a237c3d977666f130f945a4013687296.ppt
- Количество слайдов: 84



Idiopathic Membranous Glomerulopathy: Diagnosis and Treatment Geeta Gyamlani, MD

Clinical case • 35 yr old male pt s/b pcp • At that time, he was noted to have elevated total cholesterol of 353 mg/dl and triglycerides of 417 mg/dl and was started on simvastatin 40 mg/d • Next 2 mo, he started developing swelling + tenderness in his calves. Diagnosed with DVT was started on oral anticoagulant therapy.

• UA showed 3+ proteinuria, 24 hr urine showed 9 gms of protein. • Referred to Nephrology clinic • No DM, HTN, Macroscopic hematuria, • Serologic w/u for complements, monoclonal proteins, ANCA, Hep B, Hep. C, HIV and ANA negative • BP 137/87, wt 90 kg BMI 29 kg/m 2 • No LN, No JVD, 2+ LE edema

Lab data • Hb 15 g/dl, WBC 4. 7, plt 236, Cr 1, alb 2. 5, cholesterol 260, trig 224. • Proteinuria 8. 6 g/24 hrs • Cx. R normal • Renal US normal, renal veins were patent bilaterally
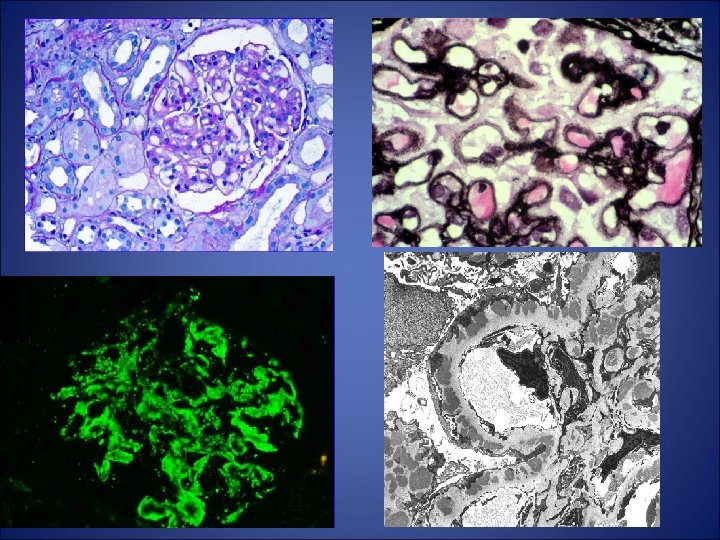
 • Full house pattern on IF")
Features of secondary membranous • Proliferative changes( measangial/endocapillary) • Full house pattern on IF • Glomerular deposits containing Ig other than Ig. G 4 • EDD in subendothelial , mesangium and along TBM+ vessel wall. • Endothelial tubuloreticular inclusions

Epidemiology • The second most common causes of primary NS in Caucasian adults ( upto 33% of adult cases of NS). • ~ 40% of patients eventually develop ESRD. • Because of its frequency, it remains the 2 nd or 3 rd cause of a primary glomerulopathy leading to ESRD. • Patients with MN who remain nephrotic are at an increased risk for thromboembolic and CV events.

Swaminathan et al Clin J Am Soc Nephrol 2006

Clinical manifestations M>F 2: 1 Peak incidence 4 -5 th decade of life 60 -70% have NS, 30 -40% have SNP. Microscopic hematuria may be seen in 30% patients • Majority of patients are normotensive and hypertension + in 10 -20%. • At presentation significant renal insufficiency <20% • •
 and immunoblotting (Panel C) show a lack")
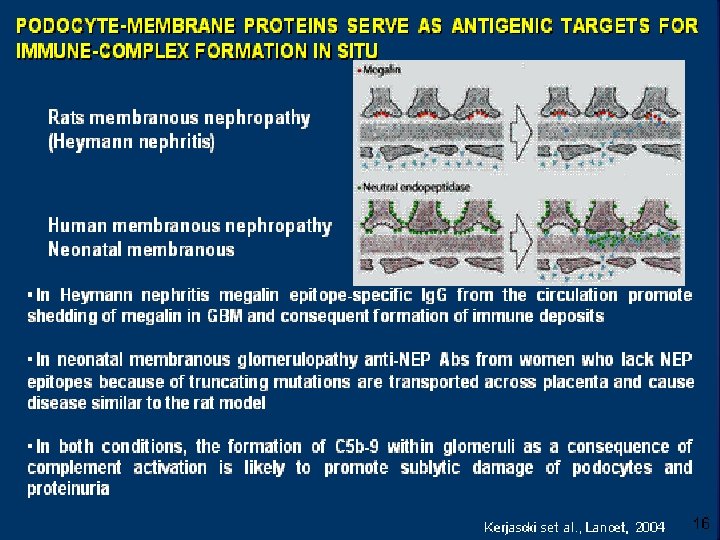
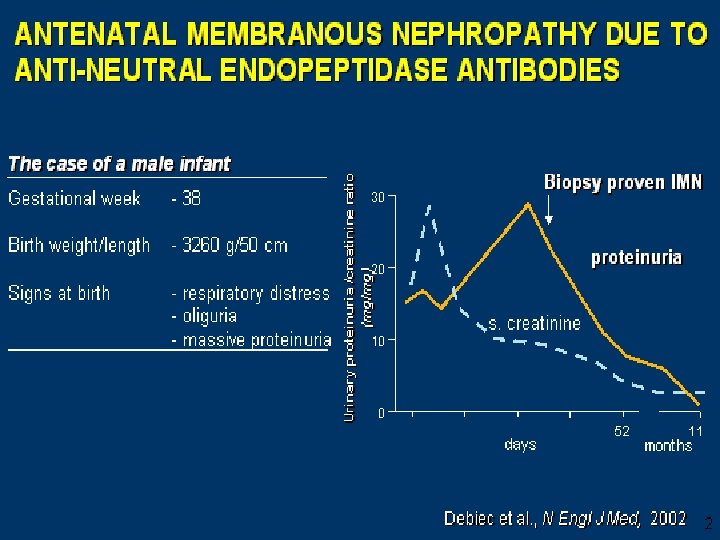
Fluorescence-activated cell-sorter analysis (Panels A and B) and immunoblotting (Panel C) show a lack of expression of neutral endopeptidase in the mother’s granulocytes. Debiec et al. NEJM 346 (26): 2053 June 27, 2002
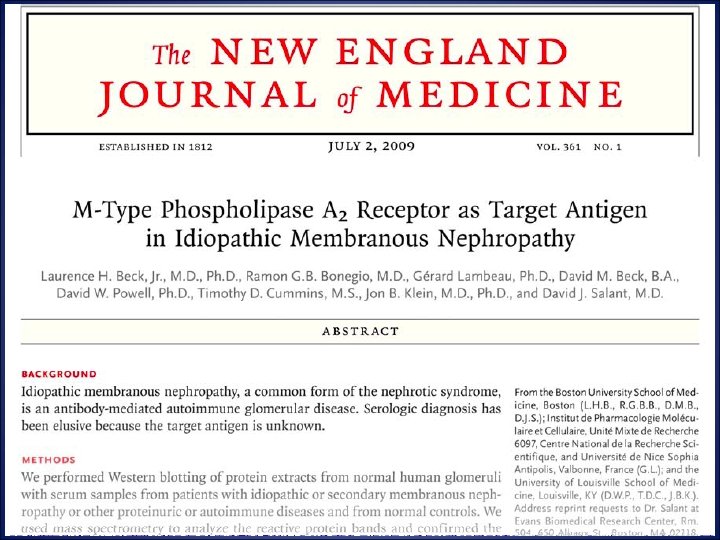

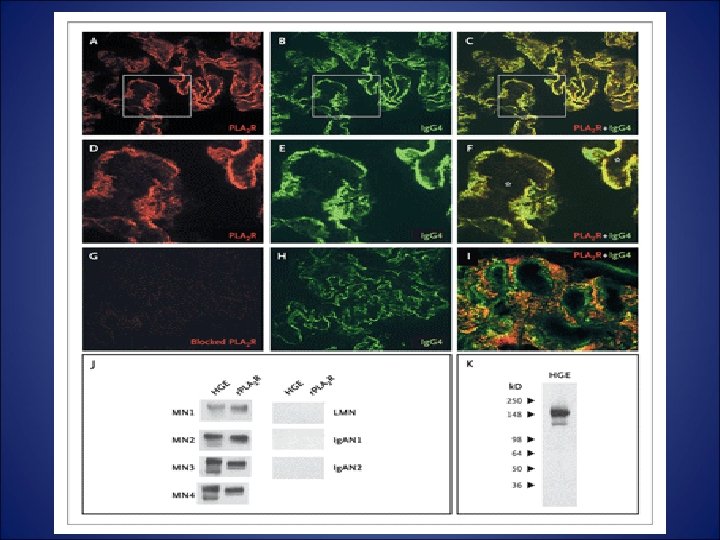
Results of Western Blotting of Glomerular Proteins with Serum from Patients with Idiopathic Membranous Nephropathy Western Blotting Beck et al: NEJM 361: 11, 2009 Reactivity to 185 -k. D Protein
")
Anti Phospholipase A 2 receptor Ab ( PLA 2 R)
 and immunological activity (circulating anti-PLA 2 R) Beck et")
Relationship between clinical disease (proteinuria) and immunological activity (circulating anti-PLA 2 R) Beck et al, Kidney International (2010) 77, 765– 770

Probability of renal survival from a pooled analysis of all 32 studies Cattran et al, Kidney International (2001) 59, 1983– 1994
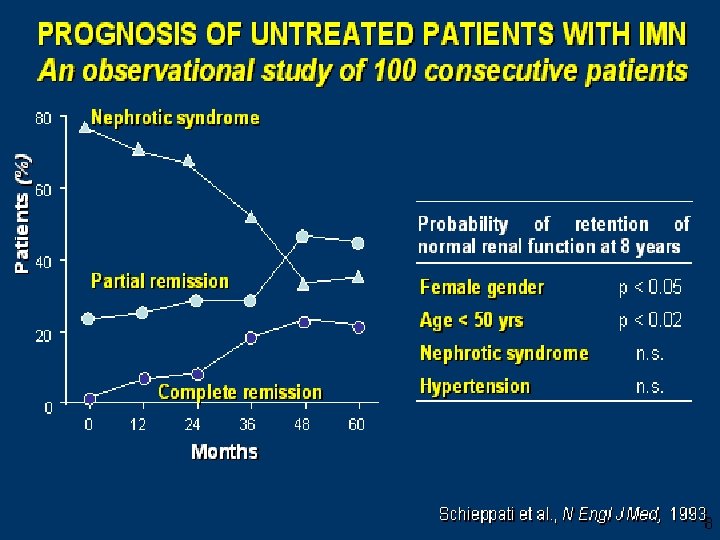

Natural History • • 30% Undergo spontaneous remission 30% Variable proteinuria with stable renal fx 30% Progress to renal failure 10% Die of non renal causes Donadio et al , KI , 33, 1988, 708 -715

Can prognostic factors assist in therapeutic decision. • • • Age Gender Pathology GFR Proteinuria Biomarkers- Urinary NAG, B 2 microglobulin and Ig. G

Gender, proteinuria, age at onset and decline of renal fx.
 69, 1641– 1648")
Troyanov et al, Kidney International (2006) 69, 1641– 1648

Probability of CR/PR according to UNAG 86% 27% Probability of renal survival acc to UNAG 0% 47% Bazzi, C. et al. Nephrol. Dial. Transplant. 2002 17: 1890 -1896; doi: 10. 1093/ndt/17. 11. 1890

B 2 microglobulin/ Ig. G as predictors of renal survival. Sn=88%, sp 91% Sn and sp 88% Branten, A. J. W. et al. J Am Soc Nephrol 2005; 16: 169 -174

Idiopathic Membranous Nephropathy Probability of Surviving Without Developing End-Stage Renal Disease According to Baseline Proteinuria Donadio et al: KI, 1988

Survival from Renal Failure in Patients with Complete, Partial, and No Remission 90% 45% 5 pt out of 348 had a creatinine clearance <15 m. L/min at initial assessment and were excluded from this analysis Troyanov et al. Kidney Int. (2004)
")
At onset Cr. Cl m. L/min Univariate Hazard ratio P value (95% CI) Multivariate Hazard ratio P value (95% CI) 0. 97 (0. 96– 0. 99) <0. 001 Proteinuria g/d 1. 07 (1. 02– 1. 13) 0. 008 Follow-up MAP Remission NR 1. 08 (1. 02– 1. 15) 0. 009 <0. 001 1 <0. 001 1 0. 08 (0. 03– 0. 19)b –b <0. 001 PR 0. 17 (0. 09– 0. 33) NR<PR<CR CR –b Troyanov et al. Kidney Int. (2004) –

Number of Partial and Complete SR and Time to Achieve Partial and Complete SR According to Baseline Proteinuria Polanco et al: J Am Soc Nephrol, 2010

Risk of Progression Categories Low risk Laboratory Normal Function Proteinuria < 4 g/d Medium risk Normal function Persistent proteinuria > 4<8 g/d High risk Abnormal function and/or Persistent proteinuria > 8 g/d Pei et al, KI 42, 960 -966, 1992 Time 6/12 <6/12
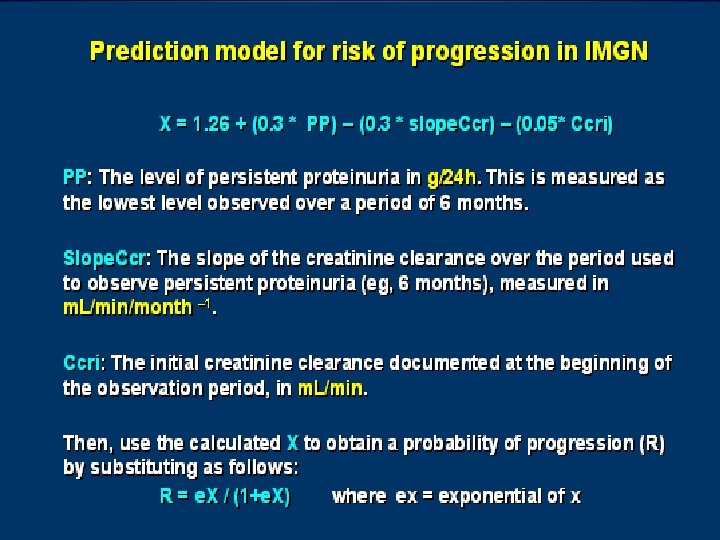
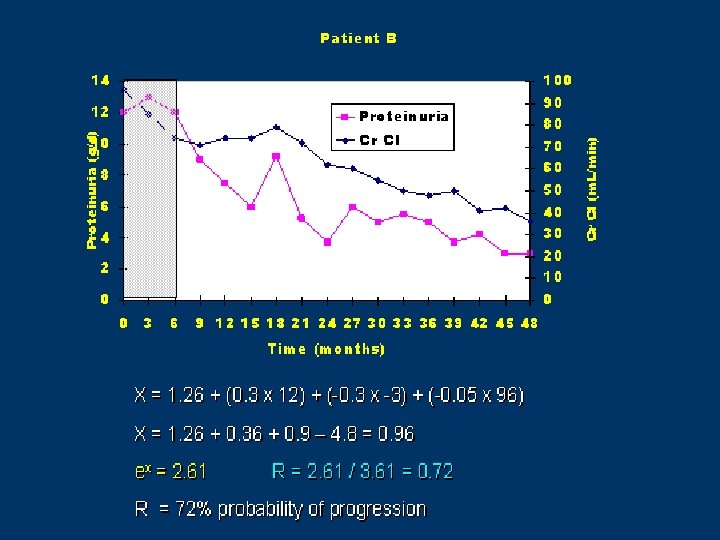

Cattran et al, KI 51, 901 -907, 1997

Goal of therapy is to reduce proteinuria and prevent progression to renal failure

Probability of SR in patients treated with ACEIs/ARBs and in patients who did not receive this treatment Polanco, N. et al. J Am Soc Nephrol 2010; 21: 697 -704

A 10 -year follow-up - Ponticelli Protocol Study Design: RCT, Pts with MN and NS, 42 pts received CB + steroids, 39 received symptomatic Rx. Outcome: Renal survival, slopes of reciprocal of creatinine, Remisssion of proteinuria RESULTS Rx arm n=39 Conservative arm N=42 p Renal Survival 92% 60% P<0. 0005 CR/PR 88% 47% P<0. 0001 Time spent without NS 58% total f/u period 22% of total P<0. 0001 1/sr cr 0. 84 0. 51 P<0. 05

A 10 -year follow-up - Renal Survival P<0. 005 Ponticelli C et al: KI 48: 1600, 1995

Characteristics of Patients at Start of Treatment with MP plus Chlorambucil or MP plus Cyclophosphamide Ponticelli et al: JASN 9: 444, 1998
 or (C) Remission Ponticelli et al: JASN 9: 444,")
Cumulative Probability of Obtaining (P) or (C) Remission Ponticelli et al: JASN 9: 444, 1998

Efficacy of chlorambucil based regimen vs steroid alone Ponticelli, C et al, N Engl J Med 1992; 327: 599
 range Gender ratio Disease")
Cytoxan in this era Characteristic No. of cases Age (yr) range Gender ratio Disease duration (mo) Serum creatinine (mg/dl) MDRD GFR (ml/min) Serum albumin (g/dl) Serum cholesterol (mg/dl) Proteinuria (g/d) Group 1 Group 2 46 37. 2 ± 12. 4 16 to 66 27: 19 11. 7 ± 6. 2 47 38. 0 ± 13. 6 18 to 64 30: 17 10. 8 ± 7. 9 1. 17 ± 0. 22 1. 21 ± 0. 31 0. 48 84 ± 22 89 ± 26 0. 32 2. 42 ± 0. 81 2. 34 ± 0. 58 306. 4 ± 88. 2 336. 7 ± 99. 6 0. 12 5. 91 ± 2. 2 6. 11 ± 2. 5 Jha, V. et al. J Am Soc Nephrol 2007; 18: 1899 -1904 P 0. 77 0. 67 0. 48 0. 68

Probability of Reaching a Remission Dialysis free survival 90% Ctx-73% 65% Supp-34% Jha et al: JASN 18: 1899, 2007 ---Group 1 placebo, --- Group 2 - Cytoxan therapy
 and (MDRD) estimated GFR (e. GFR; B) during the follow up-period Jha,")
Proteinuria (A) and (MDRD) estimated GFR (e. GFR; B) during the follow up-period Jha, V. et al. J Am Soc Nephrol 2007; 18: 1899 -1904

What about Cyclosporine ?
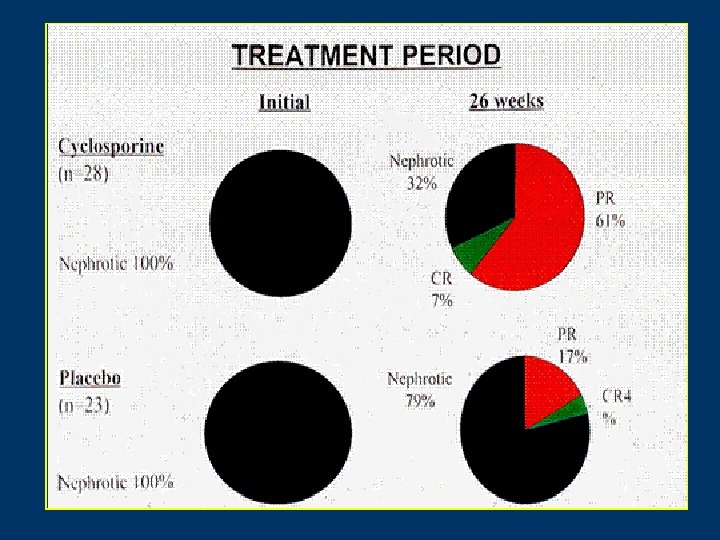
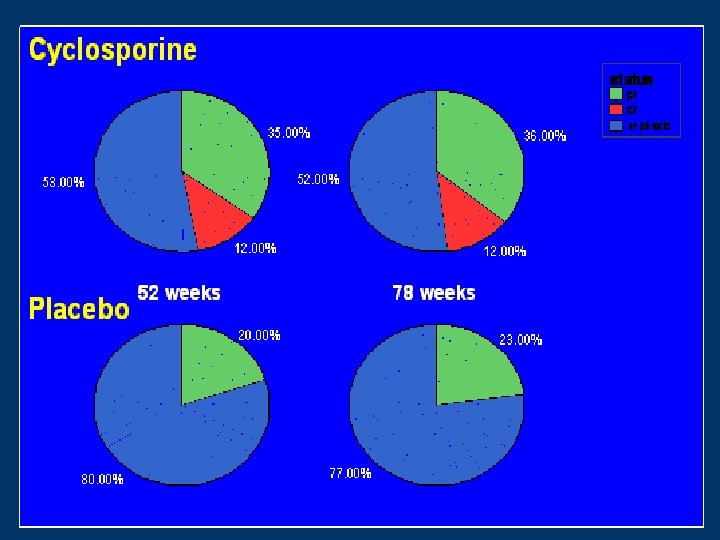

Cyclosporine in progressive membranous nephropathy

Cyclosporine • How to Use? Initial dose of 34 mg/kg. X 6 months ( bid dosing). • If no response d/c, use something else. If CR occurs stop 3 -4 months after CR. If PR ct for 12 yrs at full dose. • What to target? CR, PR, maintaining stable GFR +/- 20% of pretreatment levels and a non toxic cyclosporine level i. e C 0 level of 125 -175 or a C 2 level of 400 -600.

Tacrolimus Monotherapy Randomized Controlled Trial T = tacrolimus; C = control Praga et al: Kid Int, 2007

Tacrolimus Monotherapy Randomized Controlled Trial 56% 36% 9% 13% T = tacrolimus; C = control; numbers within columns indicate the total number of pt in CR or PR in both groups Praga et al: Kid Int, 2007

• Mean time to PR and CR in tac group was 6. 1 vs 11. 3 in the control group. • 9/19 patients (47%)who achieved CR or PR by month 18 relapsed after tac withdrawal. Time to NS relapse was 4. 2 months. • Sec endpt of 50% increase in cr: 4% tac vs 26% control. • Limitation: short f/u

Tacrolimus +steroids vs CTX + steroids • N=73, RCT, 39 Tac 0. 1 mg/kg/day X 6 months (T 0 levels 5 -10) foll by reduced dose X 3 months to keep levels 2 -5 + prednisone. • 34 pts received CTX 100 mg/day X 4 months+ prednisone • 1 yr f/u Wang et al, The American Journal of the Medical Sciences Issue: Volume 339(3), March 2010, pp 233 -238

Tacrolimus +steroids vs CTX + steroids Remission Rate was 85% in Tac arm vs 65% in CTX arm, p<0. 05 at 6 months but no change at 12 months More pts with Tac had developed glucose tolerance( 30%) Relapse rates similar 6/33 pts in the tac gp and 5/22 in CTX gp. 6 Pts had a repeat renal bx in tac gp. No pts had typical signs of CNI. Wang et al, The American Journal of the Medical Sciences Issue: Volume 339(3), March 2010, pp 233 -238 P<0. 01 Tac CTX

1 yr prospective RCT, MGN+ NS N=36 19 received MMF 2 gm/day X 12 mths, 17 conservative Rx Outcome: proteinuria, PR, CR 1 yr f/u Am J Kidney Dis 52: 699 -705

MMF as monotherapy Remission 41% 37% Dussol et al AJKD 2008

Mycophenolate Mofetil + steroids or Cyclophosphamide + steroids • Study design: 32 cases and 32 historic controls with MN and renal insufficiency ( Cr >1. 5). • Intervention: MMF 1 gm bid or CTX 1. 5 mg/kg/day X 1 yr + steroids. • Outcome: GFR, proteinuria, side effects. Median F/U 23 mths(11 -46 months).

Cumulative Incidence of Partial Remission of Proteinuria in Patients Treated with Mycophenolate Mofetil or Cyclophosphamide 72% 66% Branten et al: Am J Kidney Dis 50: 248, 2007

Cumulative Incidence of Relapses in Patients Treated with Mycophenolate Mofetil or Cyclophosphamide 55% 38% 13% Branten et al: Am J Kidney Dis 50: 248, 2007

Ruggenenti, JASN 14, 1851 -57 , 2003
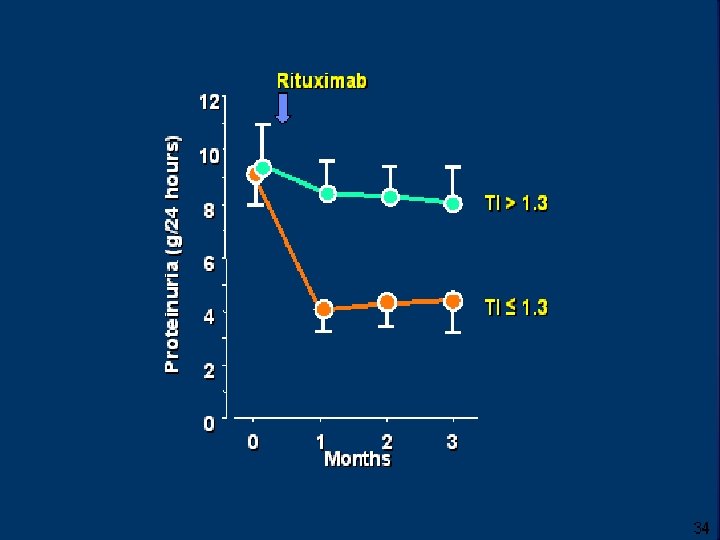

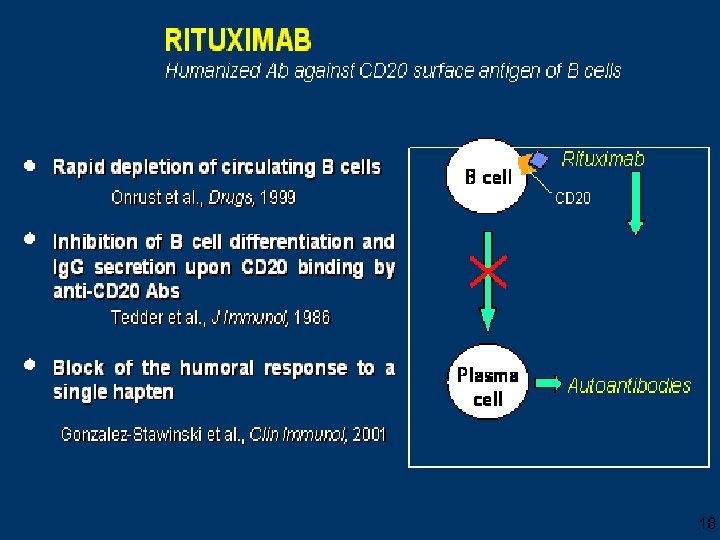
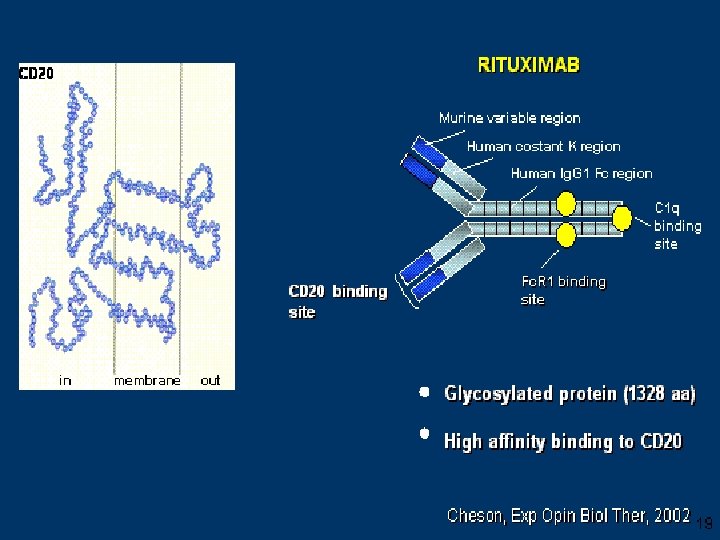
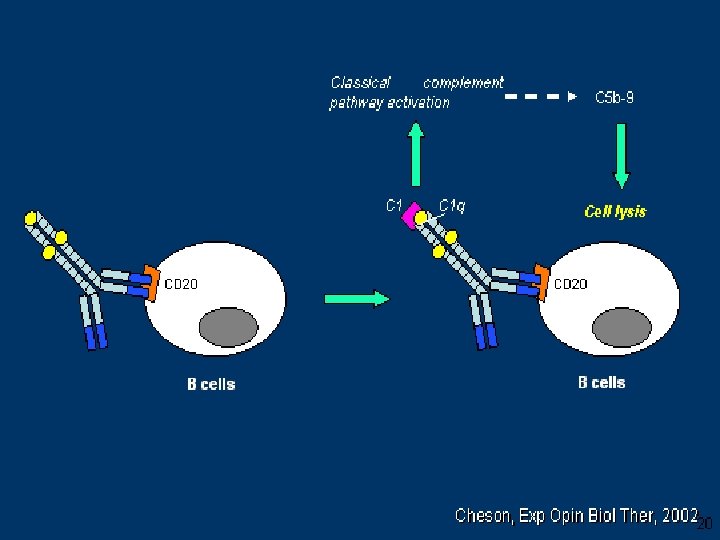
Rituximab • Open-label pilot trial n= 15 severely nephrotic patients , 7 failed other IS agents. • Rituximab was given at 0, 2 weeks and, 6 months. • At 12 mths 2/14 were in CR and 6/14 achieved PR. • Prospective identification of responsive pts not possible in their study. Fervenza et al , Kidney International (2008) 73, 117– 125
 73,")
Rituximab treatment of idiopathic membranous nephropathy Fervenza et al , Kidney International (2008) 73, 117– 125

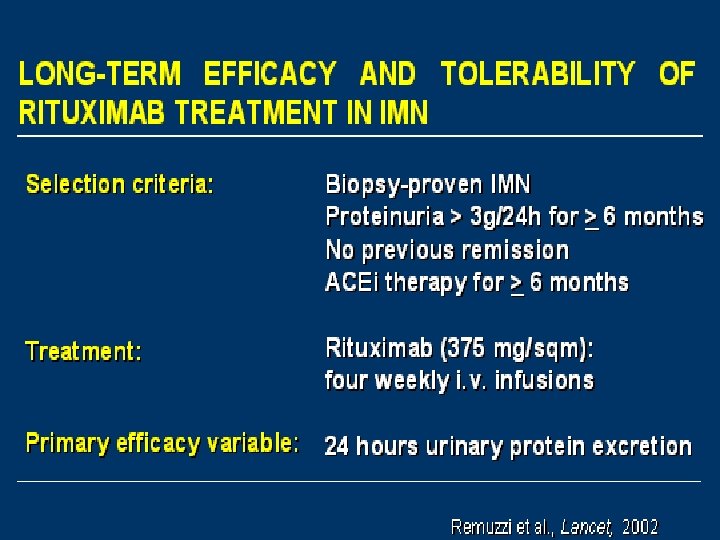
• 13 patients with normal renal fx, MGN and dependence to Cn. I were included. • Intervention: 4 weekly doses of ritux • Outcome: CR, PR 30 months after CNI withdrawal.

Clinical response not parallel with circulating CD 19 cells

A Randomized Pilot Trial Comparing Methylprednisolone Plus a Cytotoxic Agent Versus Synthetic Adrenocorticotropic Hormone in Idiopathic Membranous Nephropathy Ponticelli et al, American Journal of Kidney Diseases - 47, 2006

Prophylactic anticoagulation in MG • No RCT • Venous thromboembolic events occur in 40% of patients with membranous nephropathy and nephrotic syndrome with a serum albumin concentration of <2. 5 g/dl vs 2. 7% in those with a serum albumin concentration of >2. 5 g/dl(Bellomo et al, Nephron 63 : 249 – 254, 1993). • Severe nephrotic syndrome (serum albumin <2. 0 to 2. 5 g/dl) with other risk factors for thrombosis (e. g. , congestive heart failure; prolonged immobilization; morbid obesity; abdominal, orthopedic, or gynecologic surgery) or a family history of "thrombophilia" (who might have a genetic predisposition to thrombosis)

MGN and Transplant Recurrent 10 -45% 10 -14 months post Tx Graft loss at 10 yrs about 12. 5% Cyclosporine, MPA, steroids other immunosuppressives do not work. • Small series showing rituximab may work. ( Sprangers , CJASN, May 2010 ) • • • De-Novo 2 -6% 18 -24 months post tx Cause – Rejection -exposure of previously unseen glomerular antigenssecondary antibody response. – Glomerular injury icreases capillary wall permeability facilitating the deposition of IC – Circulating Ab directed against HLA Ag expressed on the graft. – Graft loss at 10 yrs about 40 -50% – Cyclosporine and steroids do not work. Pulse steroids do not work. Treatment is an enigma.

Current Therapies for Idiopathic Membranous Nephropathy Efficacy Safety Chlorambucil + corticosteroids Efficacy in RCT vs placebo Bone marrow suppression, seizures, malignancy, infertility Cyclophosphamide + corticosteroids Small studies suggest efficacy Leukopenia, infertility, hemorrhagic cystitis, malignancy Calcineurin inhibitors Efficacy in RCT vs placebo; frequent relapses once stopped Hypertension, hyperlipidemia, glucose intolerance, nephrotoxicity (blood levels need to be measured)
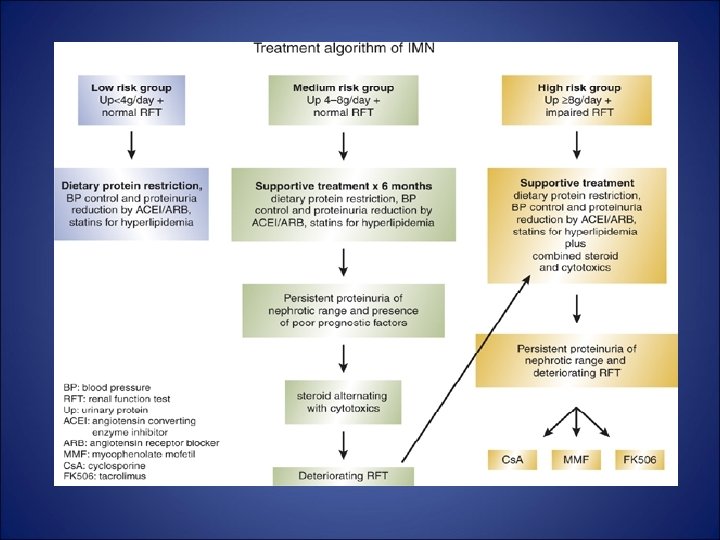

Take Home Message • Establish whether primary or secondary • If pt has normal renal fx, ct monitoring X 6 mths + ct conservative therapy. Establish progression score • If medium risk/ high risk then treat

Take Home Message • The primary regimens used to treat idiopathic MN include Cyclophosphamide or chlorambucil or CNI with glucocorticoids. • MMF + glucocorticoids, may be as effective in inducing remission of proteinuria but is associated with a high rate of relapse. No data on the long term effect of MMF on renal survival • Synthetic ACTH has been associated with complete or partial remission in a large percentage of patients in one study. No data on long-term outcomes. • Rituximab. Data mostly from case series. No data on long term outcomes.

Thankyou
a237c3d977666f130f945a4013687296.ppt