first degree relatives • PTC larger >1. 5 cm or extra thyroidal extension • Syndromic FCDTC • PTC found on PET? (data needed)
Management of Occult Papillary Thyroid Cancer Special situations when more aggressive bilateral near total or total thyroidectomy may be needed • History of head and neck radiation • Non- medullary hereditary differentiated thyroid cancer or family history in first degree relatives • PTC larger >1. 5 cm or extra thyroidal extension • Syndromic FCDTC • PTC found on PET? (data needed)
 Issues Needing More Data • • If observation is chosen should T 4 therapy given? If lobectomy is done should therapy with T 4 given? Should multifocal PTC be treated differently? Should non- invasive ehanol or RFA ablation be a standard option for diagnosed occult PTC • Should we be less aggressive in performing FNA for less than 1 cm suspect incidental PTCs specially in elderly ? • Need confirmation that older asymptomatic patients with Micro PTC are not subject to higher age related risk
Issues Needing More Data • • If observation is chosen should T 4 therapy given? If lobectomy is done should therapy with T 4 given? Should multifocal PTC be treated differently? Should non- invasive ehanol or RFA ablation be a standard option for diagnosed occult PTC • Should we be less aggressive in performing FNA for less than 1 cm suspect incidental PTCs specially in elderly ? • Need confirmation that older asymptomatic patients with Micro PTC are not subject to higher age related risk
 Micropapillary Thyroid Cancer Found on PET scans • • • 12 patients with incidental PET positive PTC 25% multifocal 66% extra thyroidal extension 41% angioinvasion 16% lung mets Conclusion: 92% had intermediate or high risk per ATA criteria. Thyroid carcinomas detected by 18 -F-FDG PPET have aggressive histology and likely worse prognosis Pedro Marques et. al. Endo Practice 2014; 20: 1129
Micropapillary Thyroid Cancer Found on PET scans • • • 12 patients with incidental PET positive PTC 25% multifocal 66% extra thyroidal extension 41% angioinvasion 16% lung mets Conclusion: 92% had intermediate or high risk per ATA criteria. Thyroid carcinomas detected by 18 -F-FDG PPET have aggressive histology and likely worse prognosis Pedro Marques et. al. Endo Practice 2014; 20: 1129
 CHOOSING THE “RIGHT” TREATMENT A 44 -year-old executive concerned about future metastatic disease might opt for thyroid surgery A singer, or a public speaker, concerned about the possible perioperative damage to voice may opt for active surveillance
CHOOSING THE “RIGHT” TREATMENT A 44 -year-old executive concerned about future metastatic disease might opt for thyroid surgery A singer, or a public speaker, concerned about the possible perioperative damage to voice may opt for active surveillance
 Conclusion-1 • Worldwide increase in papillary thyroid cancer is mostly related to increased imaging and finding of non–significant micro -PTC • Incidentally discovered micro PTC in thyroidectomy for benign disease can be considered not clinically significant and no further action is needed • For PTC less than 1. 0 cm active surveillance may be offered in future if acceptable to the patient
Conclusion-1 • Worldwide increase in papillary thyroid cancer is mostly related to increased imaging and finding of non–significant micro -PTC • Incidentally discovered micro PTC in thyroidectomy for benign disease can be considered not clinically significant and no further action is needed • For PTC less than 1. 0 cm active surveillance may be offered in future if acceptable to the patient
 Conclusion-2 • Decision for FNA of a <1. 5 m nodule if incidentally discovered should be more conservative following 2015 ATA guidelines • Controlled studies of active surveillance vs. surgery or minimally invasive procedure such as alcohol ablation are underway • If surgery is chosen for incidental micro PTC Lobectomy should be adequate and central compartment node sampling may not be needed
Conclusion-2 • Decision for FNA of a <1. 5 m nodule if incidentally discovered should be more conservative following 2015 ATA guidelines • Controlled studies of active surveillance vs. surgery or minimally invasive procedure such as alcohol ablation are underway • If surgery is chosen for incidental micro PTC Lobectomy should be adequate and central compartment node sampling may not be needed
 Conclusion-3 • Rare cases of Micro PTC with significant neck node mets or distant mets exist. But they are usually diagnosed by clinical metastasis and primary source may be occult and their management is according to the staging of the cancer
Conclusion-3 • Rare cases of Micro PTC with significant neck node mets or distant mets exist. But they are usually diagnosed by clinical metastasis and primary source may be occult and their management is according to the staging of the cancer
 That is it! Thank YOU
That is it! Thank YOU
 2002 Incidence of thyroid cancer in multiple countries, 1985 vs. 2002 1985 Brito JP. BMJ 2013; 347: f 4706
2002 Incidence of thyroid cancer in multiple countries, 1985 vs. 2002 1985 Brito JP. BMJ 2013; 347: f 4706
 Clinically “silent” disease
Clinically “silent” disease
 Clinically “silent” disease
Clinically “silent” disease
 IDENTIFICATION OF PATIENTS AT LOW RISK No family history of thyroid cancer No personal history of radiation exposure PTCC LOW RISK PTC <1. 5 cm lesion compatible with papillary thyroid cancer on cytology – no unusual histology No evidence of extraglandular extension or lymph node metastasis
IDENTIFICATION OF PATIENTS AT LOW RISK No family history of thyroid cancer No personal history of radiation exposure PTCC LOW RISK PTC <1. 5 cm lesion compatible with papillary thyroid cancer on cytology – no unusual histology No evidence of extraglandular extension or lymph node metastasis
 LOOKING AHEAD • The term micro. PLIC should also be tested to ensure that it promotes careful deliberation and patient-centered treatment. • RCT of active surveillance vs. thyroid surgery and other potential treatment options for PLICs • Role of decision aids to avoid overtreatment for PLICs • Interventions to prevent overdiagnosis and overtreatment of PLICs – Molecular or other markers of aggression – Less invasive treatment options – PEI, RFA, Laser, etc • Role of guidelines and recommendations to overcome overdiagnosis and overtreatment
LOOKING AHEAD • The term micro. PLIC should also be tested to ensure that it promotes careful deliberation and patient-centered treatment. • RCT of active surveillance vs. thyroid surgery and other potential treatment options for PLICs • Role of decision aids to avoid overtreatment for PLICs • Interventions to prevent overdiagnosis and overtreatment of PLICs – Molecular or other markers of aggression – Less invasive treatment options – PEI, RFA, Laser, etc • Role of guidelines and recommendations to overcome overdiagnosis and overtreatment
 Recent rise in thyroid cancer incidence is related to discovery of a reservoir of previously unrecognized subclinical disease: a population-based study in Olmsted County, Minnesota during 2000 through 2012 2000 -2012 1935 -1999 (263) 2000 -2012 (213) 46 (17. 8) 46. 3(14. 9) 49. 6 (14. 9) 42. 7 (14. 14)* 193 (73) 149 (79) 79 (70) 70 (70) 1. 98 (1. 6) 1. 76 (1. 2)* 1. 3 (1) 2. 26 (1. 2)* MACIS score (Mean, SD) 4. 6 (1. 5) 4. 7(1. 3) 4. 6 (1. 2) 4. 7 (1. 4) MACIS score < 6 ( N, %) 184 (86) 175 (88) 94 (87) 81 (89) Age at Diagnosis in years ( Mean, SD) Female N(%) Size of tumor ( Mean, SD) Type of thyroid Cancer Clinically occult (113) Clinically recognized (100) Papillary ( N, %) 215 (82) 199 (93)* 108 (96) 91 (91) Follicular( N, %) 15(6) 6 (3) 3 (2) 3 (3) Hurtle( N, %) 19(7) 1 (0. 5) 1 (1) 0 (0) Medullary( N, %) 38 (2) 4 (2) 1 (1) 3 (3) Metastatic( N, %) 0 (0) 1 (0. 5) 0 (0) 1 (1) Anaplastic ( N, %) 6(2) 0 (0) Lymphoma( N, %) 0 (0) 2(1) 0 (0) 2 (2)
Recent rise in thyroid cancer incidence is related to discovery of a reservoir of previously unrecognized subclinical disease: a population-based study in Olmsted County, Minnesota during 2000 through 2012 2000 -2012 1935 -1999 (263) 2000 -2012 (213) 46 (17. 8) 46. 3(14. 9) 49. 6 (14. 9) 42. 7 (14. 14)* 193 (73) 149 (79) 79 (70) 70 (70) 1. 98 (1. 6) 1. 76 (1. 2)* 1. 3 (1) 2. 26 (1. 2)* MACIS score (Mean, SD) 4. 6 (1. 5) 4. 7(1. 3) 4. 6 (1. 2) 4. 7 (1. 4) MACIS score < 6 ( N, %) 184 (86) 175 (88) 94 (87) 81 (89) Age at Diagnosis in years ( Mean, SD) Female N(%) Size of tumor ( Mean, SD) Type of thyroid Cancer Clinically occult (113) Clinically recognized (100) Papillary ( N, %) 215 (82) 199 (93)* 108 (96) 91 (91) Follicular( N, %) 15(6) 6 (3) 3 (2) 3 (3) Hurtle( N, %) 19(7) 1 (0. 5) 1 (1) 0 (0) Medullary( N, %) 38 (2) 4 (2) 1 (1) 3 (3) Metastatic( N, %) 0 (0) 1 (0. 5) 0 (0) 1 (1) Anaplastic ( N, %) 6(2) 0 (0) Lymphoma( N, %) 0 (0) 2(1) 0 (0) 2 (2)
 Thyroid Incidental Micro-cancer In Autopsy : • Finland n=101 • 35% thyroid cancer • ( 2 -3 mm cuts) (range 0. 1 mm 15 mm) 67% under 1 mm
Thyroid Incidental Micro-cancer In Autopsy : • Finland n=101 • 35% thyroid cancer • ( 2 -3 mm cuts) (range 0. 1 mm 15 mm) 67% under 1 mm
 Thyroid Cancer Reservoir First author, year Ottino 1989 Martinez-Tello 1993 Solares 2005 Men N (%) USA (Mayo Clinic) All nodules 318/821 (38%) 191/538 (34%) Finland All of gland 13/48 23/53 (43%) ‘Suspicious areas’ only 24/421 39/599 (6%) (7%) not clearly defined 3/41 8/59 (14%) 6/34 16/66 (18%) Lang 1988 Women N (%) (7%) Harach 1985 Method (27%) Mortensen 1955 (& Woolner) Country (24%) 1/34 2/116 (3%) (2%) Germany Argentina Spain Guatemala All of gland ‘Suspicious areas’ only
Thyroid Cancer Reservoir First author, year Ottino 1989 Martinez-Tello 1993 Solares 2005 Men N (%) USA (Mayo Clinic) All nodules 318/821 (38%) 191/538 (34%) Finland All of gland 13/48 23/53 (43%) ‘Suspicious areas’ only 24/421 39/599 (6%) (7%) not clearly defined 3/41 8/59 (14%) 6/34 16/66 (18%) Lang 1988 Women N (%) (7%) Harach 1985 Method (27%) Mortensen 1955 (& Woolner) Country (24%) 1/34 2/116 (3%) (2%) Germany Argentina Spain Guatemala All of gland ‘Suspicious areas’ only
 IDENTIFICATION OF PATIENTS AT LOW RISK 10 <1 cm Rate per 100 000 8 6 1 -2. 5 cm 4 2 0 >3 cm 1975 1979 1983 1987 1991 1995 1999 2003 2007 Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html
IDENTIFICATION OF PATIENTS AT LOW RISK 10 <1 cm Rate per 100 000 8 6 1 -2. 5 cm 4 2 0 >3 cm 1975 1979 1983 1987 1991 1995 1999 2003 2007 Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. html
 Case-1 What should be management? • • 1 - Radioactive iodine remnant ablation 2 -Suppressive thyroxine therapy to TSH< 0. 1 3 -Annual thyroid US for 5 years 4 -No follow up neck US is needed
Case-1 What should be management? • • 1 - Radioactive iodine remnant ablation 2 -Suppressive thyroxine therapy to TSH< 0. 1 3 -Annual thyroid US for 5 years 4 -No follow up neck US is needed
 Case-2 1. Patient needs completion thyroidectomy 2. Patient needs central compartment node sampling 3. If FNA of the larger nodule was benign observation might have been an option 4. None of the above
Case-2 1. Patient needs completion thyroidectomy 2. Patient needs central compartment node sampling 3. If FNA of the larger nodule was benign observation might have been an option 4. None of the above
 Study Points to Overdiagnosis of Thyroid Cancer New York Times, November 6, 2014 Korea's Thyroid-Cancer “Epidemic” — Screening and Overdiagnosis N Engl J Med 2014; 371: 1765 -1767 November 6, 2014 Thyroid cancer (PTC) is now the most Prevalent cancer in Korea.
Study Points to Overdiagnosis of Thyroid Cancer New York Times, November 6, 2014 Korea's Thyroid-Cancer “Epidemic” — Screening and Overdiagnosis N Engl J Med 2014; 371: 1765 -1767 November 6, 2014 Thyroid cancer (PTC) is now the most Prevalent cancer in Korea.
 Study Points to Overdiagnosis of Thyroid Cancer New York Times, November 6, 2014 Korea's Thyroid-Cancer “Epidemic” — Screening and Overdiagnosis N Engl J Med 2014; 371: 1765 -1767 November 6, 2014 Thyroid cancer (PTC) is now the most Prevalent cancer in Korea.
Study Points to Overdiagnosis of Thyroid Cancer New York Times, November 6, 2014 Korea's Thyroid-Cancer “Epidemic” — Screening and Overdiagnosis N Engl J Med 2014; 371: 1765 -1767 November 6, 2014 Thyroid cancer (PTC) is now the most Prevalent cancer in Korea.
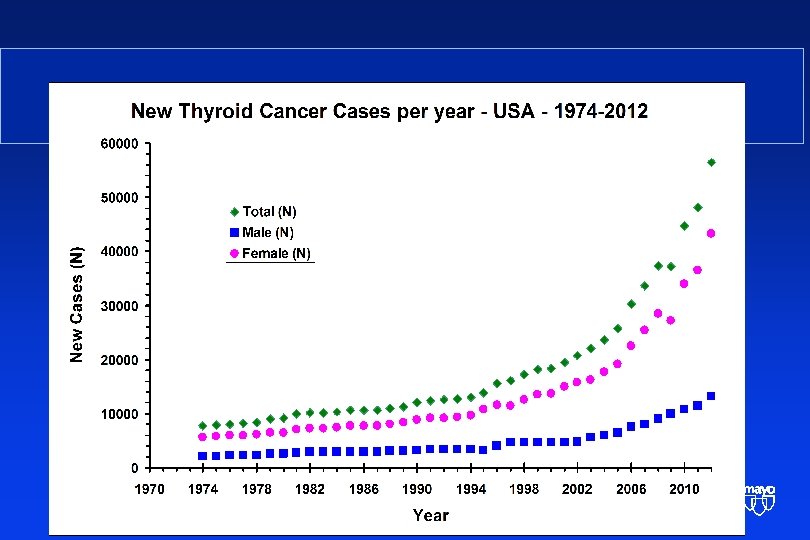
 Incidence Rates for Thyroid Cancer Rate per 100 000 14. 3 4. 8 Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/t hyro. html
Incidence Rates for Thyroid Cancer Rate per 100 000 14. 3 4. 8 Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/t hyro. html
 comprise up") Differentiated Thyroid Carcinoma • Follicular cell derived thyroid carcinomas (PTC and FTC) comprise up to 95% of all thyroid carcinomas • The vast majority of these tumors are well differentiated Grebe & Hay 1995
Differentiated Thyroid Carcinoma • Follicular cell derived thyroid carcinomas (PTC and FTC) comprise up to 95% of all thyroid carcinomas • The vast majority of these tumors are well differentiated Grebe & Hay 1995
 Case-1 • 32 year old lady seen in 2012 with hyperthyroidism, • Thyroid US: Heterogenous pattern and tiny nodularity not suspicious. Isotopic scan diffuse enlargement, serology consistent with Graves • Treated for 2 years with antithyroid medications poor response • Surgery in 2014 bilateral diffuse hyperplasia. Left lobe had 1. 3 cm follicular variant of PTC • What should be management?
Case-1 • 32 year old lady seen in 2012 with hyperthyroidism, • Thyroid US: Heterogenous pattern and tiny nodularity not suspicious. Isotopic scan diffuse enlargement, serology consistent with Graves • Treated for 2 years with antithyroid medications poor response • Surgery in 2014 bilateral diffuse hyperplasia. Left lobe had 1. 3 cm follicular variant of PTC • What should be management?
 Case -2 68 year old with a palpable newly found 2. 5 cm nodule in the left
Case -2 68 year old with a palpable newly found 2. 5 cm nodule in the left
 Case-2 • Lobectomy done • The 2. 5 cm lesion was follicular benign adenoma • 5 mm PTC in the left lobe and also 2 other foci of 2 and 3 mm PTC
Case-2 • Lobectomy done • The 2. 5 cm lesion was follicular benign adenoma • 5 mm PTC in the left lobe and also 2 other foci of 2 and 3 mm PTC
 Increasing Diagnosis of Micro-papillary Thyroid Cancer New Trends in Management No Disclosure
Increasing Diagnosis of Micro-papillary Thyroid Cancer New Trends in Management No Disclosure