
Gastric Cancer Prepared by: student of 15-007-1 group


Gastric Cancer Prepared by: student of 15-007-1 group Asan Sandugash Checked by: Rahmanova A.M

GASTRIC TUMOURS Anatomy of the stomach Aetiology of Gastric cancer Types of Gastric cancer Pathology of Gastric Cancer Treatment of Gastric Cancer

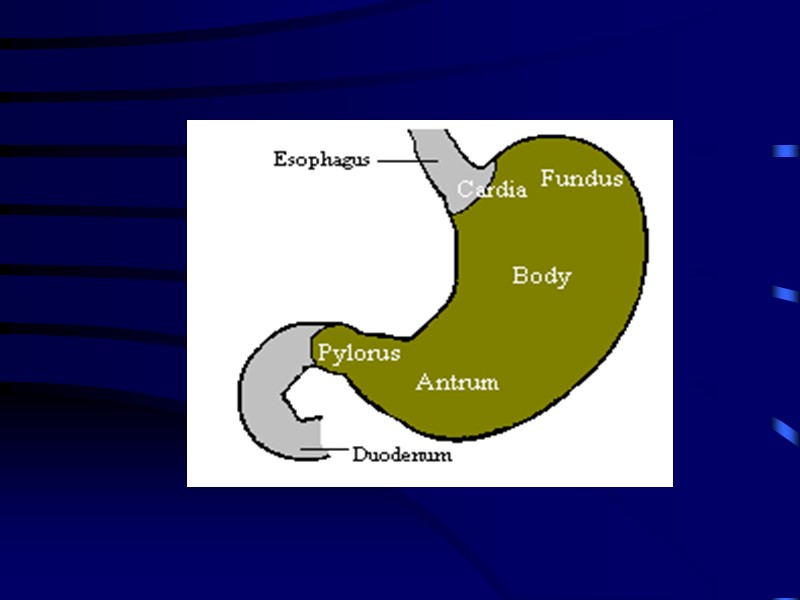
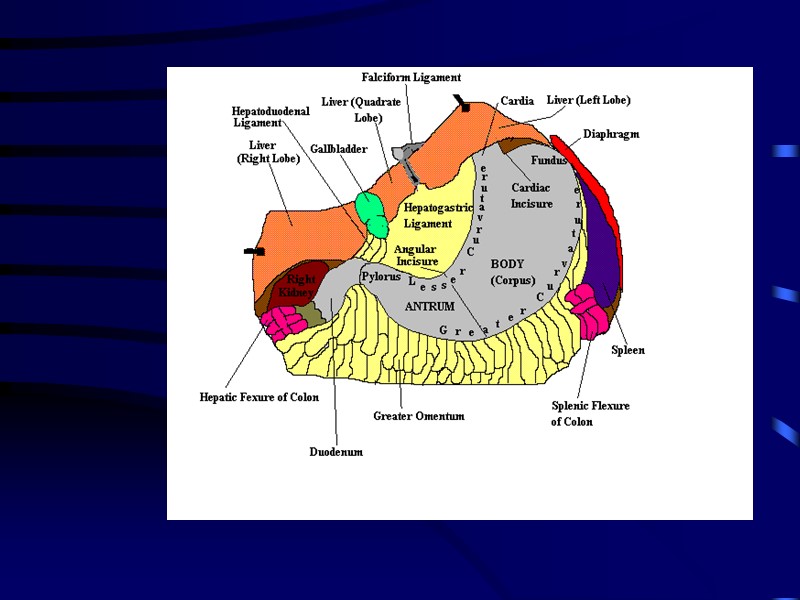
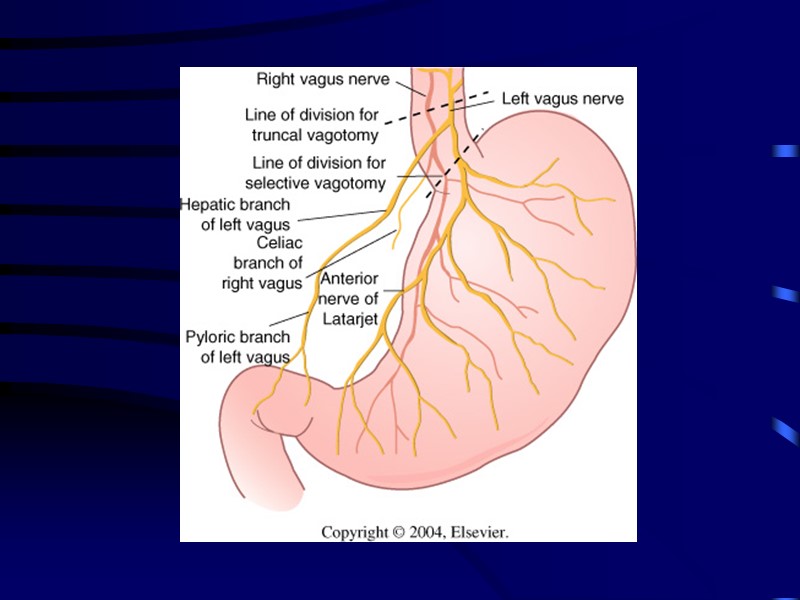
ANATOMY: The stomach J-shaped. The stomach has two surfaces (the anterior & posterior), two curvatures (the greater & lesser), two orifices (the cardia & pylorus). It has fundus, body and pyloric antrum.

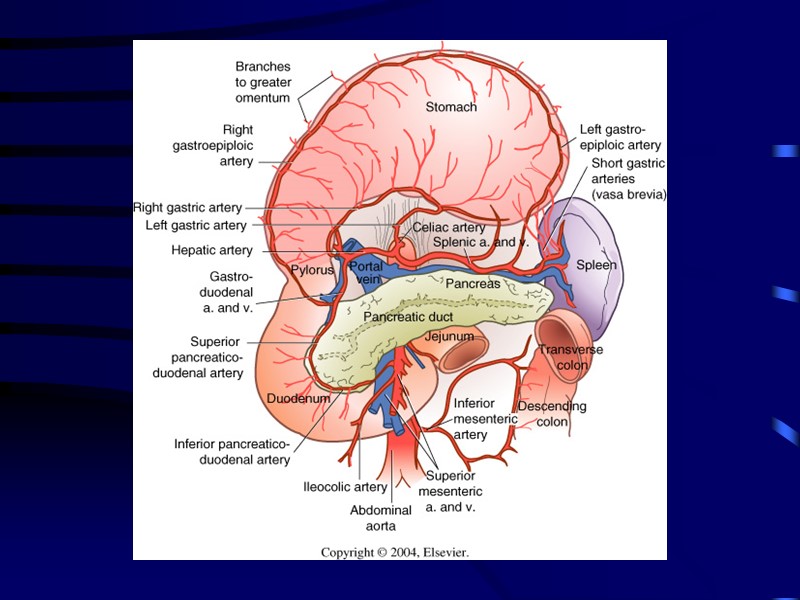
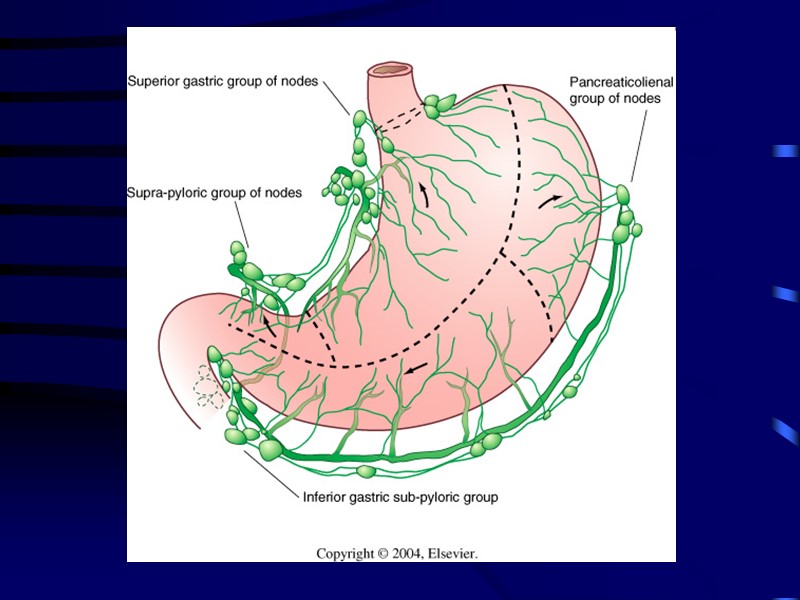
BLOOD SUPPLY: a. The left gastric artery b. Right gastric artery c. Right gastro-epiploic artery d. Left gastro-epiploic artery e. Short gastric arteries The corresponding veins drain into portal system. The lymphatic drainage of the stomach corresponding its blood supply.

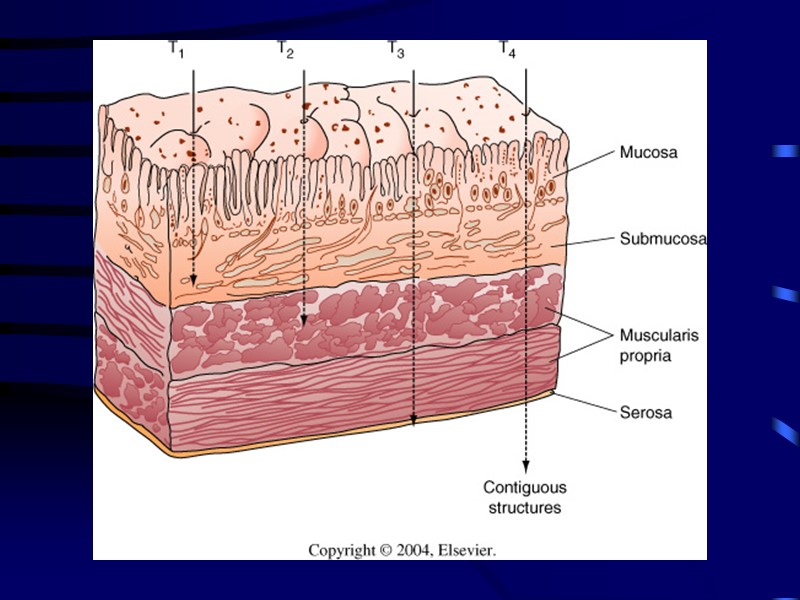
Anatomy Stomach has five layers: Mucosa Epithelium, lamina propria, and muscularis mucosae* Submucosa Smooth muscle layer Subserosa Serosa


AETIOLOGY: Gastric cancer is the second most common fatal cancer in the world with high frequency in Japan. The disease presents most commonly in the 5th and 6th decades of life and affect males twice as often as females. Contn…

The cause of the disease multistep process but several predisposing factors attributed to cause the disease : a. Environment e. Atrophic gastritis b. Diet f. Chronic gastric ulcer c. Heredity g. Adenomatous polyps d. Achlorhydria h. Blood group A i. H. Pyloric colonisation

TYPES OF GASTRIC CANCER: A. Benign Tumours B. Malignant Tumours

TYPES OF GASTRIC CANCER: A. Benign Tumours B. Malignant Tumours

THE BENIGN TUMORS: Although benign tumors can occur in the stomach most gastric tumours are malignant.

The benign groups includes:- 1. Non-neoplastic gastric polyps 2. Adenomas 3. Neoplastic gastric polyps 4. Smooth muscles tumours benign (Leiomyomas) 5. Polyposis Syndrome (eg:- Polyposis coli, Juvenile polyps and P.J. Syndrome) 6. Other benign tumours are fibromas, neurofibromas, aberrat pancreas and angiomas.
")
PATHOLOGY OF GASTRIC (MALIGNANT) TUMOURS: The gastric cancer may arise in the antrum (50%), the gastric body (30%), the fundus or oesophago-gastric juntion (20%).

Types of Malignant Tumours: a. Adenocarcinoma b. Leiomyosarcoma c. Lymphomas d. Carcinoid Tumours

1. Polypoid or Proliferative 2. Ulcerating 3. Ulcerating/Infiltrating 4. Diffuse Infiltrating (Linnitus- Plastica) The macroscopic forms of gastric cancers are classified by (Bormann classification) into:-

Early Gastric Cancer: Defined as cancer which is confined to the mucosa and submucosa regard- less of lymph nodes status. Advanced Gastric Cancer: Defined as tumor that has involved the muscularis propria of the stomach wall.

SPREAD OF GASTRIC CANCER: The diffuse type spreads rapidly through the submucosal and serosal lymphatic and penetrates the gastric wall at early stage, the intestinal variety remains localized for a while and has less tendency to disseminate. The spread by: 1. Direct (loco regional) 2. Lymphatic 3. Blood (Haematogenous) 4. Transcoelomic

Clinical Manifestation: Weight loss due to anorexia and early satiety is the most common symptoms Abdominal pain (not severe) common Nausea / vomiting Chronic occult blood loss is common; GIT bleeding (5%) Dysphagia (cardia involvement)

Clinical Manifestation: Paraneoplastic syndromes ( Trousseau’s syndrome – thrombophlebitis; acanthosis nigricans – hyperpigmentation of axilla and groin; peripheral neuropathy) Signs of distant metastasis: Hepatomegally / ascites Krukenbergs tumor Blummers shelf (drop metastasis) Virchow’s node Sister Joseph node (pathognomonic of advances dse)

EVALUATION OF GASTRIC CANCER: History Clinical Examination Investigations The clinical features of gastric cancer may arise from local disease, its complications or its metastases.

Investigations for patients with gastric cancer Endoscopy & biopsy Performance status Physiological assessment Cardio-pulmonary function CT chest & abdomen EUS (endoscopic ultrasound) Laparoscopy

Laparoscopy Inspect peritoneal surfaces, liver surface. Identification of advanced disease avoids non-therapeutic laparotomy in 25%. Patients with small volume metastases in peritoneum or liver have a life expectancy of 3-9 months, thus rarely benefit from palliative resection.

Screening of Gastric Cancer Patients at risk for gastric CA should undergo yearly endoscopy and biopsy: Familial adenomatous polyposis Hereditary nonpolyposis colorectal cancer Gastric adenomas Menetrier’s disease Intestinal metaplasia or dysplasia Remote gastrectomy or gastrojejunostomy

Surgical Treatment

TREATMENT: SURGERY: Radical subtotal gastrectomy Standard operation for gastric cancer Organs resected: Distal 75% of stomach 2 cm of duodenum Greater & lesser omentum Ligation of R & L gastric artery and gastroepiploic vesels Billroth II gastojejunostomy

TREATMENT: SURGERY: Radical subtotal gastrectomy Standard operation for gastric cancer If gastric remnant left is small (<20%) do Roux-en-Y reconstruction

Surgical Treatment

References http://www.plaintest.com/general Пропедевтика внутренних болезней - Гребенев А.Л. – Учебник Пропедевтика внутренних болезней - Лис М.А. – Учебник www.google.com
39754-dars_gasteric_cancer.ppt
- Количество слайдов: 34