f4e44f929e343b352d642739376f6d08.ppt
- Количество слайдов: 20



Hematemesis in Blunt Trauma Diagnosis and Discussion Presenter: Paris Lovett, MD Beth Israel Medical Center, New York May 18, 2002

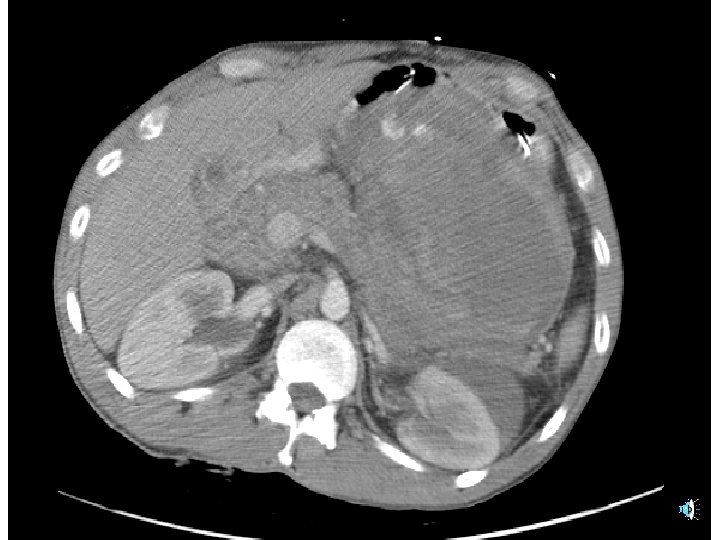
Hospital Course l l l Vitals remained stable after crystalloid and packed RBC infusions Contrast CT of the abdomen showed a heterogeneous collection in the lesser sac, consistent with a hematoma, measuring 15 x 12. 5 cm A small left perinephric hematoma was also identified



Hospital Course cont’d l l l Patient went from CT to OR EGD performed showing fresh blood in stomach, but no source and no lesions Laparotomy revealed a tense 1000 ml hematoma in a well-formed pancreatic pseudocyst, which had perforated into posterior wall of stomach Bleeding either from ruptured wall, or from pseudocyst. Hemostasis achieved with wall repair Histology benign, suggested acute traumatic rupture Discharged on day 9

Discussion l l Unfamiliar confluence of two cardinal Emergency Medicine presentations: hematemesis & blunt abdominal trauma Very few cases in the medical literature

Diagnosis suggested by: l l Monteggia Fx suggests significant mechanism Blunt abdominal trauma suggests viscus rupture as mechanism Alcohol abuse and chronicity of prior abdominal pain suggests pancreatic pathology Sudden onset massive bright hematemesis, and lack of melena, suggests acute process, temporally related to the trauma

Diagnosis suggested by cont’d: l l Vaguely located abdominal pain, and lower back pain without bruising or tenderness, suggests retroperitoneal injury Abdominal tenderness with lack of peritoneal signs, consistent with retroperitoneal injury
 (Amylase")
Diagnosis Confirmed By: l l l Coagulation studies normal (ED Ultrasound not performed) (Amylase 82; Lipase 45; available after OR) CT showed blood in lesser sac. Limits source to pancreas, spleen, kidneys, aorta, proximal small bowel, stomach EGD non-contributory (in this case) Laparotomy and histology confirmed diagnosis

Diagnostic Grid - Hematemesis Causes of Hematemesis Bl. Trauma PUD, Erosions Retroperit. Varices Mallory-Weis Malignancy Fistula Mucosal tear AVM Hemobilia Hemosuccus Pancreaticus

Diagnostic Grid – Fistula/Tear Cause Et. OH Chronic Pain Mucosal Tear Fistula Aorta Pancreas Bowel (& vessels) Spleen Kidneys

Case Reports #1 l Pancreatic pseudocyst with pseudoaneurysm 1 -13 – – – Follows chronic pancreatitis, trauma, surgery Perforation and fistula formation, most often to GI tract Bleeding spontaneous, not s/p trauma

Case Reports #2 l Traumatic aneurysms of splanchnic vessels 1, 14 -19 – – Aneurysm formation after blunt or penetrating trauma Perforation and fistula formation weeks to years after traumatic event

Case Reports #3 l Intramural and/or mesenteric hematoma of small bowel in blunt trauma 20 -24 – – – Steering-wheel, seat-belt, falls, child abuse Pain Obstruction Palpable mass Minor blood loss via Lower GI Few reports of heavy blood loss. One report of upper GI blood loss

Case Reports #4 l Mucosal tears and upper GI bleeding in blunt trauma 29 -32 – – Some have occurred through CPR 31 -32 Similar presentation, different mechanism
![References (1 -16) l l l l [1] Yeh TS, Jan YY, Jeng LB,](https://present5.com/presentation/f4e44f929e343b352d642739376f6d08/image-17.jpg "References (1 -16) l l l l [1] Yeh TS, Jan YY, Jeng LB,")
References (1 -16) l l l l [1] Yeh TS, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen MF, Massive extra-enteric gastrointestinal hemorrhage secondary to splanchnic artery aneurysms, Hepato-Gastroenterology. 1997; 44(16): 1152 -6. [2] Stanley JC, Frey CF, Miller TA, Lindenauer SM. Child CG 3 rd, Major arterial hemorrhage: a complication of pancreatic pseudocysts and chronic pancreatitis. Archives of Surgery, 1976; 111(4): 435 -40. [3] Santos JC Jr, Feres O, Rocha JJ, Aracava MM. Massive lower gastrointestinal hemorrhage caused by pseudocyst of the pancreas ruptured into the colon, Report of two cases, Diseases of the Colon & Rectum. 1992; 35(1): 75 -? ? ? [4] Zanen AL, van Vliet AC, Beukers R. Pancreatic pseudocyst as a cause of upper gastrointestinal bleeding. Netherlands Journal of Medicine. 1995; 46(2): 904. [5] Nogara MA, Cesar AM, Kanegusuku J, Lopes RW. [Upper gastrointestinal hemorrhage associated with chronic pancreatitis and pseudocyst: report of a case. ] Arquivos de Gastroenterologia. 1993; 30(1): 33 -7. [6] Nishida K, Terai Y, Nojiri I, Kato M, Higashijima M, Takagi K, Adashi R. [A case of pancreatic pseudocyst with intracystic hemorrhage and repeated gastrointestinal bleeding]. Nippon Ronen Igakkai Zasshi - Japanese Journal of Geriatrics. 1993; 30(8): 714 -9. [7] von Flue M, Kocher T, Herzog U, Looser C, Schuppisser JP. [Hemorrhage from pseudocysts caused by pseudoaneurysms in chronic pancreatitis. Diagnosis and management]. Helvetica Chirurgica Acta. 1993; 59(5 -6): 785 -9. [8] Takeuchi H. Konaga E. Tanemoto K. Gotoh K. Murata K. Murakami I. A case of chronic pancreatitis with pseudoaneurysm rupturing into a pseudocyst. [Journal Article] Acta Medica Okayama. 47(1): 59 -62, 1993 Feb. [9] Fernandez-Cruz L. Pera M. Vilella A. Llovera JM. Navasa M. Teres J. Hemosuccus pancreaticus from a pseudoaneurysm of the hepatic artery proper in a patient with a pancreatic pseudocyst. [Journal Article] Hepato-Gastroenterology. 39(2): 149 -51, 1992 [10] Muckart DJ, Bade P. Pancreatic pseudocyst haemorrhage presenting as a bleeding duodenal ulcer. Postgraduate Medical Journal. 1989; 65(768): 748 -9. [11] Bergamini G, Repaci G, Bertoncini M, Garbini A, Nanni G, Bragherio G. [Exsanguinating hemorrhage caused by perforation of a pseudocyst of the tail of the pancreas in the transverse colon. ] Minerva Chirurgica. 1985; 40(20): 1411 -4. [12] Kiviluoto T, Schroder T, Kivilaakso E, Lempinen M. Acute haemorrhage associated with pancreatic pseudocyst and chronic pancreatitis. Annales Chirurgiae et Gynaecologiae. 1984; 73(4): 214 -8. [13] Cahow CE, Gusberg RJ, Gottlieb LJ. Gastrointestinal hemorrhage from pseudoaneurysms in pancreatic pseudocysts. American Journal of Surgery. 1983; 145(4): 534 -41. [14] Hassantash SA. Mock C. Maier RV. Traumatic visceral artery aneurysm: presentation as massive hemorrhage from perforation into an adjacent hollow viscus. [Journal Article] Journal of Trauma-Injury Infection & Critical Care. 38(3): 357 -60, 1995 [15] Kestenberg WL, Mittal VK. Post-traumatic pseudoaneurysm of the left hepatic artery initially appearing as upper gastrointestinal hemorrhage secondary to hepatic artery-duodenal fistula, a case study. American Surgeon. 1992; 58(8): 451 -4. [16] Taylor DW Jr, , Babchuk WI, Walz DJ, Vemuri BR, Gastrointestinal hemorrhage from fistula between traumatic pseudoaneurysm of the right hepatic artery and the duodenum, Clinical Nuclear Medicine. 1988; 13(5): 337 -8.
![References (17 -32) l l l l [17] Gow KW, Murphy JJ 3 rd,](https://present5.com/presentation/f4e44f929e343b352d642739376f6d08/image-18.jpg "References (17 -32) l l l l [17] Gow KW, Murphy JJ 3 rd,")
References (17 -32) l l l l [17] Gow KW, Murphy JJ 3 rd, Blair GK, Stringer DA, Culham JA, Fraser GC. Splanchnic artery pseudo-aneurysms secondary to blunt abdominal trauma in children. Journal of Pediatric Surgery. 1996; 31(6): 812 -5. [18] Maloney RD, Nealon TF Jr, Roberts EA. Massive bleeding from a ruptured superior mesenteric artery aneurysm duodenum. Archives of Surgery, 1976; 111(3): 286 -8. [19] Bleichrodt RP, Smulders TA, Schreuder F, Tinbergen W, Muller WF. Aneurysms of the jejunal artery, Journal of Cardiovascular Surgery. 1984; 25(4): 376 -7. [20] Lotti R, Gaetano Perri S, Gola P, Leardi S, Cianca G, Citone G. [An intramural hematoma of the duodenum. ] Annali Italiani di Chirurgia. 2000; 71(4): 519 -23. [21] Kleinman PK, Brill PW, Winchester P. Resolving duodenal-jejunal hematoma in abused children. Radiology. 1986; 160(3): 747 -50. [22] Sidhu MK, Weinberger E, Healey P. Intramural duodenal hematoma after blunt abdominal trauma, AJR, American Journal of Roentgenology. 1998; 170(1): 38. [23] Voss M, Bass DH, Traumatic duodenal haematoma in children. Injury. 1994; 25(4): 227 -30. [24] Zapf S, Duber C, Kuhn FP, Lauff V. [Diagnosis of duodenal wall hematoma. ] Rontgen-Blatter. 1988; 41(1): 27 -30. [25] Moore JB, Moore EE, Lower gastrointestinal bleeding: an unusual presentation for blunt abdominal trauma, Journal of Trauma-Injury Infection & Critical Care. 1977; 17(12): 961 -3. [26] Johansson L, Jonsson A, Norrby K, Lennquist S. Intestinal intramural haemorrhage after blunt abdominal trauma, Acta Chirurgica Scandinavica. 1984; 150(2): 165 -71. [27] Johansson L, Norrby K, Nystrom PO, Lennquist S. Intestinal intramural haemorrhage after abdominal missile trauma--clinical classification and prognosis, Acta Chirurgica Scandinavica. 1984; 150(1): 51 -6. [28] Birns MT, Katon RM, Keller F. Intramural hematoma of the small intestine presenting with major upper gastrointestinal hemorrhage, Case report and review of the literature. Gastroenterology. 1979; 77(5): 1094 -100 [29] Kushimoto S, Mun M, Yamamoto Y, Harada N, Sato N, Koido Y, Journal of Trauma-Injury Infection & Critical Care. 2001; 51(3): 591 -3. [30] Mc. Boyle MF, Schiller WR, Hurt AV, Massive gastrointestinal bleeding following blunt abdominal trauma: an unusual case presentation, Journal of Trauma-Injury Infection & Critical Care, 1984; 24(12): 1057 -9. [31] Register SD, Downs JB, Tabeling BB. Gastric mucosal lacerations: a complication of cardiopulmonary resuscitation. Anesthesiology. 1985; 62(4): 513 -4. [32] Mc. Donnell PJ, Hutchins GM, Hruban RH, Brown CG. Hemorrhage from gastric mucosal tears complicating cardiopulmonary resuscitation. Annals of Emergency Medicine. 1984 13(4): 230 -3.

Summary l l Pancreatic pseudocyst + traumatic rupture to stomach + major upper GI bleed = unique in literature Unfamiliar paring of very familiar presentations Some similar or contiguous case reports Set of clinical elements pointing the way to diagnosis

José Guadalupe Posada Mexican Engraver 1852 -1913
f4e44f929e343b352d642739376f6d08.ppt