

1a1d2cc1d2b9159891a793bd3c96b1b1.ppt
- Количество слайдов: 54
 Giving addiction its due* Addiction what is the added value of the concept today? The University of Helsinki Centre for Research on Addictions Gene M. Heyman Dept. of Psychology, Boston College October 15, 2012 * This is actually my 2 nd talk First talk: Some basic findings on drug use (among DSM “addicts”)
Giving addiction its due* Addiction what is the added value of the concept today? The University of Helsinki Centre for Research on Addictions Gene M. Heyman Dept. of Psychology, Boston College October 15, 2012 * This is actually my 2 nd talk First talk: Some basic findings on drug use (among DSM “addicts”)
 Outline of topics Context: What experts and addicts say about addiction, policy, individual responsibility Two questions: – Is addiction a chronic disorder – Does drug use become involuntary Approach: – Use DSM to distinguish addicts from drug users – Look at the data Why don’t they just quit? * Is addiction like other psychiatric disorders? **
Outline of topics Context: What experts and addicts say about addiction, policy, individual responsibility Two questions: – Is addiction a chronic disorder – Does drug use become involuntary Approach: – Use DSM to distinguish addicts from drug users – Look at the data Why don’t they just quit? * Is addiction like other psychiatric disorders? **
 Views on addiction from experts: Alan Leshner & Nora Volkow, past and present directors of US National Institute on Drug Abuse (NIDA) “Addiction is a brain disease. . . For most people, it [addiction] is a chronic relapsing disorder. . addiction must be approached more like other chronic illnesses. ” “A metaphorical switch in the brain [is] thrown as a result of prolonged drug use. Initially, drug use is a voluntary behavior, but when that switch is thrown, the individual moves into a state of addiction, characterized by compulsive drug seeking and use. ” Leshner, Science, 1997. “The key symptoms of addiction. . . are compulsive drug intake and intense drive to take the drug. . ” “at the expense of lifepreserving activities. ”Volkow, 1992, 2000
Views on addiction from experts: Alan Leshner & Nora Volkow, past and present directors of US National Institute on Drug Abuse (NIDA) “Addiction is a brain disease. . . For most people, it [addiction] is a chronic relapsing disorder. . addiction must be approached more like other chronic illnesses. ” “A metaphorical switch in the brain [is] thrown as a result of prolonged drug use. Initially, drug use is a voluntary behavior, but when that switch is thrown, the individual moves into a state of addiction, characterized by compulsive drug seeking and use. ” Leshner, Science, 1997. “The key symptoms of addiction. . . are compulsive drug intake and intense drive to take the drug. . ” “at the expense of lifepreserving activities. ”Volkow, 1992, 2000
, author, counter culture hero, opiate addict Junk yields") Views on Addiction: William Burroughs (19141998), author, counter culture hero, opiate addict Junk yields a basic formula of “evil” virus: . . . A dope fiend is a man in total need of dope. . . Dope fiends are sick people who cannot act other than they do. A rabid dog cannot choose but bite. Naked Lunch (1959)
Views on Addiction: William Burroughs (19141998), author, counter culture hero, opiate addict Junk yields a basic formula of “evil” virus: . . . A dope fiend is a man in total need of dope. . . Dope fiends are sick people who cannot act other than they do. A rabid dog cannot choose but bite. Naked Lunch (1959)
 Policy recommendations regarding insurance coverage and individual responsibility for addiction “. . effects of drug dependence treatment are optimized when patients remain in continuing care and monitoring without limits or restrictions on the number of days or visits covered. ” – (A. T. Mc. Lellan, Recent Deputy Director of Drug Control Policy, Obama Administration) “Ten percent of [the] population [are] unknowingly vulnerable to alcoholism when they drink. They can’t be held responsible for developing that illness. ” – Dr. David Gastfriend, Recent Director of the Addiction Research Center at Massachusetts General “ I find it useful to conceptualize addiction as the cancer of behavior. How else could one fathom the mother who buys cocaine for herself instead of food for her children …” – Dr. P. Martin in New England Journal of Medicine
Policy recommendations regarding insurance coverage and individual responsibility for addiction “. . effects of drug dependence treatment are optimized when patients remain in continuing care and monitoring without limits or restrictions on the number of days or visits covered. ” – (A. T. Mc. Lellan, Recent Deputy Director of Drug Control Policy, Obama Administration) “Ten percent of [the] population [are] unknowingly vulnerable to alcoholism when they drink. They can’t be held responsible for developing that illness. ” – Dr. David Gastfriend, Recent Director of the Addiction Research Center at Massachusetts General “ I find it useful to conceptualize addiction as the cancer of behavior. How else could one fathom the mother who buys cocaine for herself instead of food for her children …” – Dr. P. Martin in New England Journal of Medicine
 One more account: Patty: Mother of two girls, heavy cocaine user for 15 years, drug dealer Oh, for a time my nose opened up when I went out partying and drinking, but I learned how to handle it. You know, I never really decided to quit using. I just quit selling. Once I stopped selling I didn’t have the money to buy it anymore. I would have literally had to say, “ Sorry, girls, you don’t eat this week” to buy some. I would have exactly $80 for two weeks of food. Waldorf et al. (1991)Cocaine changes: The experience of using and quitting.
One more account: Patty: Mother of two girls, heavy cocaine user for 15 years, drug dealer Oh, for a time my nose opened up when I went out partying and drinking, but I learned how to handle it. You know, I never really decided to quit using. I just quit selling. Once I stopped selling I didn’t have the money to buy it anymore. I would have literally had to say, “ Sorry, girls, you don’t eat this week” to buy some. I would have exactly $80 for two weeks of food. Waldorf et al. (1991)Cocaine changes: The experience of using and quitting.
 Some context, an example of human decision making: What to eat when you have a severe food allergy Ira Glass: “Barbara said. . . she got incredibly sick, throwing up, rushing to the emergency room, getting an IV, an anti-nausea medication. . . ”. Barbara: “And being on vacation now, I've got a room full of popcorn and trail mix. ” Ira Glass: “You do? Right now? Wait, don't you think you're playing with fire? ” Barbara: “Well, you know, it's not going to kill me. And if it does, I won't know. ” Ira Glass: “Just a quick trip to the hospital, an IV, some medication. ” Ira Glass: This is Michelle De. Vito, an emergency room doctor. . . she says that nearly every day, she sees somebody with a food allergy who has eaten the food that they're not supposed and ended up in her ER. Michelle De. Vito: “The ER is a virtual laboratory of dysfunctional behaviors and bad choices. . much of the pathology we see in the ER is a result of bad choices. And some of them, decades of bad choices. ”
Some context, an example of human decision making: What to eat when you have a severe food allergy Ira Glass: “Barbara said. . . she got incredibly sick, throwing up, rushing to the emergency room, getting an IV, an anti-nausea medication. . . ”. Barbara: “And being on vacation now, I've got a room full of popcorn and trail mix. ” Ira Glass: “You do? Right now? Wait, don't you think you're playing with fire? ” Barbara: “Well, you know, it's not going to kill me. And if it does, I won't know. ” Ira Glass: “Just a quick trip to the hospital, an IV, some medication. ” Ira Glass: This is Michelle De. Vito, an emergency room doctor. . . she says that nearly every day, she sees somebody with a food allergy who has eaten the food that they're not supposed and ended up in her ER. Michelle De. Vito: “The ER is a virtual laboratory of dysfunctional behaviors and bad choices. . much of the pathology we see in the ER is a result of bad choices. And some of them, decades of bad choices. ”
 Some initial conclusions The understanding of addiction has consequences for public policy and tax dollars Many cases (e. g. , Burroughs) are consistent with the disease/compulsive model (“rabid dogs”) ---but not all – Real addicts vs. apparent addicts – No “real” addicts? – Food allergies (and addiction): human nature/decision making revealed? How to proceed
Some initial conclusions The understanding of addiction has consequences for public policy and tax dollars Many cases (e. g. , Burroughs) are consistent with the disease/compulsive model (“rabid dogs”) ---but not all – Real addicts vs. apparent addicts – No “real” addicts? – Food allergies (and addiction): human nature/decision making revealed? How to proceed
") Find a tool for identifying “addicts” then test if they are chronic, compulsive (involuntary) drug users.
Find a tool for identifying “addicts” then test if they are chronic, compulsive (involuntary) drug users.
 criteria for “substance dependence”") How to identify addicts Use the American Psychiatric Association (DSM) criteria for “substance dependence” to distinguish addicts from drug users Rationale: – – – Official criteria for clinics, courts, & researchers Reliable/research based Divides drug users into meaningful categories Key feature: persistence of drug use despite aversive consequences – – – High levels of drug use Use despite health & job risks Relapse & takes more than initially intended
How to identify addicts Use the American Psychiatric Association (DSM) criteria for “substance dependence” to distinguish addicts from drug users Rationale: – – – Official criteria for clinics, courts, & researchers Reliable/research based Divides drug users into meaningful categories Key feature: persistence of drug use despite aversive consequences – – – High levels of drug use Use despite health & job risks Relapse & takes more than initially intended
 drug") Questions regarding DSM “addicts” Are they chronic cases? Do they become involuntary (compulsive) drug users?
Questions regarding DSM “addicts” Are they chronic cases? Do they become involuntary (compulsive) drug users?
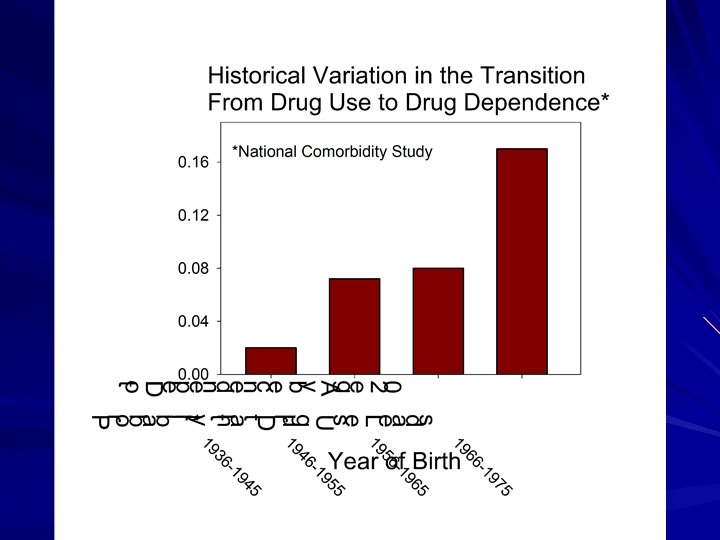
 Overall prevalence of use and dependence
Overall prevalence of use and dependence
 Is addiction a chronic disorder, as so often claimed? paraphrasing O’Brien and Mc. Lellan: “cure is an unrealistic hope, addiction requires lifelong treatment as does “arthritis, diabetes, asthma”’ Rem% = (LT-C)/LT Community Studies Textbook of Clinical Psychiatry: “for addiction patients recovery is a never-ending process, the term cure is avoided.
Is addiction a chronic disorder, as so often claimed? paraphrasing O’Brien and Mc. Lellan: “cure is an unrealistic hope, addiction requires lifelong treatment as does “arthritis, diabetes, asthma”’ Rem% = (LT-C)/LT Community Studies Textbook of Clinical Psychiatry: “for addiction patients recovery is a never-ending process, the term cure is avoided.
 High remission rates for different drugs Did type of drug matter?
High remission rates for different drugs Did type of drug matter?
 How long does substance dependence persist? Increasing functions suggest that once addicts quit, they usually do not resume heavy drug use Yrs to 50% quit: Cocaine: 4 Marijuana: 6 Alcohol: 16 Cigarettes: 31 Lopez-Quintero, 2010
How long does substance dependence persist? Increasing functions suggest that once addicts quit, they usually do not resume heavy drug use Yrs to 50% quit: Cocaine: 4 Marijuana: 6 Alcohol: 16 Cigarettes: 31 Lopez-Quintero, 2010
 Other methodological issues Missing addicts? Do high remission rates persist when self-report is validated?
Other methodological issues Missing addicts? Do high remission rates persist when self-report is validated?
 Why do we say that addiction is a “chronic” disorder, when the data say otherwise? Clinics as basis for understanding of addiction But most addicts do not seek treatment Berkson’s bias: those in clinic have more than one disorder Predictions: – Drug use persists longer in clinic populations – Clinic populations have more disorders (Berkson’s bias)
Why do we say that addiction is a “chronic” disorder, when the data say otherwise? Clinics as basis for understanding of addiction But most addicts do not seek treatment Berkson’s bias: those in clinic have more than one disorder Predictions: – Drug use persists longer in clinic populations – Clinic populations have more disorders (Berkson’s bias)
 Clinic results support received wisdom: “Addiction is a chronic disorder” Typical clinic study results
Clinic results support received wisdom: “Addiction is a chronic disorder” Typical clinic study results
 Berkson’s bias
Berkson’s bias
 Is addiction a chronic disorder, according to the data? Summary Yes, for some (perhaps most) clinic populations But most addicts do not seek/end up in treatment Illicit drug addicts not in treatment tend to quit by age 30 (alcohol and cigarettes quit at lower rates) One difference in the two groups: Additional medical disorders
Is addiction a chronic disorder, according to the data? Summary Yes, for some (perhaps most) clinic populations But most addicts do not seek/end up in treatment Illicit drug addicts not in treatment tend to quit by age 30 (alcohol and cigarettes quit at lower rates) One difference in the two groups: Additional medical disorders
? In 1619, Robert Harris described habitual") Is addiction a disease (meaning involuntary drug use)? In 1619, Robert Harris described habitual drunkenness as this “Dropsilike disease. ” In 1628, William Prynne notes that drunkenness is a “dangerous dropsie and disease. ” John Bury (1677) writes: “drunkenness is a disease so epidemical that all the Physicians in England know not how to stop it. ”
Is addiction a disease (meaning involuntary drug use)? In 1619, Robert Harris described habitual drunkenness as this “Dropsilike disease. ” In 1628, William Prynne notes that drunkenness is a “dangerous dropsie and disease. ” John Bury (1677) writes: “drunkenness is a disease so epidemical that all the Physicians in England know not how to stop it. ”
 Who are these early commentators and what were they thinking? British clergymen Basis of diagnosis (1609): those who addict themselves. . . turn delight into necessitie. . . yet against all rules of reason. . . they will not leave their drunkenness Drinking seemed irrational therefore it was a disease (assumption: voluntary behavior is rational)
Who are these early commentators and what were they thinking? British clergymen Basis of diagnosis (1609): those who addict themselves. . . turn delight into necessitie. . . yet against all rules of reason. . . they will not leave their drunkenness Drinking seemed irrational therefore it was a disease (assumption: voluntary behavior is rational)
 Additional, more recent explanations: addiction is a disease because it has a biological basis: genes and drug-induced changes in the brain Genetic etiology: “the evidence of this physical basis (genes) has significantly advanced the acceptance of alcoholism (addiction) as a disease. ” Miller & Chappel (1991) Drugs change the brain: “That addiction is tied to changes in brain structure and function is what makes it, fundamentally, a disease. ” Alan Leshner, Science (1997)
Additional, more recent explanations: addiction is a disease because it has a biological basis: genes and drug-induced changes in the brain Genetic etiology: “the evidence of this physical basis (genes) has significantly advanced the acceptance of alcoholism (addiction) as a disease. ” Miller & Chappel (1991) Drugs change the brain: “That addiction is tied to changes in brain structure and function is what makes it, fundamentally, a disease. ” Alan Leshner, Science (1997)
 Changes in nucleus accumbens and cortex produce a “recipe for addiction. ” Fig. 5. Photographs of three examples of apparently anomalous apical dendrites on Cg 3 pyramidal cells in rats that selfadministered cocaine (see text). Robinson et al. , 2001, Synapse…
Changes in nucleus accumbens and cortex produce a “recipe for addiction. ” Fig. 5. Photographs of three examples of apparently anomalous apical dendrites on Cg 3 pyramidal cells in rats that selfadministered cocaine (see text). Robinson et al. , 2001, Synapse…
 Motor sensitization (3 x a much cocaine as in Perhaps as much as 15 Robinson study); saccharin linked to lower DA g/day for humans (or release) Recall Volkow : “at expense of life about 1 -2 wk supply for preserving activities”) heavy user).
Motor sensitization (3 x a much cocaine as in Perhaps as much as 15 Robinson study); saccharin linked to lower DA g/day for humans (or release) Recall Volkow : “at expense of life about 1 -2 wk supply for preserving activities”) heavy user).
 The proper question All psychological phenomena vary as a function of variation in genes and brain structure/function Thus, we can ask: do genes and drug- induced neural adaptations insulate drug use in addicts from the determinants of choice? Does biology of addiction lead to involuntary drug use?
The proper question All psychological phenomena vary as a function of variation in genes and brain structure/function Thus, we can ask: do genes and drug- induced neural adaptations insulate drug use in addicts from the determinants of choice? Does biology of addiction lead to involuntary drug use?
 Criteria for the voluntary/involuntary continuum Not free will Different causal relations: elicited vs. feedback Elicited: reflexes, instincts Feedback: Values, sanctions, opinion of others, costs benefits, punishment, reward, etc.
Criteria for the voluntary/involuntary continuum Not free will Different causal relations: elicited vs. feedback Elicited: reflexes, instincts Feedback: Values, sanctions, opinion of others, costs benefits, punishment, reward, etc.
 Examples and difficult cases Contrasts – – – Patellar reflex vs. kick Blush vs. rouge Blink vs. wink Ballistic missile vs. guided missile Sneezing vs. spitting Difficult cases: OCD symptoms, compelled crimes (e. g. , kidnap victim forced to rob bank)
Examples and difficult cases Contrasts – – – Patellar reflex vs. kick Blush vs. rouge Blink vs. wink Ballistic missile vs. guided missile Sneezing vs. spitting Difficult cases: OCD symptoms, compelled crimes (e. g. , kidnap victim forced to rob bank)
 Do the factors that influence choice help bring drug use to a halt in addicts (and can the same be said for symptoms of other psychiatric disorders? ) Logical implications of high remission rates plus nonclinic recovery in community samples Correlates of recovery: – Information: Surgeon General’s Report on smoking (1964) – Historical events: Harrison narcotics tax act (1914) /Prohibition (alcohol) – Biographies: values and practical concerns
Do the factors that influence choice help bring drug use to a halt in addicts (and can the same be said for symptoms of other psychiatric disorders? ) Logical implications of high remission rates plus nonclinic recovery in community samples Correlates of recovery: – Information: Surgeon General’s Report on smoking (1964) – Historical events: Harrison narcotics tax act (1914) /Prohibition (alcohol) – Biographies: values and practical concerns
 Common themes in biographical accounts of quitting: Stories are laced with explicit and implicit values: – – : “I wasn’t put on earth to be an addict” “I wanted my parents to be proud of me again” “I didn’t want to embarrass my children” “I was sick of the hassles” Ordinary concerns – Fear of arrest – Finances and occupational concerns – Family pressures
Common themes in biographical accounts of quitting: Stories are laced with explicit and implicit values: – – : “I wasn’t put on earth to be an addict” “I wanted my parents to be proud of me again” “I didn’t want to embarrass my children” “I was sick of the hassles” Ordinary concerns – Fear of arrest – Finances and occupational concerns – Family pressures
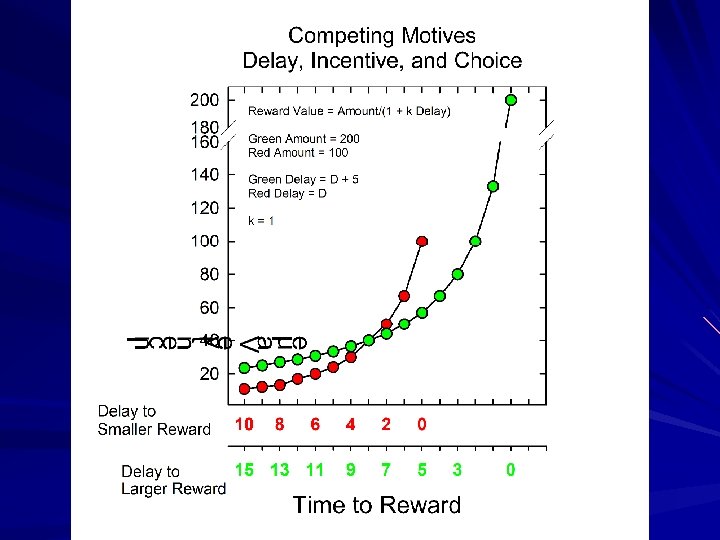
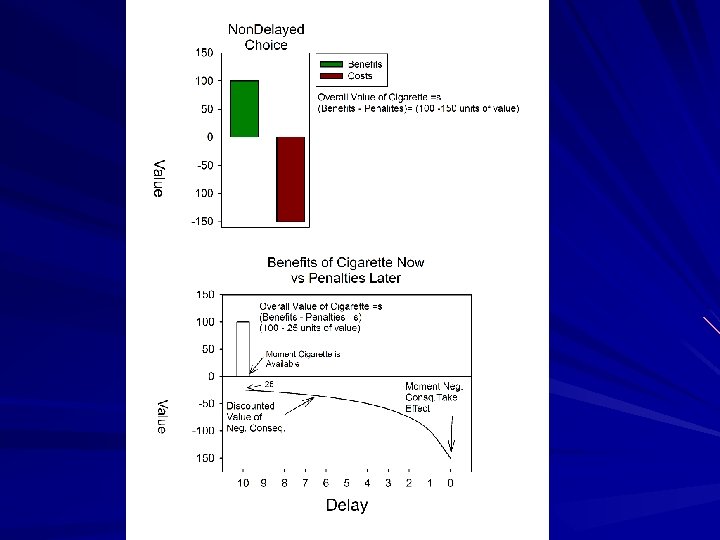
 If drug use is voluntary, why don’t addicts just quit? Drug is the better choice from a local perspective (1) Addictive drugs are behaviorally “toxic”---they undermine the value of competing activities Benefits are immediate; costs are delayed No direct self-satiating mechanisms as with most other rewarding activities Intoxicating, whereas moderation depends on judgment
If drug use is voluntary, why don’t addicts just quit? Drug is the better choice from a local perspective (1) Addictive drugs are behaviorally “toxic”---they undermine the value of competing activities Benefits are immediate; costs are delayed No direct self-satiating mechanisms as with most other rewarding activities Intoxicating, whereas moderation depends on judgment
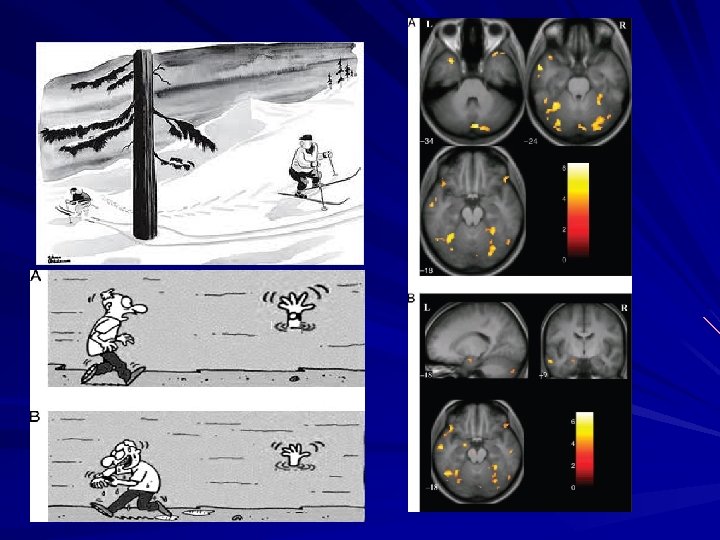
 Intoxication, depression, anxiety") If drug use is voluntary why don’t addicts just quit? (2) Intoxication, depression, anxiety and other emotional states reduce the frame of reference to “now” Lifestyle associated with drug use may not include activities with long time horizons, thereby promoting local frame of reference
If drug use is voluntary why don’t addicts just quit? (2) Intoxication, depression, anxiety and other emotional states reduce the frame of reference to “now” Lifestyle associated with drug use may not include activities with long time horizons, thereby promoting local frame of reference
 Is addiction like other mental disorders Yes, e. g. , analogous to OCD: symptom provides immediate reward, resisting symptom provides delayed larger reward No: – Addiction’s unique idioms – Addiction’s unique correlates of recovery: legislation, opinion of others, AA – Importance of cohort
Is addiction like other mental disorders Yes, e. g. , analogous to OCD: symptom provides immediate reward, resisting symptom provides delayed larger reward No: – Addiction’s unique idioms – Addiction’s unique correlates of recovery: legislation, opinion of others, AA – Importance of cohort
 The original talk summarized: “Addiction” is a useful label Addiction as compulsion is not in accord with the research Addiction as a psychiatric disorder is questionable
The original talk summarized: “Addiction” is a useful label Addiction as compulsion is not in accord with the research Addiction as a psychiatric disorder is questionable
 The talk that there is not time for: Why are we so susceptible to the idea that addicts are compulsive drug users?
The talk that there is not time for: Why are we so susceptible to the idea that addicts are compulsive drug users?
 Recall William Burroughs Junk yields a basic formula of “evil” virus: . . . A dope fiend is a man in total need of dope. . . Dope fiends are sick people who cannot act other than they do. A rabid dog cannot choose but bite. From: Naked Lunch (1959)
Recall William Burroughs Junk yields a basic formula of “evil” virus: . . . A dope fiend is a man in total need of dope. . . Dope fiends are sick people who cannot act other than they do. A rabid dog cannot choose but bite. From: Naked Lunch (1959)
 “I stood there with") Burroughs redux His allowance from home stops (at age 40) “I stood there with my last check in my hand realized that it was my last check. I took the next plane to London [to enter “treatment”]. ” – From Naked Lunch…(1959)
Burroughs redux His allowance from home stops (at age 40) “I stood there with my last check in my hand realized that it was my last check. I took the next plane to London [to enter “treatment”]. ” – From Naked Lunch…(1959)
 Graph is consistent with Amer. Psych Assoc. definition of addiction: Persistence of drug use despite negative consequences Graph is consistent with temporal pattern of addiction: alternating periods of drug use and abstinence
Graph is consistent with Amer. Psych Assoc. definition of addiction: Persistence of drug use despite negative consequences Graph is consistent with temporal pattern of addiction: alternating periods of drug use and abstinence
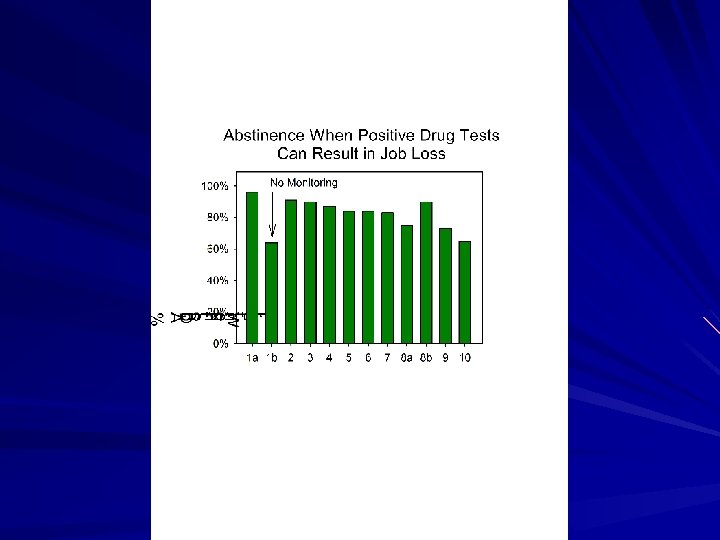
 Explicit test of incentives
Explicit test of incentives
 Choice-based voucher treatment: Cocaine dependent users Incentives and drug use in cocaine addicts
Choice-based voucher treatment: Cocaine dependent users Incentives and drug use in cocaine addicts
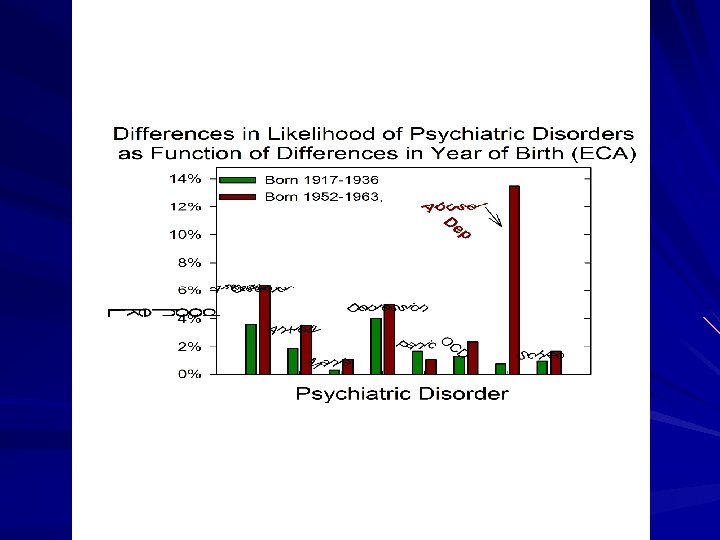
 Do all psych disorders have high remission rates?
Do all psych disorders have high remission rates?
 How can we justify interventions to aid addicts, if they so often quit on their own? We can shorten the period of self-destructive drug use Likelihood of quitting depends on alternatives and judgment. – Drug user may have few alternatives – Assuming a better alternative to drug use exists, it may take sober effort to achieve it
How can we justify interventions to aid addicts, if they so often quit on their own? We can shorten the period of self-destructive drug use Likelihood of quitting depends on alternatives and judgment. – Drug user may have few alternatives – Assuming a better alternative to drug use exists, it may take sober effort to achieve it
 Missing Addicts? Perhaps addicts who keep using are missing? Assume most addicts remain addicts but go missing. Thus real % no longer showing symptoms is 20% not 80%. How many missing addicts are there? Let 80% = True % of current addicts = (Current Addicts + X)/(X + Lifetime Addicts), where X = number of missing addicts. X = 3 x Current lifetime addicts (or about 12 % of Americans were addicted to an illicit drug at some time in their life---and 75% of this population (>20 M) cannot be found are still addicted or dead
Missing Addicts? Perhaps addicts who keep using are missing? Assume most addicts remain addicts but go missing. Thus real % no longer showing symptoms is 20% not 80%. How many missing addicts are there? Let 80% = True % of current addicts = (Current Addicts + X)/(X + Lifetime Addicts), where X = number of missing addicts. X = 3 x Current lifetime addicts (or about 12 % of Americans were addicted to an illicit drug at some time in their life---and 75% of this population (>20 M) cannot be found are still addicted or dead
 Remission in studies that include repeated, face-to-face interviews, back-up validation methods Does type of study matter?
Remission in studies that include repeated, face-to-face interviews, back-up validation methods Does type of study matter?
Addiction has a genetic basis. (2) You do") The logic behind the genetic argument: (1)Addiction has a genetic basis. (2) You do not choose your genes. (3) Therefore, drug use in addicts is involuntary (4) Sensible argument if voluntary behaviors do not have a biological basis But as this graph shows voluntary behavior has a genetic basis also (5) Yet…see graph
The logic behind the genetic argument: (1)Addiction has a genetic basis. (2) You do not choose your genes. (3) Therefore, drug use in addicts is involuntary (4) Sensible argument if voluntary behaviors do not have a biological basis But as this graph shows voluntary behavior has a genetic basis also (5) Yet…see graph
 Brain plasticity is inherent to all psychological phenomena, particularly learning and voluntary acts. That addiction is tied to changes in brain structure and function is what makes it, fundamentally, a disease. Alan Leshner, Science (1997) But all learning is tied to changes in brain structure and function…
Brain plasticity is inherent to all psychological phenomena, particularly learning and voluntary acts. That addiction is tied to changes in brain structure and function is what makes it, fundamentally, a disease. Alan Leshner, Science (1997) But all learning is tied to changes in brain structure and function…
 VVVVolkow et al. , Synapse, 1993, 14: 169 -177.
VVVVolkow et al. , Synapse, 1993, 14: 169 -177.
 Summary: In accordance with the idioms that distinguish addiction from chronic illnesses, research reveals Most addicts stop using drugs and usually do so without professional assistance The primary factors that bring drug use to a halt are those that influence decisions: familial concerns, economics, values We cannot make a similar summary for “chronic illnesses” Although addiction has a biological basis, these differences are important and too large to overlook: Thus, addiction, is not “Really like chronic diseases”
Summary: In accordance with the idioms that distinguish addiction from chronic illnesses, research reveals Most addicts stop using drugs and usually do so without professional assistance The primary factors that bring drug use to a halt are those that influence decisions: familial concerns, economics, values We cannot make a similar summary for “chronic illnesses” Although addiction has a biological basis, these differences are important and too large to overlook: Thus, addiction, is not “Really like chronic diseases”