

b9f22b3913ecd5b9db236d35279a10c6.ppt
- Количество слайдов: 64
 Heart Failure Improvement Across the Continuum Hospital to Home: Optimizing the Transition January 2009 Florida Hospital Assoc. Peg M. Bradke, RN, MA Director, Heart Care Services St. Luke’s Hospital, Cedar Rapids, Iowa
Heart Failure Improvement Across the Continuum Hospital to Home: Optimizing the Transition January 2009 Florida Hospital Assoc. Peg M. Bradke, RN, MA Director, Heart Care Services St. Luke’s Hospital, Cedar Rapids, Iowa
 February 2006 l l St. Luke’s joined the Institute for Health Improvement Innovation Project for Transitions to Home. Work concentrated on the Heart Failure patient.
February 2006 l l St. Luke’s joined the Institute for Health Improvement Innovation Project for Transitions to Home. Work concentrated on the Heart Failure patient.
 Strategies in Place l l l l Heart Failure work team in place Congestive Heart Failure class Utilizing BNP to identify HF patients Follow-up phone calls Setting up discharge appointments Pad/pencil at bedside for patient A lot of work on CMS indicators
Strategies in Place l l l l Heart Failure work team in place Congestive Heart Failure class Utilizing BNP to identify HF patients Follow-up phone calls Setting up discharge appointments Pad/pencil at bedside for patient A lot of work on CMS indicators
 First Steps l Heart Failure Work Group reorganized to include: l l Home Care representative Family member of a HF patient Long-Term Care representative Physician Clinic representative These views added new context to our efforts.
First Steps l Heart Failure Work Group reorganized to include: l l Home Care representative Family member of a HF patient Long-Term Care representative Physician Clinic representative These views added new context to our efforts.
 Measurement How will we know a change is improvement? HF 30 -day readmission rate: (Unit of focus or hospital-wide) l HF is primary, secondary or lower level diagnosis l Patient with HF had a readmission for HF within 30 days of a readmission for HF l Use your own definition or CHF Toolkit measures at www. IHI. org http: //www. ihi. org/NR/rdonlyres/708 DEB 58 -6082 -453 A-B 26 A 3391290 EC 0 AD/0/MIFCHFPercentof. Congestive. Heart. Failure. Patient. Dischargeswith. Readmission. Within 30 D ays. doc Hospital 30 -day (all) readmission rate: l Patient with HF was readmitted for any reason For both measures: l l l Exclude chemo day patients treated on the unit If focusing your work on a single unit, the HF readmission or all readmission rates for that unit will be needed Display monthly on a line (run) chart for last twelve months.
Measurement How will we know a change is improvement? HF 30 -day readmission rate: (Unit of focus or hospital-wide) l HF is primary, secondary or lower level diagnosis l Patient with HF had a readmission for HF within 30 days of a readmission for HF l Use your own definition or CHF Toolkit measures at www. IHI. org http: //www. ihi. org/NR/rdonlyres/708 DEB 58 -6082 -453 A-B 26 A 3391290 EC 0 AD/0/MIFCHFPercentof. Congestive. Heart. Failure. Patient. Dischargeswith. Readmission. Within 30 D ays. doc Hospital 30 -day (all) readmission rate: l Patient with HF was readmitted for any reason For both measures: l l l Exclude chemo day patients treated on the unit If focusing your work on a single unit, the HF readmission or all readmission rates for that unit will be needed Display monthly on a line (run) chart for last twelve months.
 l l") AIM Statement (From February 2006 Initial Transition to Home IHI Kick-off Meeting) l l By January 1, 2007, St. Luke’s Hospital’s Telemetry Unit and Medical Unit will reduce unplanned readmissions by 50% (from 12 to 6%) by improving the transition home process for all Heart Failure patients. Our methodology will include the patient and caregiver - ensuring that they fully understand their diagnosis, plan of care and follow-up care with physician.
AIM Statement (From February 2006 Initial Transition to Home IHI Kick-off Meeting) l l By January 1, 2007, St. Luke’s Hospital’s Telemetry Unit and Medical Unit will reduce unplanned readmissions by 50% (from 12 to 6%) by improving the transition home process for all Heart Failure patients. Our methodology will include the patient and caregiver - ensuring that they fully understand their diagnosis, plan of care and follow-up care with physician.
 What Changes Can We Make That Will Result in Improvement? l Four Key Changes to Achieve an Ideal Care Transition from Hospital to Home: 1. Enhanced Assessment of Patients 2. Enhanced Teaching and Learning 3. Patient-Centered Communication Handoffs 4. Post Hospital Follow-up
What Changes Can We Make That Will Result in Improvement? l Four Key Changes to Achieve an Ideal Care Transition from Hospital to Home: 1. Enhanced Assessment of Patients 2. Enhanced Teaching and Learning 3. Patient-Centered Communication Handoffs 4. Post Hospital Follow-up
 Result of the IHI Collaborative Work on Transitions l Transforming Care at the Bedside How-to Guide http: //www. ihi. org/NR/rdonlyres/8 F 0551 D 1 -DCD 7 -4 EE 7 -BEE 07 C 0 DFBB 5 F 6 AB/5867/Transitions. Home_Howto. Guide_Final 102207. pdf
Result of the IHI Collaborative Work on Transitions l Transforming Care at the Bedside How-to Guide http: //www. ihi. org/NR/rdonlyres/8 F 0551 D 1 -DCD 7 -4 EE 7 -BEE 07 C 0 DFBB 5 F 6 AB/5867/Transitions. Home_Howto. Guide_Final 102207. pdf
 Enhancing the Admission Assessment for Post. Discharge Needs
Enhancing the Admission Assessment for Post. Discharge Needs
 Enhanced Admission Assessment for Post Discharge Needs l l l Identify the appropriate family caregivers Partner with home care agencies, primary care offices and clinics, and long-term care facilities Communicate to all members of the care team the discharge plan and what needs to happen Estimate the home-going date on admission and anticipate needs Estimate standard discharge criteria
Enhanced Admission Assessment for Post Discharge Needs l l l Identify the appropriate family caregivers Partner with home care agencies, primary care offices and clinics, and long-term care facilities Communicate to all members of the care team the discharge plan and what needs to happen Estimate the home-going date on admission and anticipate needs Estimate standard discharge criteria
 Heart Failure Work Group Reorganized to Include: Home Care representative l Family member of a HF patient l Long-Term Care representative l Physician Clinic representative l These views added new context to our efforts.
Heart Failure Work Group Reorganized to Include: Home Care representative l Family member of a HF patient l Long-Term Care representative l Physician Clinic representative l These views added new context to our efforts.
 Sample of White Board
Sample of White Board
 Sample of SBAR Kardex
Sample of SBAR Kardex
 Communication l l l Daily discharge huddle at 10: 00 AM Bedside reporting Both opportunities to review plan for day and anticipate discharge needs
Communication l l l Daily discharge huddle at 10: 00 AM Bedside reporting Both opportunities to review plan for day and anticipate discharge needs
 Reconcile Medications Upon Admission l l l Involve the patient and family caregivers, care providers, physicians, pharmacy Reconcile on admission (suitably trained professional) Include record of the reconciliation in the medical record Ensure drug changes during the admission are reconciled, updated, accurate and timely Consider using a personalized medication
Reconcile Medications Upon Admission l l l Involve the patient and family caregivers, care providers, physicians, pharmacy Reconcile on admission (suitably trained professional) Include record of the reconciliation in the medical record Ensure drug changes during the admission are reconciled, updated, accurate and timely Consider using a personalized medication
 for readmission. What did the patient or") Chart Review Tool l l Known reason(s) for readmission. What did the patient or family think contributed to the readmission? Any self-care instructions misunderstood? Evidence of teach back documented? What did the physician or office staff think contributed? Was a follow-up physician visit scheduled? Attended? Number of days between the discharge and physician’s office visit. Number of days between discharge and readmission Any urgent clinic/ED visits before readmission? Functional status of the patient on discharge? Clear discharge plan documented?
Chart Review Tool l l Known reason(s) for readmission. What did the patient or family think contributed to the readmission? Any self-care instructions misunderstood? Evidence of teach back documented? What did the physician or office staff think contributed? Was a follow-up physician visit scheduled? Attended? Number of days between the discharge and physician’s office visit. Number of days between discharge and readmission Any urgent clinic/ED visits before readmission? Functional status of the patient on discharge? Clear discharge plan documented?
 Interview Questions Asked to Patients/ Caregiver Readmitted With Heart Failure l l l Can you tell me in your own words why you think you ended up sick enough to be readmitted again? Can you tell me what a typical meal has been for you since you left the hospital? What did you have for dinner last night? Where are your scale and calendar located? Have you seen your doctor since you were discharged from the hospital? Do you have all of your medications? How do you set your pills up every day? Were there any appointments that kept you from taking any of your pills?
Interview Questions Asked to Patients/ Caregiver Readmitted With Heart Failure l l l Can you tell me in your own words why you think you ended up sick enough to be readmitted again? Can you tell me what a typical meal has been for you since you left the hospital? What did you have for dinner last night? Where are your scale and calendar located? Have you seen your doctor since you were discharged from the hospital? Do you have all of your medications? How do you set your pills up every day? Were there any appointments that kept you from taking any of your pills?
 Enhancing Understanding in the Patient Education Process
Enhancing Understanding in the Patient Education Process
 Enhanced Understanding in the Patient Education Process l Redesign the patient education process to improve patient/family or caregiver understanding of self care: l l l Identify the appropriate family or caregivers Involve right learners in all critical education Identify how the patient and family or caregiver learn best Redesign written material Redesign teaching methods
Enhanced Understanding in the Patient Education Process l Redesign the patient education process to improve patient/family or caregiver understanding of self care: l l l Identify the appropriate family or caregivers Involve right learners in all critical education Identify how the patient and family or caregiver learn best Redesign written material Redesign teaching methods
 Enhanced Teaching and Learning Redesign patient teaching material: l During acute care hospitalizations for HF, only essential education is recommended • Reinforce within 1 -2 weeks after discharge • Continue for 3 -6 months Adams, KF et al: HFSA 2006 Comprehensive Heart Failure Practice Guideline. Journal of Cardiac Failure Vol. 12, No. 1, pg 61 February 2006
Enhanced Teaching and Learning Redesign patient teaching material: l During acute care hospitalizations for HF, only essential education is recommended • Reinforce within 1 -2 weeks after discharge • Continue for 3 -6 months Adams, KF et al: HFSA 2006 Comprehensive Heart Failure Practice Guideline. Journal of Cardiac Failure Vol. 12, No. 1, pg 61 February 2006
 Intervention: Patient Education Material Key “small tests of change”” l Reviewed content of educational materials utilizing health literacy concepts. l Outpatient Heart Failure class utilized as focus group for content. l Family member on team, along with her siblings, reviewed content for understanding Health Literacy.
Intervention: Patient Education Material Key “small tests of change”” l Reviewed content of educational materials utilizing health literacy concepts. l Outpatient Heart Failure class utilized as focus group for content. l Family member on team, along with her siblings, reviewed content for understanding Health Literacy.
 Keys to Success Utilizing Health Care Literacy Concepts l l l On all written materials, matched terminology to what we said in class. Used term Heart Failure as opposed to Congestive Heart Failure or Chronic HF Removed ranges Increased font size Added more white space
Keys to Success Utilizing Health Care Literacy Concepts l l l On all written materials, matched terminology to what we said in class. Used term Heart Failure as opposed to Congestive Heart Failure or Chronic HF Removed ranges Increased font size Added more white space
 Keys to Success with Health Literacy l Use universal health literacy communications principles to redesign written teaching materials: User-friendly written materials use: • Simple words (1 -2 syllables) • • • Short sentences (4 -6 words) Short paragraphs (2 -3 sentences) No medical jargon Headings and bullets Highlighted or circled key information
Keys to Success with Health Literacy l Use universal health literacy communications principles to redesign written teaching materials: User-friendly written materials use: • Simple words (1 -2 syllables) • • • Short sentences (4 -6 words) Short paragraphs (2 -3 sentences) No medical jargon Headings and bullets Highlighted or circled key information
 Heart Failure Magnet
Heart Failure Magnet
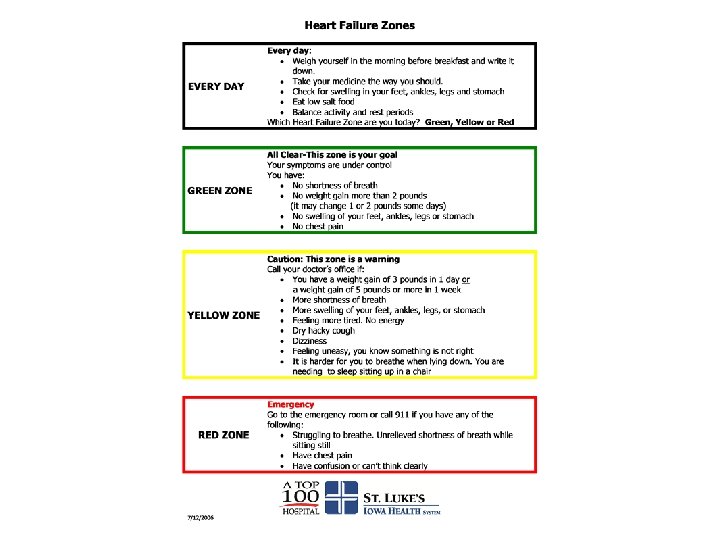
 Warning Signs and Symptoms
Warning Signs and Symptoms
 Heart Failure Handout
Heart Failure Handout
 Diet Information
Diet Information
 On-Line Discharge Instruction
On-Line Discharge Instruction
 Evaluation of New Patient Education Material Results from 15 follow-up phone calls: l “Information very helpful. ” l Able to state where information was and reported that they were referring to it. l Understood content. l Successfully answered teach back questions related to “water pill, ” diet and weight. l Improvement opportunity – patients were often unclear when they had multiple physicians which one to call for the symptoms (magnet revised).
Evaluation of New Patient Education Material Results from 15 follow-up phone calls: l “Information very helpful. ” l Able to state where information was and reported that they were referring to it. l Understood content. l Successfully answered teach back questions related to “water pill, ” diet and weight. l Improvement opportunity – patients were often unclear when they had multiple physicians which one to call for the symptoms (magnet revised).
 Enhanced Teaching and Learning Redesign patient teaching: l Stop and check for understanding using Teach Back after teaching each segment of the information l If there is a gap, review again l Another way to close the loop
Enhanced Teaching and Learning Redesign patient teaching: l Stop and check for understanding using Teach Back after teaching each segment of the information l If there is a gap, review again l Another way to close the loop
 Redesign Patient Teaching l l l Slow down when speaking to the patient and family and break messages into short statements Use plain language, breaking content into short statements Segment education to allow for mastery
Redesign Patient Teaching l l l Slow down when speaking to the patient and family and break messages into short statements Use plain language, breaking content into short statements Segment education to allow for mastery
 Enhanced Teaching and Learning Utilizing “Teach Back” l Explain needed information to the patient or family caregiver. l Ask in a non-shaming way for the individual to explain in his or her own words what was understood. l Example: “I want to be sure that I did a good job of teaching you today about how to stay safe after you go home. Could you please tell me in your own words the reasons you should call the doctor? ” l Return demonstration or show back
Enhanced Teaching and Learning Utilizing “Teach Back” l Explain needed information to the patient or family caregiver. l Ask in a non-shaming way for the individual to explain in his or her own words what was understood. l Example: “I want to be sure that I did a good job of teaching you today about how to stay safe after you go home. Could you please tell me in your own words the reasons you should call the doctor? ” l Return demonstration or show back
 Teach Back Questions l l What is the name of your water pill? What weight gain should you report to your doctor? What foods should you avoid? Do you know what symptoms to report to your doctor?
Teach Back Questions l l What is the name of your water pill? What weight gain should you report to your doctor? What foods should you avoid? Do you know what symptoms to report to your doctor?
 Enhanced Teaching and Learning l Use Teach Back daily l l In the hospital During home visits and follow-up phone calls To assess the patients’ and family caregivers’ understanding of discharge instructions and ability to do self-care To close understanding gaps between: l l Caregivers and patients Professional caregivers and family caregivers
Enhanced Teaching and Learning l Use Teach Back daily l l In the hospital During home visits and follow-up phone calls To assess the patients’ and family caregivers’ understanding of discharge instructions and ability to do self-care To close understanding gaps between: l l Caregivers and patients Professional caregivers and family caregivers
 Teach Back Success l l l Percent of time patients can teach back 90% or more of content taught related to the transition to home utilizing the four questions related to self management of heart failure Stop and check for understanding using Teach Back after teaching each segment of information Assess patient’s, family’s or caregiver’s ability and confidence
Teach Back Success l l l Percent of time patients can teach back 90% or more of content taught related to the transition to home utilizing the four questions related to self management of heart failure Stop and check for understanding using Teach Back after teaching each segment of information Assess patient’s, family’s or caregiver’s ability and confidence
 Improving Teach Back Results
Improving Teach Back Results
 Staff Competency Validation for Teachback l Methodology l The learning station will use discussion, role playing and patient teaching scenarios to help RN’s communicate effectively to patient/family.
Staff Competency Validation for Teachback l Methodology l The learning station will use discussion, role playing and patient teaching scenarios to help RN’s communicate effectively to patient/family.
 Staff Competency Validation for Teachback l Objectives – Each participant will be able to: 1. Define health literacy 2. Learn clear communication strategies 3. Define plain language 4. Learn and utilize the “teach back” method in a shame-free way
Staff Competency Validation for Teachback l Objectives – Each participant will be able to: 1. Define health literacy 2. Learn clear communication strategies 3. Define plain language 4. Learn and utilize the “teach back” method in a shame-free way
 Staff Competency Validation for Teachback l Each participant will participate in a role-play providing education to a patient. The following will be assessed: l l l Ability to do teach back in a shame-free way; tone is positive Utilizes plain language for explanations Does not ask patient, “Do you understand? ” Uses statements such as “I want to make sure I explained everything clearly to you. ” “Can you please explain it back to me in your own words? ” Or, as an example, “I want to make sure I did a good job explaining this to you because it can be very confusing. Can you tell me what changes we decided to make and how you will take your medicine now? ” If needed, participant will clarify and reinforce the explanation to improve patient understanding.
Staff Competency Validation for Teachback l Each participant will participate in a role-play providing education to a patient. The following will be assessed: l l l Ability to do teach back in a shame-free way; tone is positive Utilizes plain language for explanations Does not ask patient, “Do you understand? ” Uses statements such as “I want to make sure I explained everything clearly to you. ” “Can you please explain it back to me in your own words? ” Or, as an example, “I want to make sure I did a good job explaining this to you because it can be very confusing. Can you tell me what changes we decided to make and how you will take your medicine now? ” If needed, participant will clarify and reinforce the explanation to improve patient understanding.
 Patient and Family Centered Transition Communication
Patient and Family Centered Transition Communication
 Patient-Centered Transition Communication l l l l Provide next caregiver customized real-time information: l What to expect at home l Easy to read self-care instructions l Reasons to call for help l Number to call for emergent and non-emergent needs and questions Share patient education materials and education processes across all care settings Physicians, home care and other involved clinicians transmit information at time of discharge Include anticipated, important next steps in the transition, including concerns about the patients Ask receiving care teams for their preferred format, mode of communication and specific information needs about the patient’s functional status Continually improve by aggregating the experience of patients, families, and caregivers and designing improvements
Patient-Centered Transition Communication l l l l Provide next caregiver customized real-time information: l What to expect at home l Easy to read self-care instructions l Reasons to call for help l Number to call for emergent and non-emergent needs and questions Share patient education materials and education processes across all care settings Physicians, home care and other involved clinicians transmit information at time of discharge Include anticipated, important next steps in the transition, including concerns about the patients Ask receiving care teams for their preferred format, mode of communication and specific information needs about the patient’s functional status Continually improve by aggregating the experience of patients, families, and caregivers and designing improvements
 Example of Class Calendar
Example of Class Calendar
 St. Luke’s Heart Failure Continuum l l l l Teach back in hospital using new teaching material Standardized HF on-line discharge instructions Home Care complimentary visit 24 to 48 hours post discharge – use teach back again Physician office visit within three to five days Advance Practice Nurse follow-up phone call on seventh day post discharge – teach back repeated Outpatient Heart Failure class – seeing increased participation Collaboration with cardiology office Heart Failure Clinic
St. Luke’s Heart Failure Continuum l l l l Teach back in hospital using new teaching material Standardized HF on-line discharge instructions Home Care complimentary visit 24 to 48 hours post discharge – use teach back again Physician office visit within three to five days Advance Practice Nurse follow-up phone call on seventh day post discharge – teach back repeated Outpatient Heart Failure class – seeing increased participation Collaboration with cardiology office Heart Failure Clinic
 Post Acute Care Follow-Up
Post Acute Care Follow-Up
 Post Acute Care Follow-Up l l High risk patients: prior to discharge, schedule a face-to-face follow-up visit (home care visit, care coordination visit, or physician office visit) to occur within 48 hours after discharge Moderate risk patients: prior to discharge, schedule follow-up phone call within 48 hours and schedule a physician office visit within five days
Post Acute Care Follow-Up l l High risk patients: prior to discharge, schedule a face-to-face follow-up visit (home care visit, care coordination visit, or physician office visit) to occur within 48 hours after discharge Moderate risk patients: prior to discharge, schedule follow-up phone call within 48 hours and schedule a physician office visit within five days
 Post Acute Care Follow-Up High-risk patients: l Patient has been admitted two or more times in the past year l Patient failed “Teach Back” or the patient or family caregiver has low degree of confidence to carry out self-care at home l l Patient and family caregiver have the phone number for questions and concerns Consider home care or discharge coach
Post Acute Care Follow-Up High-risk patients: l Patient has been admitted two or more times in the past year l Patient failed “Teach Back” or the patient or family caregiver has low degree of confidence to carry out self-care at home l l Patient and family caregiver have the phone number for questions and concerns Consider home care or discharge coach
 Post Acute Care Follow-Up Moderate risk patients: l l Patient has been admitted once in the past year Patient or family caregiver has moderate degree of confidence to carry out self-care at home l l Prior to discharge, schedule follow-up phone call within 48 hours Schedule a physician office visit within five days
Post Acute Care Follow-Up Moderate risk patients: l l Patient has been admitted once in the past year Patient or family caregiver has moderate degree of confidence to carry out self-care at home l l Prior to discharge, schedule follow-up phone call within 48 hours Schedule a physician office visit within five days
 Intervention: Home Care Visit 24 -48 Hours Post Discharge l l Small test of change October 2006 Education to all Home Care staff Visit 48 hours after discharge Visit outline l Medication Reconciliation l Review of diet and foods in-house l Teach back on water pill, diet and weight l Vital signs Hardwired process in January 2007
Intervention: Home Care Visit 24 -48 Hours Post Discharge l l Small test of change October 2006 Education to all Home Care staff Visit 48 hours after discharge Visit outline l Medication Reconciliation l Review of diet and foods in-house l Teach back on water pill, diet and weight l Vital signs Hardwired process in January 2007
 Cost for Heart Failure Program l Home Care visit: $110. 00 l l l St. Luke’s covers $58. 00; the remainder of $52. 00 is absorbed Follow-up phone calls: $10, 000 Education material l l Magnet: $1. 00 Total with handouts: $1, 200
Cost for Heart Failure Program l Home Care visit: $110. 00 l l l St. Luke’s covers $58. 00; the remainder of $52. 00 is absorbed Follow-up phone calls: $10, 000 Education material l l Magnet: $1. 00 Total with handouts: $1, 200
 Intervention: Nursing Home l l l Patient education sent with all nursing home patients at discharge. Educational offerings for the staff conducted in the nursing homes. Nursing home representative added to our HF Team.
Intervention: Nursing Home l l l Patient education sent with all nursing home patients at discharge. Educational offerings for the staff conducted in the nursing homes. Nursing home representative added to our HF Team.
 Intervention: Follow-Up Phone Call l l Advance Practice Nurse makes follow-up phone call at seven days post-discharge Standardize questions Results monitored and changes made as needed based on feedback Results monitored globally and per individual unit
Intervention: Follow-Up Phone Call l l Advance Practice Nurse makes follow-up phone call at seven days post-discharge Standardize questions Results monitored and changes made as needed based on feedback Results monitored globally and per individual unit
 Intervention: Primary Care Follow-Up Appointment l l Worked with Primary Care to assure followup visits scheduled 3 to 5 days post discharge Particularly on high-risk patient for readmission
Intervention: Primary Care Follow-Up Appointment l l Worked with Primary Care to assure followup visits scheduled 3 to 5 days post discharge Particularly on high-risk patient for readmission
 Intervention: Dietitian Visits l Now mandatory on all HF patients
Intervention: Dietitian Visits l Now mandatory on all HF patients
") Discharge Status (Nov 07 -Oct 08)
Discharge Status (Nov 07 -Oct 08)
") Attending MD During Hospitalization (Nov 07 -Oct 08)
Attending MD During Hospitalization (Nov 07 -Oct 08)
 Patient Satisfaction on Discharge Hand-Off
Patient Satisfaction on Discharge Hand-Off
 Heart Failure Readmission Rates* Good Aug 06 = Implemented use of new patient education materials Jan 07 = Initiated complimentary visits *Percent of heart failure patients readmitted for exacerbation of their heart failure.
Heart Failure Readmission Rates* Good Aug 06 = Implemented use of new patient education materials Jan 07 = Initiated complimentary visits *Percent of heart failure patients readmitted for exacerbation of their heart failure.
 Example of Data Collection
Example of Data Collection
 HF Continuum l l l l Teach back in hospital using new teaching material Standardized HF on-line discharge instructions Home Care complimentary visit 24 to 48 hours post discharge – use teach back again Physician office visit within three to five days Advance Practice Nurse follow-up phone call on seventh day post discharge – teach back repeated Outpatient Heart Failure class – seeing increased participation Collaboration with cardiology office Heart Failure Clinic
HF Continuum l l l l Teach back in hospital using new teaching material Standardized HF on-line discharge instructions Home Care complimentary visit 24 to 48 hours post discharge – use teach back again Physician office visit within three to five days Advance Practice Nurse follow-up phone call on seventh day post discharge – teach back repeated Outpatient Heart Failure class – seeing increased participation Collaboration with cardiology office Heart Failure Clinic
 Lessons Learned l l l Engaged leadership Worked in tandem with our CMS core measures for HF Took advantage of existing workflows Stories are as important as the data Health literacy: “If they don’t do what we want, we haven’t given them the right information. ” (Vice Admiral Richard Carmona, Former Surgeon General)
Lessons Learned l l l Engaged leadership Worked in tandem with our CMS core measures for HF Took advantage of existing workflows Stories are as important as the data Health literacy: “If they don’t do what we want, we haven’t given them the right information. ” (Vice Admiral Richard Carmona, Former Surgeon General)
 Our Work Continues l l Working on HF LOS Working in conjunction with Cardiologists, PC HF Clinic HF Certification from JCAHO Working with Wellmark to get Home Visit as a covered visit
Our Work Continues l l Working on HF LOS Working in conjunction with Cardiologists, PC HF Clinic HF Certification from JCAHO Working with Wellmark to get Home Visit as a covered visit
 Our Impact By: l Enhancing the patient assessment process on admission l Enhancing patient and family understanding of complex self-care processes l Improving the hand-off of critical information to caregivers in the next care setting l Providing continuity in post acute care follow-up We can reduce unnecessary readmissions for patients with Heart Failure.
Our Impact By: l Enhancing the patient assessment process on admission l Enhancing patient and family understanding of complex self-care processes l Improving the hand-off of critical information to caregivers in the next care setting l Providing continuity in post acute care follow-up We can reduce unnecessary readmissions for patients with Heart Failure.