bc7dbead0f325e666043bad57fa85473.ppt
- Количество слайдов: 47



Impact of a Diabetic Registry in a Primary Care Network Steven Ashmead MD, Associate Director, Grand Rapids Family Medicine Residency Phil Baty MD, Chair, Quality Improvement Committee, Advantage Health Physicians

100 + Primary Care Physicians 14 Offices 4 Clinics 2 Resident clinics

Wege Family Medicine Clinic • 27 Residents • Four faculty providers 2. 3 half days a week in patient care • Nurse Practitioner 0. 6 patient care per week • Patient Mix - Medicaid/Medicare 65% - Commercial 15% - HMO 10% - No insurance 10%

Wege Family Medicine Clinic • Urban location • 12, 823 office visits 2005 • Patient mix - African American 18% - Asian 6% - Hispanic 12% - Native American 2% - Other 14%


Goal • You can make an all payer registry even if you don’t have an EMR.

Objectives • • • Barriers Registry Overview Our registry Implementation Results Next Steps

Barriers to Implementation of Chronic Care Improvements • Physicians work part time • Physicians don’t buy in - Faculty § Academic freedom § Lack of knowledge/modeling - Inertia Challenges to Improving Chronic Disease Care and Training in Residencies, Academic Medicine 2006

Barriers to Implementation of Chronic Care in Residencies • Residents - Continuity is difficult § Resident turnover § Limited time in Health Center - Learning Fatigue - Chronic care not exciting - Limited time PDSA and implement new routines - Residents are tired and overwhelmed Challenges to Improving Chronic Disease Care and Training in Residencies, Academic Medicine 2006

Cochrane Review 2006 No. 4 • The review found that multifaceted professional interventions (for example combinations of postgraduate education, reminders, audit and feedback, local consensus processes, and peer review) could enhance the performance of care providers. • The effectiveness of these interventions on patient outcomes (glycaemic control, cardiovascular risk factors, wellbeing) is less clear.

Why ‘points out the importance of good patient information and using information to improve outcomes’


Registry Functions • Ensure regular follow up • Embed evidence based guidelines into daily practice • Integrate specialist expertise and primary care • Provide timely reminders

Registry Functions • Identify relevant subpopulations for targeted care • Facilitate individual patient care planning • Share information with patients / providers to coordinate care • Monitor performance of patient care team/system

Why A Registry In Grand Rapids? • AH Value Quality • Changing Health Care Environment - P 4 P - National Quality Standards - Market Forces
 Blue Care Network Health Plan of Michigan")
P 4 P Expectations BCBSM PGIP (Target) Blue Care Network Health Plan of Michigan Priority Health (Target) DOQIT NQF A 1 c screening in 2005 89% Screen only X Not measured X X A 1 c < 7. 0 in 2005 (most recent test) 40% Not measured 60% Not measured Poor controlled A 1 c > 9. 0 20% Not measured X X Controlled BP < 130/80 Not measured 34% X X Cholesterol Screening Not measured X X LDL < 100 in 2004 OR 2005 (most recent test) 36% Screen only X 42% X X Microalbumin screening in 2005 OR a diagnosis of nephropathy 80% Screen only X 62% X X Retinal exam in 2005 60% Screen only X 64% X X Foot assessment Not measured X X Smoking status/advice or treatment Not measured Not measured Indicator Not measured

HEDIS Comprehensive Diabetes Care • • Hgb. A 1 C testing Poor Hgb. A 1 C control >9. 5% Eye exams HDL - cholesterol screening LDL - cholesterol level Monitoring nephropathy –micro albumin BP < 130/80

Market Forces • Creation of Quality score cards

Creating the Team • • • Physician champions Nursing leadership Pharm. D IT – staff Quality Improvement Committee

2005 Diabetes Guideline

Guideline Outcomes • • Eye care Yearly CHD Yearly assessment Visits Quarterly Immunizations Flu, pneumonia Foot care Yearly Patient Education CDE Dietician initially and if uncontrolled Aspirin use Recommended Tobacco use A 4 • Hg. BA 1 c <7. 0 • Preprandial 90 -130 • Postprandial 110 -150 • Kidney yearly <30 ug/mg • Lipids LDL<100 • Blood Pressure <130/80

Diabetic Registry Criteria • • 18 – 75 years of age Patient active in practice Documented 250. XX code Patient list validated by the PCP verifying: - The patient has Diabetes - The physician is currently managing the patient

Identify Patients • Billing system MISYS • HMO data - Priority heath - Blue care network - Medicaid HMO • Minimum of two patient identifiers to identify unique patients • Unduplicated patients

Diabetes Registry Workflow Physician/Staff Reviews & Validates Registry Diabetics verified; Database updated w/ corrections & additional information (daily) Staff/Physicians Identify Care Opportunities Results captured Intervention Data refreshed Patient Outreach • Mailings • Phone • hart Reminders C

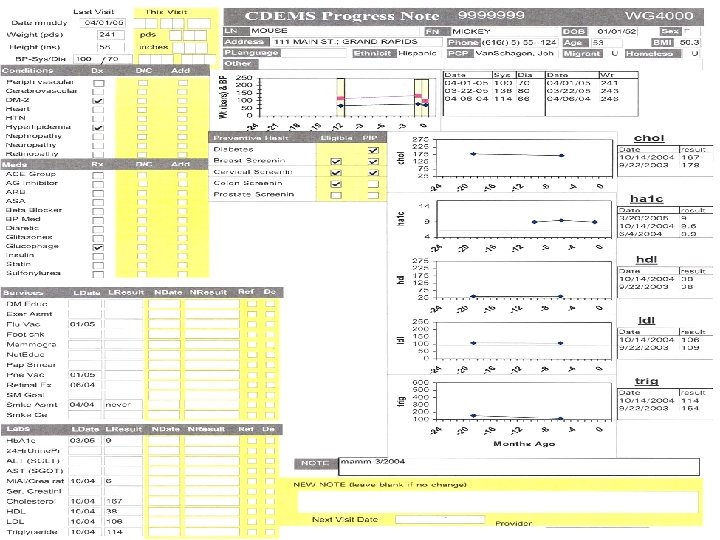
IT Support Tools Payer Data MISYS Practice Management Data • Claims • Eligibility • Rx Pathology Data Kent Radiology Data Warehouse Oracle Database CDEMS Retinal Exam Cerner Powerchart AS 400

Registry Reports • Patient reports at the point of care • Registry generated exceptions - Overdue For Care - Not meeting Management Goals • Aggregate Reports - Provider - Care Team - Organizational




Diabetic Outcomes 2004 -2005 All 2004 Number = 5551 2005 Number = 5504
 y")
Advantage Health Physicians Commercial Offices AH Offices 2004 AH Offices 2005 (N=4271 '04) y ro p at h 10 0 ep h L < N Measures LD LD L < 13 0 LD L >9 c A 1 <7 c A 1 c Ex am 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Ey e Percent Complete (N=3952 '05)

Wege Family Medicine Wege Offices 2004 Wege Offices 2005 y ro p at h 10 0 ep h L < N Measures LD LD L < 13 0 LD L >9 c A 1 <7 c A 1 c Ex am 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Ey e Percent complete (N=798 '04) (N=818 '05)

Diabetic Outcomes 2004 -2005 Underserved Clinics 2004 Number = 482 2005 Number = 734

Wege Clinics vs. National HEDIS Medicaid 50% Wege clinics 2005 HEDIS Medicaid 2005 NHANESIII 2000 100% 90% 70% 60% 50% 40% 30% 20% 10% o icr ex al in M am 0 Measures Re t L< LD LD L< 13 10 0 ne do L >9 . 0 <7 . 0 LD c do ne 0% A 1 Percent completed 80%

AHP vs. National HEDIS 50% Data Wege clinics 2005 HEDIS Commercial 2005 NHANESIII 2000 100% 90% 70% 60% 50% 40% 30% 20% 10% o icr ex al in M am 0 Measures Re t L< LD LD L< 13 10 0 ne do L >9 . 0 <7 . 0 LD c do ne 0% A 1 Percent completed 80%

PIP Settlements % of adjusted opportunity received in PIP Settlements 2001 -2004 $772, 662 Payout $820, 000 Adjusted Opportunity $560, 120 $474, 450 $393, 620 $488, 973 $334, 864 $208, 000 2001 2002 2003 2004 53% 71% 87% 94%

Paying Better Attention • Auditing and giving feedback • To individual patients through the use of global registries • Point of Care testing in offices Helps in delivering quality diabetes care in residency and commercial populations!

Next Steps • Continue to expand use of registry for chronic and preventative care • Implement self care management strategies • Work with specialists for education and expertise • Screen and treat for Depression

Resources • Cdems http: //www. cdems. com/ • California Health Care Foundation http: //www. chcf. org/topics/chronicdisease/index. cfm? item. ID=102741

Questions ashmeads@trinity-health. org batyp@trinity-health. org
bc7dbead0f325e666043bad57fa85473.ppt