f99d56af5252a62c046062e24d2b6cb4.ppt
- Количество слайдов: 114



Health Care Crisis United States Health Care by the Numbers Matthew Mc. Coy DC, MPH


Crisis $2 Trillion Dollars a Year is Spent on Health Care in the US (This is equal to the size of the economy of China) Taxpayers pay for 44% of this Health care is 16 -20% of GDP

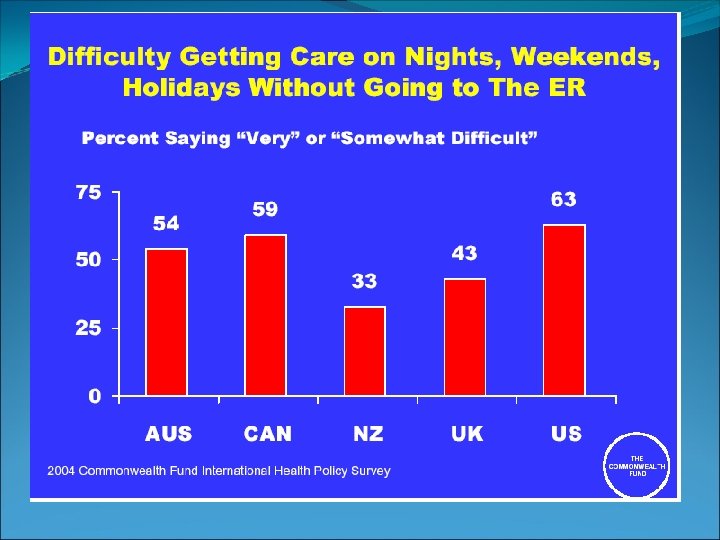
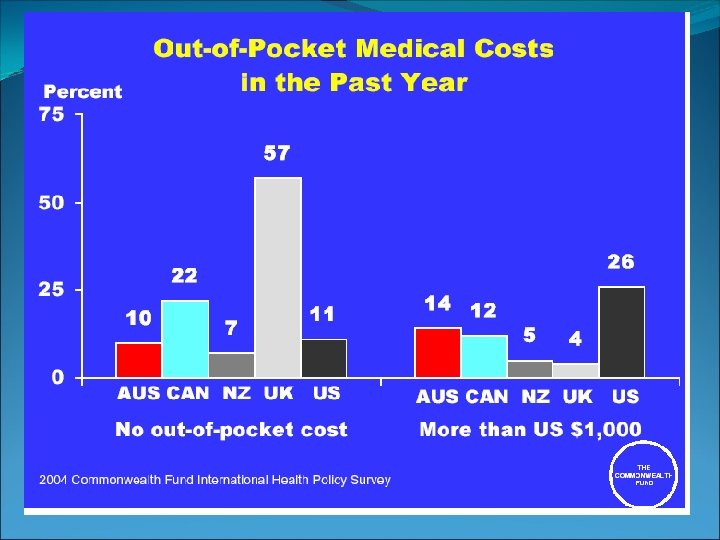
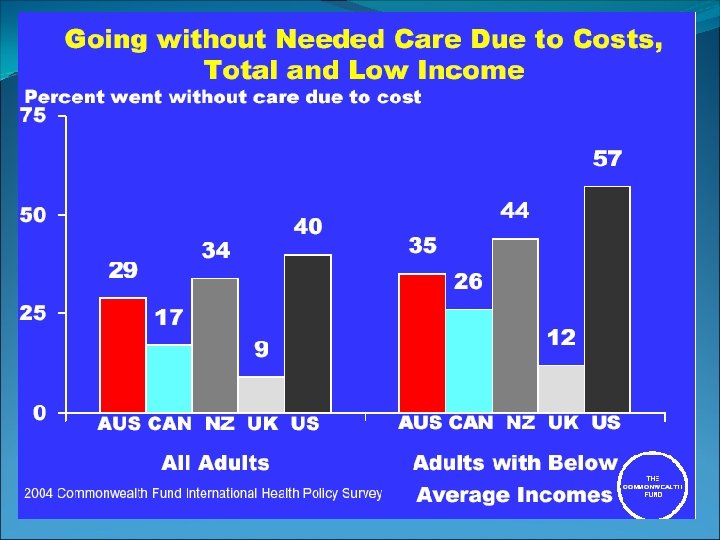
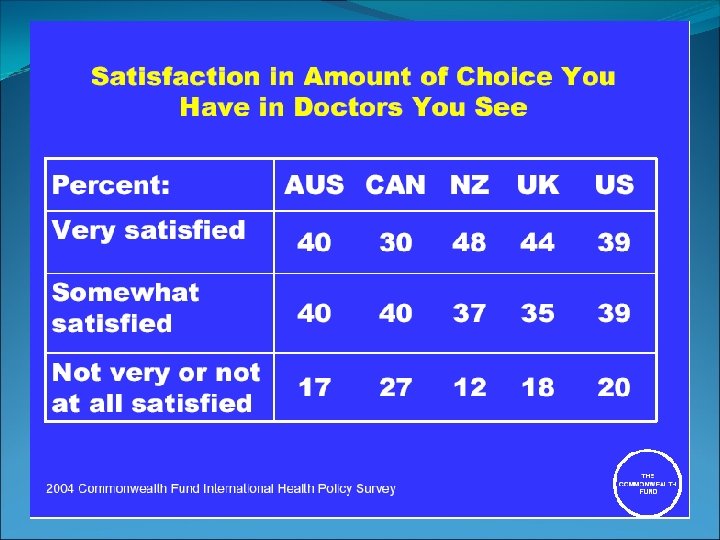
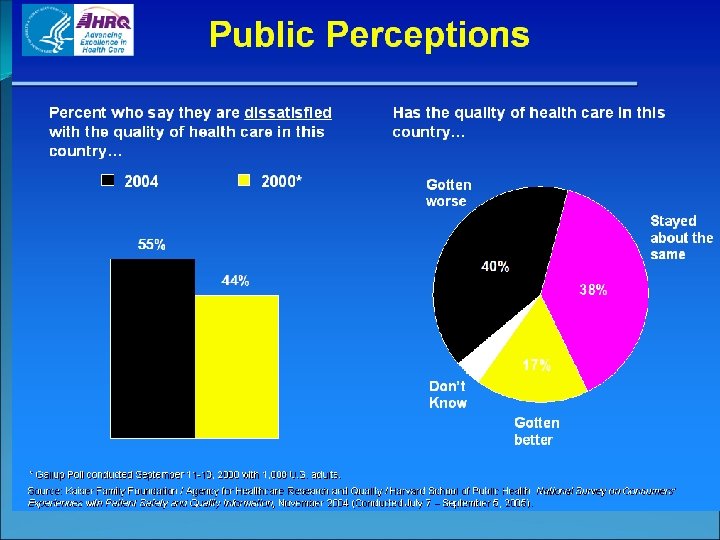
Crisis General Motors spends $5. 2 Billion a year on Health Care (This adds $1600 for every car) US Consumers are more dissatisfied with their care than other nations There are ~50 million uninsured Americans

Crisis Medical bills are leading cause of bankruptcy in US 1/5 of Americans have medical debt they are paying off

Crisis 34% of Americans believe medicine can cure any illness as long as people have access to advanced technology and treatment $6, 100 person is spent on health care Health premiums have risen 98% since 2000

US “Health Care” Expenditures 70% is spent on Chronic illness Cardio and Stroke--$210 billion Cancer--$192 billion Diabetes--$92 billion Obesity-Related--$75 billion Arthritis--$22 billion Kessler A: The End of Medicine, 2006.

US “Health Care” Costs $1 out of every $6 goes to health care. It is estimated to grow to $1 out of $5 by 2015. Will grow to $12, 320 person in 2015, almost double the 2005 figure of $6, 683. May grow to $4 trillion in ten years. Medicare hospital insurance will become insolvent by 2019. U. S. Health Care Bill by 2015: $4 Trillion. ABC News. 2/22/06 2006 Medicare Trustees Report. CMS Office of Public Affairs

Medicare 5% of sickest Medicare beneficiaries account for 47% of Medicare expenditures During the last six months of life, the average number of doctor visits is 41. 5 in New Jersey; while it is 17 in Utah. For each illness studied, higher mortality rates were found in the regions with the most intense care. Less Health Care Can Be Better for Elderly. AP. 5/17/06.

U. S. Lags Behind While health care in the United States is generally touted as being superior to anywhere else, the reality is more harsh. According to the WHO, in terms of life expectancy, the United States lags far behind most other comparable nations. US ranks 28 th in infant mortality among 39 industrialized nations.

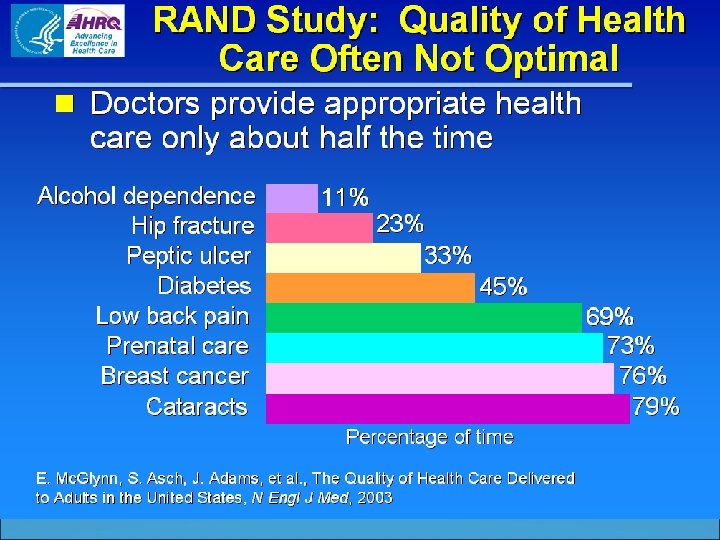
U. S. Lags Behind Compared with 30 other countries, the United States has the highest incidence of all cancers The United States ranks 37 th according to WHO’s assessment of health care systems throughout the world. Americans receive only 55% of needed care (RAND)

US Life Expectancy

Life Expectancy

Cost of Care

Cost v. Quality

Medical Error

Medical Error The Institute of Medicine states medical errors account for at least 100, 000 deaths per year. To Err is Human

Medical Error Others such as Null et al have been more critical asserting that: The number of unnecessary medical and surgical procedures performed annually is 7. 5 million. The number of people exposed to unnecessary hospitalization annually is 8. 9 million. The total number of iatrogenic deaths is 783, 936 annually

Medical Error Dr. Lucian Leape of Harvard estimated that in the United States 180, 000 people die each year as a result of iatrogenic injury. The equivalent of three jumbo-jet crashes every two days.


Medical Error 195, 000 people die each year in hospitals due to preventable errors Other Estimates range from 225, 000 – 284, 000 deaths One million error related non fatal injuries yearly Redefining Health Care Porter and Teisberg

Medical Error Negligence or errors in diagnosis account for 30 -40% of malpractice payments 18 types of errors account for 32, 600 deaths and $9. 3 Billion in extra costs Preventable drug related errors in OP’s cost $77 billion yearly Redefining Health Care Porter and Teisberg

Medical Error Leape of Harvard estimated that in the United States 180, 000 people die each year as a result of iatrogenic injury. The equivalent of three jumbo-jet crashes every two days.

Medical Error According to Public Citizen, medical malpractice kills approximately 80, 000 people per year. Public Citizen stated that if this number is correct than medical malpractice is the 3 rd leading cause of preventable death in the United States just behind cigarettes and alcohol.

Admin Costs Doctors spend ½ - 1/3 of time on paperwork Admin costs are 30% of all health care spending Redefining Health Care Porter and Teisberg


Absurd Solutions Free drugs. Indemnify drug makers. Cap damages to victims. Subsidize malpractice insurance. Keep doing more of what has been shown not to work! Christopher Kent DC, JD

David Eddy, M. D. , Ph. D. Where is the wisdom? Only about 15% of medical interventions are supported by scientific evidence…This is partly because only 1% of the articles in medical journals are scientifically sound. BMJ 1991 303: 798

No Evidence “The problem is that we don't know what we are doing. ” Even with a high-tech health-care system that costs us $2 trillion a year, there is little or no evidence that many widely used treatments and procedures actually work better than various cheaper alternatives. David Eddy

Leading Causes of Death

Leading Causes of Death Why aren’t medical errors listed?

Actual Causes of Death in US

Actual Causes of Death Why aren’t medical errors listed?

Medical Error References Marwick C. US public health system needs major overhaul. BMJ 2002; 325: 1132 16 November http: //bmj. bmjjournals. com/cgi/content/abridged/325/7373/1132 /c? ck=nck. To Err Is Human: Building a Safer Health System. Institute of Medicine 2000 http: //www. nap. edu/books/0309068371/html/ Null G, Dean C, Feldman M, Rasio D, Smith D. The American Medical System Is The Leading Cause Of Death And Injury In The United States. http: //www. ourcivilisation. com/medicine/usamed. htm Leape LL. Error in medicine. JAMA. 1994 Dec 21; 272(23): 1851 -7. Eddy D. Where is the Wisdom BMJ 1991 303: 798 Public Citizen, May/June issue 1994

Health Insurers Invest in Tobacco



18% Negative results Dickersin, 1987 Original research variable Submission 46% Balas, 2002 Negative results Kumar, 1992 0. 6 year Koren, 1989 0. 5 year Kumar, 1992 Acceptance Publication 35% Balas, 1995 Lack of numbers 17: 14 0. 3 year Poyer, 1982 Bibliographic databases 50% Poynard, 1985 Inconsistent indexing 6. 0 - 13. 0 years Expert opinion Antman, 1992 Reviews, guidelines, textbook 9. 3 years Implementation It takes 17 years to turn 14 per cent of original research to the benefit of patient care

Not a New Problem 1601 – Lancaster shows that lemon juice supplement eliminates scurvy among sailors 1747 – Lind shows that citrus juice supplement eliminates scurvy 1795 – (194 years after discovery) British navy implements citrus juice supplement

Treatments Thought to Work but Shown Ineffective Sulphuric acid for scurvy Leeches for almost anything Insulin for schizophrenia Vitamin K for myocardial infarction HRT to prevent cardiovascular disease Flecainide for ventricular tachycardia Routine blood tests prior to surgery ABMT for late stage Breast CA BMJFebruary 28 2004; 324: 474 -5.

State of Quality in the U. S. “The American health care delivery system is in need of fundamental change…. the care delivered is not, essentially, the care we should receive……Between the health care we have and the care we could have lies not just a gap, but a chasm…” “The need for leadership in health care has never been greater. ” IOM, Crossing the Quality Chasm, 2001

Bridging the Quality Chasm Where We Are Where We Want To Be Implementation Innovation Education Diffusion Adoption TRIP

RAND Study: Quality of Health Care Often Not Optimal Patients’ care often deficient, study says. Proper treatment given half the time. On average, doctors provide appropriate health care only half the time, a landmark study of adults in 12 U. S. metropolitan areas suggests. Medical errors corrode quality of healthcare system Medical Care Study: U. S. Often Not Doctors are Optimal not following Failure to Treat. the guidelines Patients Fully Spans Range of What Is for ordinary Expected of illnesses Physicians and Nurses The American healthcare system, often touted as a cutting-edge leader in the world, suddenly finds itself mired in serious questions about the ability of its hospitals and doctors to deliver quality care to millions.

Clarifying National Aims for Improvement Safety Effectiveness -- Matching care to science; avoiding overuse of ineffective care and underuse of effective care Patient Centeredness Timeliness Efficiency Equity

Brainstem Level “We have to get down to the brainstem level and affect how people go through their day on autopilot and change that” Robert Osborne MD

Priority Areas Cancer Chronic kidney disease Diabetes Heart disease HIV/AIDS Maternal and child health Mental illness-depression Respiratory illness (e. g. , asthma, flu)

Chronic & Lifestyle Disease Chronic disease has replaced infectious disease as a significant cause of morbidity and mortality Life expectancy is also on the rise Taken together this has led to the rise of chronic degenerative conditions such as cancer, coronary heart disease, stroke, diabetes, arthritis and other related diseases. While genetics plays a role, these conditions are considered lifestyle diseases and primarily attributed to behaviors related to poor diet, nutrition and physical activity.

Lifestyle The burden of disease has shifted from infectious to chronic diseases (Lee & Rosenburg) These are lifestyle-based Many types of health care providers have developed and aggressively market lifestyle interventions targeted at chronic lifestyle based diseases such as obesity, heart disease, diabetes, and metabolic syndrome It will become increasingly important that consumers, providers, payors and public health experts know which of these interventions produce beneficial outcomes.

Percent of Americans Saying “I Have A Chronic Condition” Source: Chronic Illness and Caregiving Survey, Harris 2000

Lifestyle Modification Intensive lifestyle modifications appear to be beneficial across the spectrum of what are considered to be lifestyle diseases, including hypertension, cardiovascular disease, obesity, overweight, metabolic syndrome, diabetes and in some cases cancer.

Health Care Reform & You A Summary of the Current Proposals As of August 2009

Healthcare Reform & You WHAT ARE THE ELEMENTS OF REFORM? IS THERE HELP FOR THE INSURED? IS THERE MORE SECURITY FOR ALL? WHO PAYS? WHO WON’T BE HAPPY? WHAT IF I HAVE GOOD GROUP COVERAGE? WILL I PAY LESS? WILL MY CARE SUFFER? WHAT DOES IT MEAN FOR OLDER AMERICANS?

What are the elements of the plan? Would require virtually all Americans to carry health insurance with specified minimum benefits or pay a penalty. Would require all but the smallest businesses to provide and subsidize insurance that meets minimum standards for their workers or pay a fee for failing to do so. Reforms are expected to help the poorest of the uninsured by expanding Medicaid. Middle-class Americans — earning up to three or four times the poverty level, or $66, 000 to $88, 000 for a family of four — would get subsidies to help them buy coverage through new health insurance exchanges, national or state, which would offer a menu of policies from different companies.

Is there help for the uninsured? The legislation seems almost certain to include a new marketplace, the health insurance exchange. With tens of millions of new subscribers, virtually all major insurers are expected to offer policies through an exchange. These companies would have to agree to provide a specified level of benefits They would set premiums at rates more comparable to group rates for big employers. The Congressional Budget Office estimates that 36 million people would be covered by policies purchased on an exchange by 2019.

Is there more security for all? All insurance companies would be more tightly regulated. Would require that all new policies sold on or off the exchanges must offer yet-to-be-determined “essential benefits. ” It would prohibit those policies from excluding or charging higher rates to people with pre-existing conditions and would bar the companies from rescinding policies after people come down with a serious illness. It would also prohibit insurers from setting annual or lifetime limits on what a policy would pay. All this would kick in immediately for all new policies. These rules would start in 2013 for policies purchased on the exchange, and, after a grace period, would apply to employerprovided plans as well.

Who pays? Current estimates suggest that it would cost in the neighborhood of $1 trillion over 10 years to extend coverage to tens of millions of uninsured Americans. Under current plans, half or more of that would be covered by reducing payments to providers within the Medicare program, but the rest would require new taxes or revenue sources. According to Obama and House Democratics, the entire tax burden would be dropped on families earning more than $250, 000 or $350, 000 or $1 million a year.

Who won’t be happy? Healthy young people who might prefer not to buy insurance at all will probably be forced to by a federal mandate. Conscripting healthy people into the insured pool would help reduce the premiums for sicker people.

What if I have good group coverage? The main gain for these people is greater security. If they got laid off or chose to leave their jobs, they would no longer be faced with the exorbitant costs of individually bought insurance but could buy new policies through the insurance exchanges at affordable rates. President Obama has also pledged that if you like your current insurance you can keep it. Right now employers are free to change or even drop your coverage at any time. Under likely reforms, they would remain free to do so, provided they paid a penalty to help offset the cost for their workers who would then buy coverage through an exchange. All employers would eventually be allowed to enroll their workers in insurance exchanges that would offer an array of policies to choose from, including a public plan whose premiums would almost certainly be lower than those of competing private plans.

Will I pay less? Two factors could help drive down the premiums for those who are insured. In the short-term, if reform manages to cover most of the uninsured, that should greatly reduce the amount of charity care delivered by hospitals and eliminate the need for the hospitals to shift such costs to patients who have private insurance. One oft-cited study estimates that cost-shifting to cover care for the uninsured adds about $1, 000 to a family’s annual insurance premiums; other experts think it may be a few hundred dollars. In theory, eliminating most charity care should help hold down or even reduce the premiums charged for private insurance. When, if ever, that might happen is unclear. The theory is, if reform efforts slow the growth of health care costs, then the increase in insurance costs should ease as well. And if the new health insurance exchanges — and possibly a new public plan — inject more competition into markets that are often dominated by one or two big private insurance companies, that, too, could help bring down premiums.

Will my care suffer? Critics have raised the specter that health care will be “rationed” to save money. The truth is that health care is already rationed. No insurance, public or private, covers everything at any cost. That will not change any time soon. The long-term goal of health reform is to get rid of the fee-forservice system in which patients often get very expensive care but not necessarily the best care. Virtually all experts blame the system for runaway health care costs because it pays doctors and hospitals for each service they perform, thus providing a financial incentive to order excessive tests or treatments, some of which harm the patients.

Will my care suffer The reform bills call for research and pilot programs to find ways to both control costs and improve patients’ care. The bills would alter payment incentives in Medicare to reduce needless readmissions to hospitals. They would promote comparative effectiveness research to determine which treatments are best but would not force doctors to use them. And they call for pilot programs in Medicare to test the best ways for doctors to manage and coordinate a patient’s total care. Any changes in the organization of care would take time to percolate from Medicare throughout the health care system. They are unlikely to affect most people in the immediate future.

What about older Americans? The drug industry has already agreed to provide 50 percent discounts on brand-name drugs to Medicare beneficiaries who have reached the so-called “doughnut hole” where they must pay the full cost of their medicines. Gradually phase out the doughnut hole entirely, thus making it less likely that beneficiaries will stop taking their drugs once they have to pay the whole cost. Congress is likely to reduce or do away with Medicare Advantage subsidies. If so, many of these plans are apt to charge their clients more for their current policies or offer them fewer benefits. Reformers are planning to finance universal coverage in large part by saving money in the traditional Medicare program, raising the question of whether all beneficiaries will face a reduction in benefits. Obama insisted that benefits won’t be reduced, they’ll simply be delivered in more efficient ways, like better coordination of care, elimination of duplicate tests and reliance on treatments known to work best.


National Health Care Do we already have national health care? The following data is from: The Employee Benefits Research Institute Selden, T: Agency for Healthcare Research and Quality Data from the National Health Expenditures Accounts Himmelstein, D: Associate professor of medicine at Harvard Medical School. Reinhardt, U: Princeton University

Employer Based Care From 2000 to 2005, the proportion of workers aged 18 to 64 with employmentbased health benefits was 70. 6 percent – down slightly from 74. 5 percent.

The Uninsured A record 46. 6 million Americans lacked health insurance last year. Of them, more than 82 percent lived in households headed by someone holding a job.

Medicare Enrollment Out of a total population of about 300 million, 35. 6 million elderly Americans were on Medicare in 2005.

Covered Workers Of the working-age population, which reached 257. 8 million in 2005, 45. 5 million were covered by Medicare, Medicaid or military health programs.

Federal & State Insured Another 18. 2 million workers had health insurance through public jobs such as state, federal and local governments, public schools and state universities.

Dependents Also Covered Millions of those workers’ dependents are covered as well. Even if those dependents are not included in the total, taxpayers paid the bill for almost two-fifths of all Americans with insurance in 2005.

100 Million Americans This means that at minimum 100 million Americans healthcare is paid for directly by the government and tax dollars.

Tax Subsidies The tax subsidy for employment-related health coverage was $208. 6 billion in 2006, or 35. 4 percent of the amount spent on premiums.

Medicare & Medicaid Costs In fiscal 2006, spending on Medicare was $378. 7 billion and federal spending on Medicaid was $180. 6 billion.

Public Expenditures Public expenditures on health care — Medicare, Medicaid, military health care and federal employee benefits — accounted for $888 billion of the $1. 96 trillion spent on health care in 2004.

$1. 2 Trillion Adding in the subsidies, and premiums paid for public-sector employees, the total comes to $1. 2 trillion, or 61 percent.

2/3 of Health Spending According to Uwe E. Reinhardt, the James Madison professor of political economy at Princeton, the government accounts for about two-thirds of health care spending.

GDP Comparison In 2004, government spending on health care equaled 9. 6 percent of the gross domestic product, compared with 6. 9 percent in Canada.

$1 Trillion Dollars to Fix it Estimates are that it will cost $1 Trillion to institute the current health care reforms being proposed.

What does one TRILLION dollars look like? All this talk about "stimulus packages" and "bailouts". . . A billion dollars. . . A hundred billion dollars. . . Eight hundred billion dollars. . . One TRILLION dollars. . .

We'll start with a $100 dollar bill. Currently the largest U. S. denomination in general circulation. Most everyone has seen them, slightly fewer have owned them. Guaranteed to make friends wherever they go.

A packet of one hundred $100 bills is less than 1/2" thick and contains $10, 000. Fits in your pocket easily and is more than enough for week or two of shamefully decadent fun.

Believe it or not, this next little pile is $1 million dollars (100 packets of $10, 000). You could stuff that into a grocery bag and walk around with it.

While a measly $1 million looked a little unimpressive, $100 million is a little more respectable. It fits neatly on a standard pallet. . .

And $1 BILLION dollars. . . now we're really getting somewhere. . .

One Trillion Dollars Next we'll look at ONE TRILLION dollars. This is that number we've been hearing about so much. What is a trillion dollars? Well, it's a million. It's a thousand billion. It's a one followed by 12 zeros. You ready for this? It's pretty surprising. Go ahead. . . Turn the page. . . Ladies and gentlemen. . . I give you $1 trillion dollars. . .
 So the next")
$1, 000, 000 (And notice those pallets are double stacked. ) So the next time you hear someone toss around the phrase "trillion dollars". . . that's what they're talking about. Does this bother you? ? ? It will certainly bother your grand children!!!

The Birth of Outcomes Measurement


The Birth of Outcomes In 1973 In Vermont 2 researchers studied the haphazard patterns of surgery in the state using hospital data. They found town to town variations in rates of common operations that were unexplainable. CONCLUSION: Geography determined treatment _______________ Wennberg J. , Gittelsohn A: Small area variations in health care delivery. Science Dec. 14, 1973. 182(117) 1102 -8.

Geography “IN HEALTH CARE MARKETS, GEOGRAPHY IS DESTINY” _____________________ The Dartmouth Atlas of Healthcare, 1996 Center for the Evaluative Clinical Sciences, Dartmouth Medical School

Costs "These front end costs are recouped many times over when they produce results-even when the results may not be apparent for a few years. The long term challenge, then, is to convince payers to look beyond short term goals and invest in outcomes management with the expectation that the real payoff-improvement in overall healthmay lie as far as a decade or more down the road". _______________________ Outcomes Management Comes of Age In: Outcomes Management Special Report, 1996.

Measurement "If you can't measure it, you can't improve it". _________ Dr. David Nash from the Office of Health Policy Outcomes at Thomas Jefferson University, Philadelphia

Measurement II "Measuring and managing outcomes is what we're trying to move towards". _________________ Patricia Powers Executive Director of the Pacific Area Business Group on Health, the largest employer health care purchasing coalition in the United States.

"THE GOAL IS THE BEST CARE POSSIBLE FOR EVERY PATIENT EVERY DAY. OUR PATIENTS DESERVE NOTHING LESS" ________________ Robert Waller President and CEO of The Mayo Foundation From Demanding Medical Excellence
f99d56af5252a62c046062e24d2b6cb4.ppt