

04f700d8da107131c9b2f5ad3a6ec5a7.ppt
- Количество слайдов: 90
 Getting Guidelines into Practice: Lessons Learned from Research Jenny Ploeg, RN, Ph. D Evidence-Informed Decision Making Workshop Mc. Master University May 4, 2011
Getting Guidelines into Practice: Lessons Learned from Research Jenny Ploeg, RN, Ph. D Evidence-Informed Decision Making Workshop Mc. Master University May 4, 2011
 Outline § Developing Guidelines § Appraising Guidelines § Implementing Guidelines § Sustaining Guidelines § Spreading Guidelines
Outline § Developing Guidelines § Appraising Guidelines § Implementing Guidelines § Sustaining Guidelines § Spreading Guidelines



 Question § What guidelines has your organization implemented? § What guidelines have you been involved in implementing?
Question § What guidelines has your organization implemented? § What guidelines have you been involved in implementing?
") Practice Guideline Evaluation and Adaptation Cycle (Graham et al, 2005)
Practice Guideline Evaluation and Adaptation Cycle (Graham et al, 2005)
 Sources of Guidelines § National Guideline Clearinghouse § Registered Nurses Association of Ontario § And many others
Sources of Guidelines § National Guideline Clearinghouse § Registered Nurses Association of Ontario § And many others
 RNAO Guidelines Program § Launched Nursing Best Practice Guidelines Program with funding from MOHLTC in 1999 § 42 published guidelines: English, French, Chinese, Italian, Japanese, Spanish § Guidelines for Personal Digital Assistants § Educator’s Resource § Toolkit for Implementation of Clinical Practice Guidelines
RNAO Guidelines Program § Launched Nursing Best Practice Guidelines Program with funding from MOHLTC in 1999 § 42 published guidelines: English, French, Chinese, Italian, Japanese, Spanish § Guidelines for Personal Digital Assistants § Educator’s Resource § Toolkit for Implementation of Clinical Practice Guidelines
 RNAO Guidelines Program § Best Practice Spotlight Organizations § Champions Program § Advanced Clinical/Practice Fellowships § Long-Term Care Best Practices Initiative § National Collaborative on Falls in LTC § Ph. D Fellowships
RNAO Guidelines Program § Best Practice Spotlight Organizations § Champions Program § Advanced Clinical/Practice Fellowships § Long-Term Care Best Practices Initiative § National Collaborative on Falls in LTC § Ph. D Fellowships
 Developing Guidelines RNAO Development Panel § Continence § Constipation Process of updating now, new evidence being integrated
Developing Guidelines RNAO Development Panel § Continence § Constipation Process of updating now, new evidence being integrated
 Levels of Evidence: RNAO § Ia Evidence from meta-analysis or systematic review of RCTs § Ib Evidence from at least 1 RCT § IIa Evidence from at least 1 well designed controlled study without randomization § IIb Evidence from at least 1 other type of welldesigned quasi-experimental study § III Evidence from well-designed nonexperimental descriptive studies (e. g, correlation studies, case studies) § IV Evidence from expert committee reports or opinions and/or clinical experience of respected
Levels of Evidence: RNAO § Ia Evidence from meta-analysis or systematic review of RCTs § Ib Evidence from at least 1 RCT § IIa Evidence from at least 1 well designed controlled study without randomization § IIb Evidence from at least 1 other type of welldesigned quasi-experimental study § III Evidence from well-designed nonexperimental descriptive studies (e. g, correlation studies, case studies) § IV Evidence from expert committee reports or opinions and/or clinical experience of respected
 §") Appraising Guidelines § AGREE II tool (Appraisal of Guidelines for Research and Evaluation) § Assesses methodological rigor and transparency in which a guideline is developed
Appraising Guidelines § AGREE II tool (Appraisal of Guidelines for Research and Evaluation) § Assesses methodological rigor and transparency in which a guideline is developed
 Appraising Guidelines 23 items in 6 domains § Domain 1: Scope and Purpose § Domain 2: Stakeholder Involvement § Domain 3: Rigour of Development § Domain 4: Clarity of Presentation § Domain 5: Applicability § Domain 6: Editorial Independence 7 -point scale: 1=strongly disagree, 7=strongly agree
Appraising Guidelines 23 items in 6 domains § Domain 1: Scope and Purpose § Domain 2: Stakeholder Involvement § Domain 3: Rigour of Development § Domain 4: Clarity of Presentation § Domain 5: Applicability § Domain 6: Editorial Independence 7 -point scale: 1=strongly disagree, 7=strongly agree
 Figure 1: The knowledge-to-action cycle Harrison, M. B. et al. CMAJ 2010; 182: E 78 -E 84 Copyright © 2010 Canadian Medical Association or its licensors
Figure 1: The knowledge-to-action cycle Harrison, M. B. et al. CMAJ 2010; 182: E 78 -E 84 Copyright © 2010 Canadian Medical Association or its licensors
 RNAO Toolkit § Toolkit for implementation of clinical practice guidelines
RNAO Toolkit § Toolkit for implementation of clinical practice guidelines
 § Environmental readiness (assessment form) §") Contents of Toolkit § Stakeholder engagement (assessment form) § Environmental readiness (assessment form) § Evaluation of CPG implementation and impact (indicator identification worksheet) § Human and financial resources (Budget worksheet) § Managing and monitoring implementation (action plan template)
Contents of Toolkit § Stakeholder engagement (assessment form) § Environmental readiness (assessment form) § Evaluation of CPG implementation and impact (indicator identification worksheet) § Human and financial resources (Budget worksheet) § Managing and monitoring implementation (action plan template)
. Evaluating best practice") Implementing Guidelines Edwards, Davies, Ploeg, Dobbins, Skelly, Griffin, Raphs. Thibodeau. (2005). Evaluating best practice guidelines. Canadian Nurse, 101, 19 -23.
Implementing Guidelines Edwards, Davies, Ploeg, Dobbins, Skelly, Griffin, Raphs. Thibodeau. (2005). Evaluating best practice guidelines. Canadian Nurse, 101, 19 -23.
 Facilitators: Questions From your experience, what are three most important factors that facilitate guideline implementation?
Facilitators: Questions From your experience, what are three most important factors that facilitate guideline implementation?
 Study: Facilitators and Barriers § Design: Before-after study with quantitative and qualitative data collection § Setting: 22 agencies in Ontario that implemented 7 RNAO best practice guidelines from 2000 -2001 (6 -9 month implementation period) Ploeg, Davies, Edwards, Gifford & Elliott Miller. (2007). Factors influencing best practice guideline implementation: Lessons learned from administrators, nursing staff and project leaders. Worldviews
Study: Facilitators and Barriers § Design: Before-after study with quantitative and qualitative data collection § Setting: 22 agencies in Ontario that implemented 7 RNAO best practice guidelines from 2000 -2001 (6 -9 month implementation period) Ploeg, Davies, Edwards, Gifford & Elliott Miller. (2007). Factors influencing best practice guideline implementation: Lessons learned from administrators, nursing staff and project leaders. Worldviews
 Study: Facilitators and Barriers Guidelines: § § § § Client Centered Care Crisis Intervention Healthy Adolescent Development Pain Assessment Pressure Ulcers Supporting and Strengthening Families Therapeutic Relationships
Study: Facilitators and Barriers Guidelines: § § § § Client Centered Care Crisis Intervention Healthy Adolescent Development Pain Assessment Pressure Ulcers Supporting and Strengthening Families Therapeutic Relationships
 Study: Facilitators and Barriers Data Collection: § Semi-structured audio-taped telephone interviews at end of guideline implementation Participants: § 8 Clinical Resource Nurses (Implementation leaders) § 58 Nurses and other care providers § 59 Administrators
Study: Facilitators and Barriers Data Collection: § Semi-structured audio-taped telephone interviews at end of guideline implementation Participants: § 8 Clinical Resource Nurses (Implementation leaders) § 58 Nurses and other care providers § 59 Administrators
 Facilitators Individual: § Learning about the guideline through small group interaction § Positive staff attitudes Organizational: § Leadership support § Champions § Teamwork and collaboration Environmental: § Professional association support § Inter-organizational collaboration and networks
Facilitators Individual: § Learning about the guideline through small group interaction § Positive staff attitudes Organizational: § Leadership support § Champions § Teamwork and collaboration Environmental: § Professional association support § Inter-organizational collaboration and networks
 Lessons Learned § Attend to factors at multiple levels: individual practitioner, social context, organizational and environmental contexts § Leadership support is key § Champions § Use of toolkits to help plan for implementation § Factors influencing implementation are interlinked in complex ways not yet fully
Lessons Learned § Attend to factors at multiple levels: individual practitioner, social context, organizational and environmental contexts § Leadership support is key § Champions § Use of toolkits to help plan for implementation § Factors influencing implementation are interlinked in complex ways not yet fully
 Sustaining
Sustaining
 Knowledge to Action from: Graham et al: Lost in Knowledge Translation: Time for a Map? Monitor knowledge use Select, tailor implement interventions Knowledge Creation Evaluate outcomes Knowledge inquiry e edg wl no gk Knowledge tools/ products Ta ilo rin Assess barriers to knowledge use Knowledge synthesis Adapt knowledge to local context Identify Problem Identify, Review Select knowledge http: //www. jcehp. com/vol 26/2601 graham 2006. pdf Sustain knowledge use
Knowledge to Action from: Graham et al: Lost in Knowledge Translation: Time for a Map? Monitor knowledge use Select, tailor implement interventions Knowledge Creation Evaluate outcomes Knowledge inquiry e edg wl no gk Knowledge tools/ products Ta ilo rin Assess barriers to knowledge use Knowledge synthesis Adapt knowledge to local context Identify Problem Identify, Review Select knowledge http: //www. jcehp. com/vol 26/2601 graham 2006. pdf Sustain knowledge use
 Sustainability: Questions § Has your organization been able to sustain the guideline after initial implementation? § What factors are most important for sustainability of guidelines?
Sustainability: Questions § Has your organization been able to sustain the guideline after initial implementation? § What factors are most important for sustainability of guidelines?
 Why is sustainability planning rarely addressed in research? § Only 2 of 1000 sources screened for a literature review about the diffusion of innovations in health service organisations included the term sustainability (Greenhalgh et al. , 2005) § Shorter-term perspectives are the focus of health services research, possibly due to: – Limited availability of long-term funding – Different time perspectives of policy cycles across health care sectors – Disengagement of project leaders towards the end of projects
Why is sustainability planning rarely addressed in research? § Only 2 of 1000 sources screened for a literature review about the diffusion of innovations in health service organisations included the term sustainability (Greenhalgh et al. , 2005) § Shorter-term perspectives are the focus of health services research, possibly due to: – Limited availability of long-term funding – Different time perspectives of policy cycles across health care sectors – Disengagement of project leaders towards the end of projects
 Investigators: § Barbara Davies §") Study: Determinants of the Sustained Use of Research (SURE) Investigators: § Barbara Davies § Nancy Edwards § Jenny Ploeg § Evangeline Danseco § Tazim Virani § Maureen Dobbins Project Coordinator: § Cindy Versteeg Partners: § RNAO § Canadian Nurses Association Funders: CIHR and CHSRF
Study: Determinants of the Sustained Use of Research (SURE) Investigators: § Barbara Davies § Nancy Edwards § Jenny Ploeg § Evangeline Danseco § Tazim Virani § Maureen Dobbins Project Coordinator: § Cindy Versteeg Partners: § RNAO § Canadian Nurses Association Funders: CIHR and CHSRF
 Sustainability § The degree to which an innovation continues to be used after initial efforts to secure adoption are completed (Rogers, 2003) § When new ways of working become the norm (Maher et al, 2007)
Sustainability § The degree to which an innovation continues to be used after initial efforts to secure adoption are completed (Rogers, 2003) § When new ways of working become the norm (Maher et al, 2007)
 The Issue § Up to 70% failure rate for organizational change and 30% for health care change (Maher, et al. 2010) § First 17 RNAO guidelines implemented from 2000 -2004 § Six-month pilot implementation process, funded by MOHLTC § Once the initial pilot implementation funding is over, do nurses, managers and senior executives continue to implement guideline recommendations?
The Issue § Up to 70% failure rate for organizational change and 30% for health care change (Maher, et al. 2010) § First 17 RNAO guidelines implemented from 2000 -2004 § Six-month pilot implementation process, funded by MOHLTC § Once the initial pilot implementation funding is over, do nurses, managers and senior executives continue to implement guideline recommendations?
") The Topics Cycle 1 § Falls § Continence § Constipation § Pressure ulcers (Assessment) Cycle 2 § Healthy adolescents § Client centered care § Crisis intervention § Pain § Therapeutic relationships § Pressure ulcers (management) § Supporting families Cycle 3 § Adult asthma control § Breastfeeding § Screening for delirium, dementia and depression § Smoking cessation § Reducing foot complications for people with diabetes § Venous leg ulcers
The Topics Cycle 1 § Falls § Continence § Constipation § Pressure ulcers (Assessment) Cycle 2 § Healthy adolescents § Client centered care § Crisis intervention § Pain § Therapeutic relationships § Pressure ulcers (management) § Supporting families Cycle 3 § Adult asthma control § Breastfeeding § Screening for delirium, dementia and depression § Smoking cessation § Reducing foot complications for people with diabetes § Venous leg ulcers
 hospital, LTC, community 92% Decision-makers (112/122) 80% Nurses") Results Participation rate: 90% Organizations (37/41) hospital, LTC, community 92% Decision-makers (112/122) 80% Nurses (77/96)
Results Participation rate: 90% Organizations (37/41) hospital, LTC, community 92% Decision-makers (112/122) 80% Nurses (77/96)
 Sustainability Status at Year 2
Sustainability Status at Year 2
; Of the 16 sustained, 11") Sustainability Status at Year 2 § 43% Sustained (16/37); Of the 16 sustained, 11 (30%) expanded § 57% Not sustained (21/37); Most not sustained in the first and second cohorts (81%)
Sustainability Status at Year 2 § 43% Sustained (16/37); Of the 16 sustained, 11 (30%) expanded § 57% Not sustained (21/37); Most not sustained in the first and second cohorts (81%)
 §") Sustainability Status at Year 3 § 59% sustained or sustained and expanded (22/37) § Organizations not sustaining at Year 2, likely not to sustain at Year 3 (9/12 or 75%) § Organizations sustaining and expanding at Year 2, likely to sustain at Year 3 (10/11 or 91%)
Sustainability Status at Year 3 § 59% sustained or sustained and expanded (22/37) § Organizations not sustaining at Year 2, likely not to sustain at Year 3 (9/12 or 75%) § Organizations sustaining and expanding at Year 2, likely to sustain at Year 3 (10/11 or 91%)
 Facilitators for Sustained or Expanded Long-Term Use of Guidelines § § Leadership by champions Management support at all levels Ongoing staff education Guideline integrated into policies and procedures § Staff buy-in and ownership § Synergy with partners and external influences § Guideline characteristics
Facilitators for Sustained or Expanded Long-Term Use of Guidelines § § Leadership by champions Management support at all levels Ongoing staff education Guideline integrated into policies and procedures § Staff buy-in and ownership § Synergy with partners and external influences § Guideline characteristics
 Implications To ensure sustainability, we need: § Ongoing and supportive leadership § Management support § Continuing education § Organizational culture to support evidence -informed practice § Integration of guideline recommendations into organizational policies, procedures, documentation
Implications To ensure sustainability, we need: § Ongoing and supportive leadership § Management support § Continuing education § Organizational culture to support evidence -informed practice § Integration of guideline recommendations into organizational policies, procedures, documentation
 Implications § Administrators and managers need to visibly support the guideline through provision of resources and staff education § Staff education on guidelines needs to be ongoing § Managers need to ensure there is funding for staff education and time for staff to attend education sessions during regular work hours § Guideline recommendations can be integrated into staff orientation and other professional development programs
Implications § Administrators and managers need to visibly support the guideline through provision of resources and staff education § Staff education on guidelines needs to be ongoing § Managers need to ensure there is funding for staff education and time for staff to attend education sessions during regular work hours § Guideline recommendations can be integrated into staff orientation and other professional development programs
 SURE Study Conclusions § Implementing changes in nursing practice to be more evidence-based takes time, is dynamic, long-term and iterative process § Some organizations may take 2 -3 years to show that guideline recommendations are routine part of nursing practice § Full Report: CHSRF http: //chsrf. ca/final_research/ogc/pdf/davies_final _e. pdf
SURE Study Conclusions § Implementing changes in nursing practice to be more evidence-based takes time, is dynamic, long-term and iterative process § Some organizations may take 2 -3 years to show that guideline recommendations are routine part of nursing practice § Full Report: CHSRF http: //chsrf. ca/final_research/ogc/pdf/davies_final _e. pdf
 Spread § Kudzu: vine that was introduced to the US from Japan in 1876 § One of fastest growing vines § Now covers over 7 million acres in Southwestern US § Grows as much as a foot per day in summer, climbs trees, power poles, homes § Can grow 60 feet per year
Spread § Kudzu: vine that was introduced to the US from Japan in 1876 § One of fastest growing vines § Now covers over 7 million acres in Southwestern US § Grows as much as a foot per day in summer, climbs trees, power poles, homes § Can grow 60 feet per year

 Co-Principal Investigators Nancy Edwards, RN, Ph.") Research, Exchange and Impact for System Support (REISS) Co-Principal Investigators Nancy Edwards, RN, Ph. D, FCAHS. Professor, University of Ottawa Doris Grinspun, RN, MSN, Ph. D, O. ONT. Executive Director, Registered Nurses’ Association of Ontario
Research, Exchange and Impact for System Support (REISS) Co-Principal Investigators Nancy Edwards, RN, Ph. D, FCAHS. Professor, University of Ottawa Doris Grinspun, RN, MSN, Ph. D, O. ONT. Executive Director, Registered Nurses’ Association of Ontario
 REISS Research Co. Investigators Angela Downey Associate Professor, University of Victoria Tazim Virani Principal, Tazim Virani and Associates Ali Dastmalchian Professor & Dean, Faculty of Business, University of Victoria Ian Graham Associate Professor, University of Ottawa Irmajean Bajnok Director, IABPG Program & CPNE, Registered Nurses Association of Ontario Ariella Lang Research Scientist, VON Canada Whitney Berta Associate Professor, University of Toronto Heather Mc. Connell Associate Director, IABPG Program, Registered Nurses Association of Ontario Sheila Block Registered Nurses Association of Ontario Ann Lynch Associate Director General of Clinical Operations, MUHC Barbara Davies Professor, University of Ottawa Patricia Marck Associate Professor, University of Alberta Kathryn Higuchi Associate Professor, University of Ottawa Cecile Michaud Associate Professor, Université de Sherbrooke, Campus de Longueil Jenny Ploeg Associate Professor, Mc. Master University Suresh Kalagnanam Associate Professor, Jennifer Skelly Associate Professor, Mc. Master University Kim Jarvi Judith Ritchie Associate Director for Nursing University of Saskatchewan Senior Economist, Registered Nurses Association of Ontario
REISS Research Co. Investigators Angela Downey Associate Professor, University of Victoria Tazim Virani Principal, Tazim Virani and Associates Ali Dastmalchian Professor & Dean, Faculty of Business, University of Victoria Ian Graham Associate Professor, University of Ottawa Irmajean Bajnok Director, IABPG Program & CPNE, Registered Nurses Association of Ontario Ariella Lang Research Scientist, VON Canada Whitney Berta Associate Professor, University of Toronto Heather Mc. Connell Associate Director, IABPG Program, Registered Nurses Association of Ontario Sheila Block Registered Nurses Association of Ontario Ann Lynch Associate Director General of Clinical Operations, MUHC Barbara Davies Professor, University of Ottawa Patricia Marck Associate Professor, University of Alberta Kathryn Higuchi Associate Professor, University of Ottawa Cecile Michaud Associate Professor, Université de Sherbrooke, Campus de Longueil Jenny Ploeg Associate Professor, Mc. Master University Suresh Kalagnanam Associate Professor, Jennifer Skelly Associate Professor, Mc. Master University Kim Jarvi Judith Ritchie Associate Director for Nursing University of Saskatchewan Senior Economist, Registered Nurses Association of Ontario
 REISS: 5 Projects 1. Champions Promoting the Use of Best Practice Guidelines 2. Early Steps In Innovation: What Takes a Good Idea Further? – early postpartum discharge – minimal restraint use – needle-exchange program 3. Spreading Innovation 4. Improving Communication to Improve Long Term Care 5. What Drives Cost and Enhances Benefits Project summaries available: Nursing Best Practice Research Unit
REISS: 5 Projects 1. Champions Promoting the Use of Best Practice Guidelines 2. Early Steps In Innovation: What Takes a Good Idea Further? – early postpartum discharge – minimal restraint use – needle-exchange program 3. Spreading Innovation 4. Improving Communication to Improve Long Term Care 5. What Drives Cost and Enhances Benefits Project summaries available: Nursing Best Practice Research Unit
 Project 1: Best Practice Champions Ploeg, J. , Skelly, J. , Rowan, M. , Edwards, N. , Davies, B. , Grinspun, D. , Bajnok, I. , Downey, A. (2010). The role of nursing best practice champions in diffusing practice guidelines: A mixed methods study. Worldviews on Evidence Based Nursing, 7, 238251. doi: 10. 1111/j. 17416787. 2010. 00202. x
Project 1: Best Practice Champions Ploeg, J. , Skelly, J. , Rowan, M. , Edwards, N. , Davies, B. , Grinspun, D. , Bajnok, I. , Downey, A. (2010). The role of nursing best practice champions in diffusing practice guidelines: A mixed methods study. Worldviews on Evidence Based Nursing, 7, 238251. doi: 10. 1111/j. 17416787. 2010. 00202. x
 Background Definition of Champions: individuals who dedicate themselves to supporting, marketing, and driving through an innovation (Greenhalgh et al. , 2005) Variety of terms used: change agents, opinion leaders, facilitators, linking agents, product champions, best practice champions Over 3, 000 champions trained by RNAO since 1999
Background Definition of Champions: individuals who dedicate themselves to supporting, marketing, and driving through an innovation (Greenhalgh et al. , 2005) Variety of terms used: change agents, opinion leaders, facilitators, linking agents, product champions, best practice champions Over 3, 000 champions trained by RNAO since 1999
 Background “Knowing how champions contribute to projects is critical to understanding, managing, and facilitating innovation and to training others how to champion projects” (Markham, 1998) § Little research on Nursing Best Practice Champions: roles, activities and factors influencing their role § Research evidence of impact is mixed, nature of role remains unclear § Most research conducted in acute care settings
Background “Knowing how champions contribute to projects is critical to understanding, managing, and facilitating innovation and to training others how to champion projects” (Markham, 1998) § Little research on Nursing Best Practice Champions: roles, activities and factors influencing their role § Research evidence of impact is mixed, nature of role remains unclear § Most research conducted in acute care settings
 Research Questions § How do Nursing Best Practice Champions influence the diffusion of BPG recommendations? § What factors influence the role of Nursing Best Practice Champions?
Research Questions § How do Nursing Best Practice Champions influence the diffusion of BPG recommendations? § What factors influence the role of Nursing Best Practice Champions?
 Design Figure 1. Study Design: Mixed Methods Sequential Triangulation Design Phase 1 Phase 2 QUAN QUAL data collection QUAL results Develop survey instrument QUAN data collection Interpretation QUAL + QUAN Note: QUAL: Qualitative; QUAN: Quantitative QUAN data analysis QUAN results
Design Figure 1. Study Design: Mixed Methods Sequential Triangulation Design Phase 1 Phase 2 QUAN QUAL data collection QUAL results Develop survey instrument QUAN data collection Interpretation QUAL + QUAN Note: QUAL: Qualitative; QUAN: Quantitative QUAN data analysis QUAN results
 Champions Quantitative Survey § 191/885 (21. 6%)") Participants Qualitative Interviews § 23/26 (88. 5%) Champions Quantitative Survey § 191/885 (21. 6%) Champions § 41/110 (37. 3%) Administrators
Participants Qualitative Interviews § 23/26 (88. 5%) Champions Quantitative Survey § 191/885 (21. 6%) Champions § 41/110 (37. 3%) Administrators
 Participants: Healthcare Sector
Participants: Healthcare Sector
 Participants: Position
Participants: Position
 Findings Champions: § hold multidimensional roles: educator, facilitator, mentor, leader, policy developer, evaluator § are active knowledge disseminators of clinical information to nurses § work with various disciplines in all types and levels of positions to explain, convince and help ensure guideline implementation
Findings Champions: § hold multidimensional roles: educator, facilitator, mentor, leader, policy developer, evaluator § are active knowledge disseminators of clinical information to nurses § work with various disciplines in all types and levels of positions to explain, convince and help ensure guideline implementation
 Findings Champions: § use many strategies at multiple organizational levels § attend to various stakeholder groups § tailor diffusion strategies to organizational context
Findings Champions: § use many strategies at multiple organizational levels § attend to various stakeholder groups § tailor diffusion strategies to organizational context
 Diffusion Strategies of Champions 1. Dissemination of information about clinical practice guidelines – Education and awareness – Acting as a resource to support and mentor nurses 2. Champions as persuasive practice leaders – Working through committees – Participating in and leading interdisciplinary teams 3. Tailoring the guideline implementation strategies to the organizational context – Exploring, auditing, monitoring of best practices – Documentation changes to incorporate best practice recommendations
Diffusion Strategies of Champions 1. Dissemination of information about clinical practice guidelines – Education and awareness – Acting as a resource to support and mentor nurses 2. Champions as persuasive practice leaders – Working through committees – Participating in and leading interdisciplinary teams 3. Tailoring the guideline implementation strategies to the organizational context – Exploring, auditing, monitoring of best practices – Documentation changes to incorporate best practice recommendations
 Spread Within Organization by Setting
Spread Within Organization by Setting
 Spread Beyond Organization by Setting
Spread Beyond Organization by Setting
 Factors Associated with Spread: Logistic Regression Analysis § Spread from a unit/team within an organization was dependent on the success of the implementation strategies § For every 1 unit ↑ in success of implementation you are 2. 0 times as likely to have a BPG spread beyond a unit or team § Spread outside the organization was dependent on the extent of change in team unit practices § For every 1 unit ↑ in extent of change you are 6. 8 times as likely to have a BPG spread beyond the organization
Factors Associated with Spread: Logistic Regression Analysis § Spread from a unit/team within an organization was dependent on the success of the implementation strategies § For every 1 unit ↑ in success of implementation you are 2. 0 times as likely to have a BPG spread beyond a unit or team § Spread outside the organization was dependent on the extent of change in team unit practices § For every 1 unit ↑ in extent of change you are 6. 8 times as likely to have a BPG spread beyond the organization
 Discussion § Champions hold multiple roles: facilitator, change agent, knowledge translator § Champions are persuasive practice leaders, work with many disciplines § Champions work through complex web of committees and working groups § Champions are adaptors who tailor BPG implementation strategies to organizational context
Discussion § Champions hold multiple roles: facilitator, change agent, knowledge translator § Champions are persuasive practice leaders, work with many disciplines § Champions work through complex web of committees and working groups § Champions are adaptors who tailor BPG implementation strategies to organizational context
 Implications § Adequate and ongoing training to maximize potential of champions role and impact § Broad range of knowledge and skills: knowledge transfer, policy development, research and evaluation, leadership, mentorship
Implications § Adequate and ongoing training to maximize potential of champions role and impact § Broad range of knowledge and skills: knowledge transfer, policy development, research and evaluation, leadership, mentorship
 Future Research § What criteria should be used to select champions? § Are characteristics of champions associated with effectiveness? (e. g. , position, credibility, experience) § Examine power, span of control, authority of champions § What organizational supports are required for success of champions’ role? § What constitutes a ‘critical mass’ of champions? § What is the impact of champions?
Future Research § What criteria should be used to select champions? § Are characteristics of champions associated with effectiveness? (e. g. , position, credibility, experience) § Examine power, span of control, authority of champions § What organizational supports are required for success of champions’ role? § What constitutes a ‘critical mass’ of champions? § What is the impact of champions?
 Study 3: Spreading Innovation – The Best Routes to Best Practices Barbara Davies, Judith Ritchie and team What We Studied: Examined naturally occurring diffusion of guidelines - how practice guidelines spread within and between organizations under normal, everyday conditions. Phase 1: We created diagrams to map how innovations spread within and outside an organization, two years after implementation of an RNAO BPG. Phase 2: We then visited 2 sites 7 -10 years after
Study 3: Spreading Innovation – The Best Routes to Best Practices Barbara Davies, Judith Ritchie and team What We Studied: Examined naturally occurring diffusion of guidelines - how practice guidelines spread within and between organizations under normal, everyday conditions. Phase 1: We created diagrams to map how innovations spread within and outside an organization, two years after implementation of an RNAO BPG. Phase 2: We then visited 2 sites 7 -10 years after
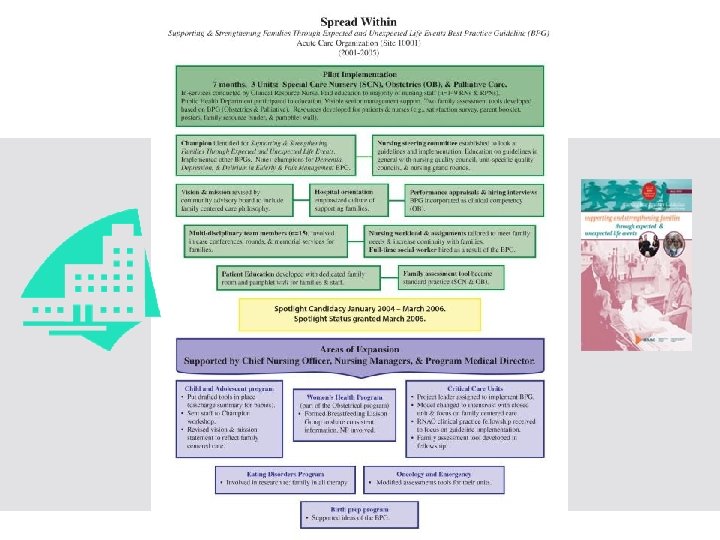
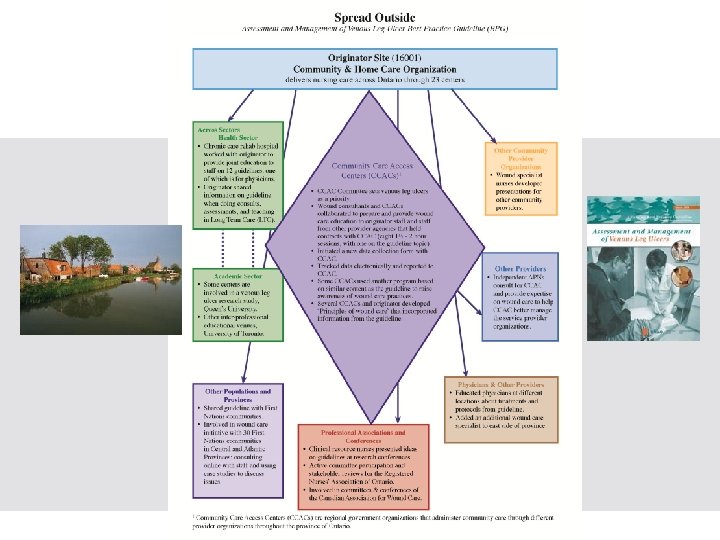
 Results Phase 1: § Spread diagrams revealed the dynamic and non -linear processes occurring in organizations as they adaptively facilitated the spread of a guideline. § Most sites, except for a community care site, had a higher level of internal organizational) spread than external spread.
Results Phase 1: § Spread diagrams revealed the dynamic and non -linear processes occurring in organizations as they adaptively facilitated the spread of a guideline. § Most sites, except for a community care site, had a higher level of internal organizational) spread than external spread.
 § Initially funding was allocated to guideline implementation but currently") Phase 2 Hospital (Acute) § Initially funding was allocated to guideline implementation but currently “in-kind” implementation is ongoing § Guideline implementation of the index topic (supporting families ) continues to be sustained 10 years later
Phase 2 Hospital (Acute) § Initially funding was allocated to guideline implementation but currently “in-kind” implementation is ongoing § Guideline implementation of the index topic (supporting families ) continues to be sustained 10 years later
 Phase 2 Community Home Visiting § Guideline implementation of the index topic (venous leg ulcers) continues to be sustained 7 years later § Challenges, some of the guideline-based requests to the case managers at the funders (CCACs) are not supported. § The spread diagram was modified to reflect the central and multi-faceted “political funding support/interference process” of the CCACs in a diamond shape box.
Phase 2 Community Home Visiting § Guideline implementation of the index topic (venous leg ulcers) continues to be sustained 7 years later § Challenges, some of the guideline-based requests to the case managers at the funders (CCACs) are not supported. § The spread diagram was modified to reflect the central and multi-faceted “political funding support/interference process” of the CCACs in a diamond shape box.
 Lessons Learned Takes a combination of strategies: learning opportunities, champions, discussion, communicating goals Frontline workers “deeply involved” to figure out barriers and ways around them Strong leadership at every level to align vision, goals + activities RNAO guidelines were sustained 7 to 10 years later “Absolutely better” to be a patient at the hospital now than 10 years earlier
Lessons Learned Takes a combination of strategies: learning opportunities, champions, discussion, communicating goals Frontline workers “deeply involved” to figure out barriers and ways around them Strong leadership at every level to align vision, goals + activities RNAO guidelines were sustained 7 to 10 years later “Absolutely better” to be a patient at the hospital now than 10 years earlier
 Implications Sustaining evidence-informed innovations for the long term depends on full engagement of leaders and staff in their implementation. When people feel involved, they will see its value and benefits and stick with it in the long term.
Implications Sustaining evidence-informed innovations for the long term depends on full engagement of leaders and staff in their implementation. When people feel involved, they will see its value and benefits and stick with it in the long term.
 Overall Program of Research: Model
Overall Program of Research: Model
 Guideline Implementation for Improved Client/patient Outcomes: A longitudinal multi-site study GICOM Academic Investigators 1. Nursing, u. Ottawa: Barbara Davies, Kathryn Higuchi, Mary Ann Murray, Jackie Ellis 2. Nursing, Mc. Master University: Sandra Ireland, Jenny Ploeg 3. Clinical Epidemiology Unit, Ottawa Hospital Research Institute: Monica Taljaard
Guideline Implementation for Improved Client/patient Outcomes: A longitudinal multi-site study GICOM Academic Investigators 1. Nursing, u. Ottawa: Barbara Davies, Kathryn Higuchi, Mary Ann Murray, Jackie Ellis 2. Nursing, Mc. Master University: Sandra Ireland, Jenny Ploeg 3. Clinical Epidemiology Unit, Ottawa Hospital Research Institute: Monica Taljaard
 Ø Formal three year partnership with RNAO Ø Focus") BPSO Candidates -2009 -2012 (16) Ø Formal three year partnership with RNAO Ø Focus on enhancing their evidence based nursing practice cultures, and quality outcomes. Ø RNAO continues to work with the BPSOs to create strategies for sustainability and system-wide spread. GICOM settings (9) Acute Teaching Hospital: 2 Community health centre: 1 Home care Nursing: 2 Long-term care: 1 Rehabilitation care: 1
BPSO Candidates -2009 -2012 (16) Ø Formal three year partnership with RNAO Ø Focus on enhancing their evidence based nursing practice cultures, and quality outcomes. Ø RNAO continues to work with the BPSOs to create strategies for sustainability and system-wide spread. GICOM settings (9) Acute Teaching Hospital: 2 Community health centre: 1 Home care Nursing: 2 Long-term care: 1 Rehabilitation care: 1
 NHS sustainability model: A promising developing model § Initiated because sustainability was a problem § Aim to identify key factors which support or hinder sustainability of improvement initiatives § Create a model that practitioners could use to assess the likelihood of sustainability § Using a Bayesian approach 250 experts identified measures, created factors and estimated the diagnostic power of the factor levels § Reported as easy to use § Model being used in England, USA, Sweden and Norway
NHS sustainability model: A promising developing model § Initiated because sustainability was a problem § Aim to identify key factors which support or hinder sustainability of improvement initiatives § Create a model that practitioners could use to assess the likelihood of sustainability § Using a Bayesian approach 250 experts identified measures, created factors and estimated the diagnostic power of the factor levels § Reported as easy to use § Model being used in England, USA, Sweden and Norway
 Sustainability Model (Maher L, Gustafson D, Evans A. NHS Institute for Innovation and Improvement 2010) Monitoring progress Training and involvement Behaviors Adaptability Staff Credibility of benefits Senior leaders Process Clinical leaders Organization Benefits beyond helping patients Fit with goals and culture Infrastructure www. institute. nhs. uk/sustainability
Sustainability Model (Maher L, Gustafson D, Evans A. NHS Institute for Innovation and Improvement 2010) Monitoring progress Training and involvement Behaviors Adaptability Staff Credibility of benefits Senior leaders Process Clinical leaders Organization Benefits beyond helping patients Fit with goals and culture Infrastructure www. institute. nhs. uk/sustainability
 Outcomes § Need for more focus on outcomes of implementing and sustaining and spreading guidelines at multiple levels
Outcomes § Need for more focus on outcomes of implementing and sustaining and spreading guidelines at multiple levels
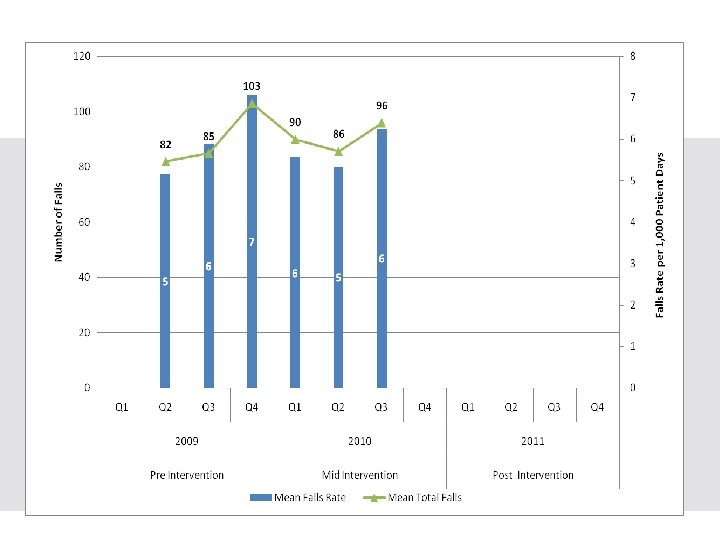
 Implementation of a Falls Prevention Guideline Across the Hamilton Niagara Haldimand Brant Local Health Integration Network: A Longitudinal Study Jenny Ploeg, Mc. Master University Sandra Ireland, Hamilton Health Sciences Barbara Davies, University of Ottawa Kathy Higuchi, University of Ottawa Mary Ann Murray, University of Ottawa Karen Cziraki, Hamilton Niagara Haldimand Brant Local Health Integration Network Nancy Fram, Hamilton Health Sciences Helen Kirkpatrick, St. Joseph’s Healthcare Hamilton Aleksandra Zecevic, University of
Implementation of a Falls Prevention Guideline Across the Hamilton Niagara Haldimand Brant Local Health Integration Network: A Longitudinal Study Jenny Ploeg, Mc. Master University Sandra Ireland, Hamilton Health Sciences Barbara Davies, University of Ottawa Kathy Higuchi, University of Ottawa Mary Ann Murray, University of Ottawa Karen Cziraki, Hamilton Niagara Haldimand Brant Local Health Integration Network Nancy Fram, Hamilton Health Sciences Helen Kirkpatrick, St. Joseph’s Healthcare Hamilton Aleksandra Zecevic, University of
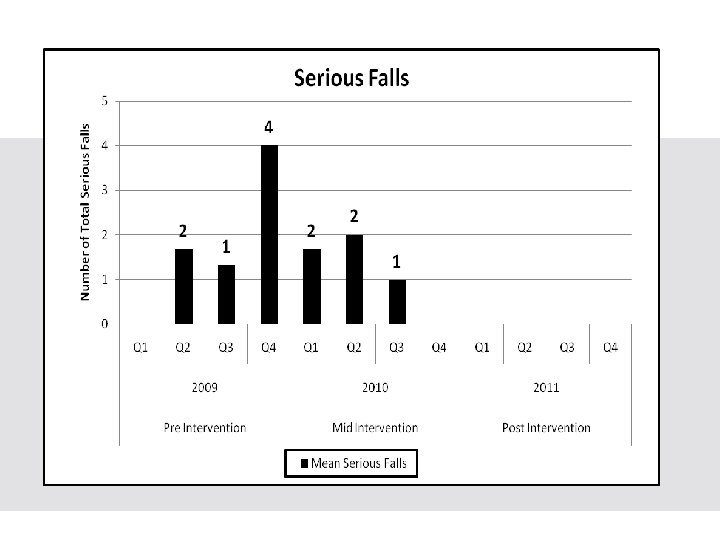
 Research Questions 1. What are the fall rates and total number of serious falls at three community hospitals providing acute care services within the LHIN before, during and after a mentored implementation of the RNAO Prevention of Falls and Fall Injuries in the Older Adult Best Practice Guideline? 2. What is the projected economic benefit to the LHIN of reducing serious falls (i. e. , those resulting in injury) at three community
Research Questions 1. What are the fall rates and total number of serious falls at three community hospitals providing acute care services within the LHIN before, during and after a mentored implementation of the RNAO Prevention of Falls and Fall Injuries in the Older Adult Best Practice Guideline? 2. What is the projected economic benefit to the LHIN of reducing serious falls (i. e. , those resulting in injury) at three community
 Research Questions 3. What are the experiences of project leaders and decision-makers in community hospitals related to implementing and sustaining a falls prevention guideline? (e. g. , strategies used to assist nurses and other health professionals to achieve improvement in fall outcomes; lessons learned in providing feedback related to fall outcomes) 4. What barriers and supports are encountered when implementing and sustaining strategies to improve patient fall-related outcomes over
Research Questions 3. What are the experiences of project leaders and decision-makers in community hospitals related to implementing and sustaining a falls prevention guideline? (e. g. , strategies used to assist nurses and other health professionals to achieve improvement in fall outcomes; lessons learned in providing feedback related to fall outcomes) 4. What barriers and supports are encountered when implementing and sustaining strategies to improve patient fall-related outcomes over
 Sustainability Scores for Site 1
Sustainability Scores for Site 1
 Challenges § Agreement on common definition of a serious fall § Difficulty experienced by participants in using the NHS survey § Competing pressures and limited resources within sites § Variable stages of implementation of the Falls BPG at baseline
Challenges § Agreement on common definition of a serious fall § Difficulty experienced by participants in using the NHS survey § Competing pressures and limited resources within sites § Variable stages of implementation of the Falls BPG at baseline
 For details and other publications visit § www. nbpru. ca § www. rnao. org
For details and other publications visit § www. nbpru. ca § www. rnao. org

 Thank you: Questions? Contact: Dr. Jenny Ploeg Email: ploegj@mcmaster. ca Dr. Ploeg is a MOHLTC mid career nursing research award recipient
Thank you: Questions? Contact: Dr. Jenny Ploeg Email: ploegj@mcmaster. ca Dr. Ploeg is a MOHLTC mid career nursing research award recipient