

35bcd7f064d3216738ce7d024f0191af.ppt
- Количество слайдов: 37
 From Casualty to Emergency medicine: The history of Training in Emergency Medicine UK “You have to understand the past to know the present” Carl Sagan 50 th Anniversary RCEM Chris Maimaris MB Ch. B, FRCS, FFAEM, FRCEM
From Casualty to Emergency medicine: The history of Training in Emergency Medicine UK “You have to understand the past to know the present” Carl Sagan 50 th Anniversary RCEM Chris Maimaris MB Ch. B, FRCS, FFAEM, FRCEM
 1950 s: 800 casualty areas -OPD • • • General practice infancy College GP 1952 RCS, RCP, RCO&G Faculty Anaesthetists RCSEng Hospitals dominate Medicine and Surgery Inpatients and OPDs Surgery: GS, trauma+Ortho Medicine : Ditto
1950 s: 800 casualty areas -OPD • • • General practice infancy College GP 1952 RCS, RCP, RCO&G Faculty Anaesthetists RCSEng Hospitals dominate Medicine and Surgery Inpatients and OPDs Surgery: GS, trauma+Ortho Medicine : Ditto
 Platt Report 1962
Platt Report 1962
 Platt Report 1962 • • 800 hospitals with “casualty” departments Difficult provide adequate experienced staff Large number pts who should be Rx by GPs Need a service for seriously injured +RTAs New name: “Accident Emergency” Reduce number departments Consultant surgeons to supervise
Platt Report 1962 • • 800 hospitals with “casualty” departments Difficult provide adequate experienced staff Large number pts who should be Rx by GPs Need a service for seriously injured +RTAs New name: “Accident Emergency” Reduce number departments Consultant surgeons to supervise
 1970 s • 1967: CSA- Casualty Surgeons association • 1970 -75 pilot 30+ A&E Consultants • Specialist Advisory Cmt in A&E at RCP: 1 st SR 1978 • 1977: 109 consultants – 60% higher qual. - FRCS • BMA concerns: moratorium new appointment • BMA Lewin Report 1979
1970 s • 1967: CSA- Casualty Surgeons association • 1970 -75 pilot 30+ A&E Consultants • Specialist Advisory Cmt in A&E at RCP: 1 st SR 1978 • 1977: 109 consultants – 60% higher qual. - FRCS • BMA concerns: moratorium new appointment • BMA Lewin Report 1979
 BMA Lewin Report 1979 • Pilot is successful • Well organised A&E care where consultants present • A&E cons work better if surgeon and physician • Establish and expand SR training
BMA Lewin Report 1979 • Pilot is successful • Well organised A&E care where consultants present • A&E cons work better if surgeon and physician • Establish and expand SR training
 Birmingham Accident Hospital 1970’s New Addenbrookes 1972
Birmingham Accident Hospital 1970’s New Addenbrookes 1972
 PG Training Structure 1980 -1995 HO, SHO, Registrar, Senior Registrar grades Parent college issues certificate 1+5+5= 10+ years SAC A&E advice re: Senior Reg posts postgraduate diploma Colleges: FRCS, MRCP, Higher Specialist training Approved A&E SR post 3 yr (+A&E Registrar =2 yr) General Professional Training: Med, Surg, other SHO/Reg - 5 years Pre-registration year
PG Training Structure 1980 -1995 HO, SHO, Registrar, Senior Registrar grades Parent college issues certificate 1+5+5= 10+ years SAC A&E advice re: Senior Reg posts postgraduate diploma Colleges: FRCS, MRCP, Higher Specialist training Approved A&E SR post 3 yr (+A&E Registrar =2 yr) General Professional Training: Med, Surg, other SHO/Reg - 5 years Pre-registration year
 My Training 1980 -91 • • • 5 yrs HO+SHO 2. 5 yrs Registrar 3. 5 yrs SR 12 hospitals FRCS Ed
My Training 1980 -91 • • • 5 yrs HO+SHO 2. 5 yrs Registrar 3. 5 yrs SR 12 hospitals FRCS Ed
 - became MRCSEd") 1980 s: • 1983 First diet of FRCSEd (A & E) - became MRCSEd (A&E) subsequently. Final diet in 2009. • 1984 Australasian College of Emergency Medicine established • 1986 1 st International Conference Emergency Medicine London • 1988 BAEM British Association A&E Medicine: Journal A&E M PLUS Archives of Emergency Medicine journals. • ATLS at RCS and ACLS
1980 s: • 1983 First diet of FRCSEd (A & E) - became MRCSEd (A&E) subsequently. Final diet in 2009. • 1984 Australasian College of Emergency Medicine established • 1986 1 st International Conference Emergency Medicine London • 1988 BAEM British Association A&E Medicine: Journal A&E M PLUS Archives of Emergency Medicine journals. • ATLS at RCS and ACLS
 Archives of Emergency Medicine, 1988 Adequacy of senior registrar training in accident and emergency medicine over the last 5 years P. DRISCOLL, A. COPE & S. A. D. MILES SUMMARY This study investigated the limitations of the present Senior Registrar training programmes in A&E Medicine. A completed questionnaire was returned from 46 of the 48 Consultants who had taken up post in the last 5 years and had themselves studied on one of the established training programmes. The positive views of the clinical training contrast sharply with the administrative and managerial components. Around 80% of the new Consultants had no training in clinical budgeting or ordering equipment and only half had experience of appointing staff and organizing locums. This is worrying as over 63% had or are currently facing staffing problems and 69% have financial or equipment difficulties. A more active training programme in A&E administration and management is recommended.
Archives of Emergency Medicine, 1988 Adequacy of senior registrar training in accident and emergency medicine over the last 5 years P. DRISCOLL, A. COPE & S. A. D. MILES SUMMARY This study investigated the limitations of the present Senior Registrar training programmes in A&E Medicine. A completed questionnaire was returned from 46 of the 48 Consultants who had taken up post in the last 5 years and had themselves studied on one of the established training programmes. The positive views of the clinical training contrast sharply with the administrative and managerial components. Around 80% of the new Consultants had no training in clinical budgeting or ordering equipment and only half had experience of appointing staff and organizing locums. This is worrying as over 63% had or are currently facing staffing problems and 69% have financial or equipment difficulties. A more active training programme in A&E administration and management is recommended.
 1990 s • • Consultants make a difference Limited training capacity, budgets, output 250 A&E Depts to have at least 1 cons, Big EDs 2+ Old Buildings, crowded A&Es, long waits
1990 s • • Consultants make a difference Limited training capacity, budgets, output 250 A&E Depts to have at least 1 cons, Big EDs 2+ Old Buildings, crowded A&Es, long waits
 1995 European Council Directive 93/16/EEC of 5 April 1993 to facilitate the free movement of doctors and the mutual recognition of their diplomas, certificates and other evidence of formal qualifications: 4 Freedoms: capital, people, goods, services. 2 nd August 1993: UK ratifies EU Treaty Re-organisation of Specialist Training The roles of the Specialist Training Authority, the CCST and the GMC's Specialist Register ORANGE GUIDE - RITAs
1995 European Council Directive 93/16/EEC of 5 April 1993 to facilitate the free movement of doctors and the mutual recognition of their diplomas, certificates and other evidence of formal qualifications: 4 Freedoms: capital, people, goods, services. 2 nd August 1993: UK ratifies EU Treaty Re-organisation of Specialist Training The roles of the Specialist Training Authority, the CCST and the GMC's Specialist Register ORANGE GUIDE - RITAs
 PG A&E Training Structure 1996 -2007 ‘Calman’ system: 1995 -2007 1+5+5 = 10+ years RITA: Orange guide to training Local Recruitment CCT Higher Specialist (Sp. R) Training 5 years General Professional (SHO) Training 3 -5 years Pre-registration year FFAEM Regional Recruitment MRCP, MRCS and MCEM
PG A&E Training Structure 1996 -2007 ‘Calman’ system: 1995 -2007 1+5+5 = 10+ years RITA: Orange guide to training Local Recruitment CCT Higher Specialist (Sp. R) Training 5 years General Professional (SHO) Training 3 -5 years Pre-registration year FFAEM Regional Recruitment MRCP, MRCS and MCEM
") Eo. E 1995 -97 • • Curriculums and PGMDT Deans (Eo. E J Biggs) Regional Committees for HST A&E Medicine Chair Howard Sherriff, F/B S Shankar PD- Program Director -CM
Eo. E 1995 -97 • • Curriculums and PGMDT Deans (Eo. E J Biggs) Regional Committees for HST A&E Medicine Chair Howard Sherriff, F/B S Shankar PD- Program Director -CM
 1990 s: • • 1993 Inauguration Faculty A&E Medicine 6 “parent” colleges 1996 First specialty exam Faculty A&E Medicine (FFAEM) Faculty is granted coat of arms by the College of Arms 1998 SAC A&E Medicine under auspices of FAEM. – Chairman Jonathan Marrow
1990 s: • • 1993 Inauguration Faculty A&E Medicine 6 “parent” colleges 1996 First specialty exam Faculty A&E Medicine (FFAEM) Faculty is granted coat of arms by the College of Arms 1998 SAC A&E Medicine under auspices of FAEM. – Chairman Jonathan Marrow
 Audit Commission 1995: “By Accident or Design” • A&E care delivered mainly by SHOs • More Cons/Middle Grades • Better organisation • ENPs • Better SHO training
Audit Commission 1995: “By Accident or Design” • A&E care delivered mainly by SHOs • More Cons/Middle Grades • Better organisation • ENPs • Better SHO training
 Better care for severely injured - RCSEng 2000 Retrospective study of 1000 deaths from injury in England Wales BMJ 1988: I D Anderson, M Woodford, F T de Dombal, and Miles Irving • 24 hr CT/Image transfer • All ventilated pts transferred NCCU • Evacuation Heamatomas <4 hrs
Better care for severely injured - RCSEng 2000 Retrospective study of 1000 deaths from injury in England Wales BMJ 1988: I D Anderson, M Woodford, F T de Dombal, and Miles Irving • 24 hr CT/Image transfer • All ventilated pts transferred NCCU • Evacuation Heamatomas <4 hrs
 BAEM: ‘Way Ahead’ Reports Medical staffing Workloads Interfaces : GP, specialties Recommended minimum staffing levels • Consultant JP • Training • CDU/Observation wards • •
BAEM: ‘Way Ahead’ Reports Medical staffing Workloads Interfaces : GP, specialties Recommended minimum staffing levels • Consultant JP • Training • CDU/Observation wards • •
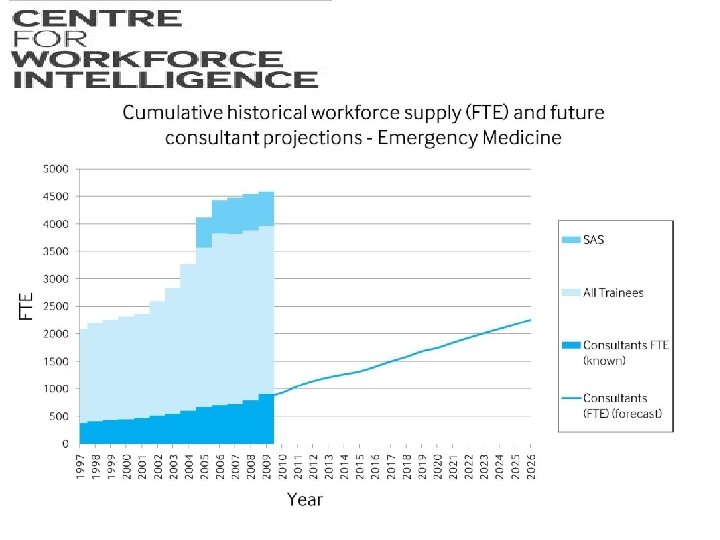
 Modernisation of A&E Depts 2000 • • • New Government 1997: Same spending plans Winters 1998 +1999 critical: Long A&E waits Modernisation Public Services: NHS Plan: 2000 Increase NHS Budget GDP 6% to 8% Modernisation Agency: NSFs, NICE, Networks MMC-Modernisation of Medical Careers 2007
Modernisation of A&E Depts 2000 • • • New Government 1997: Same spending plans Winters 1998 +1999 critical: Long A&E waits Modernisation Public Services: NHS Plan: 2000 Increase NHS Budget GDP 6% to 8% Modernisation Agency: NSFs, NICE, Networks MMC-Modernisation of Medical Careers 2007
 UK medical graduates 50 years
UK medical graduates 50 years
 New Consultant and GP contracts 2003
New Consultant and GP contracts 2003
 2005 -07 MMC • • • Abolition of SHO grade Foundation year FY 1+2 Run-Through training 7 Core Stems + ACCS Regional recruitment Implementation 2007
2005 -07 MMC • • • Abolition of SHO grade Foundation year FY 1+2 Run-Through training 7 Core Stems + ACCS Regional recruitment Implementation 2007
 MMC 2005 -07 School of Emergency Medicine
MMC 2005 -07 School of Emergency Medicine
 Run-through training in Emergency Medicine 2007 CCT in Emergency Medicine +/- sub-specialty/certification FCEM ST 4, ST 5, ST 6 Emergency Medicine MCEM ST 3 EM trauma & musculoskeletal or T&O EM Paediatrics + Paediatric EM ST 6 ST 5 ST 4 ST 3 ST 2 ST 1 ACCS ST 2 1 year Anaesthetic + ICU ST 1 1 year EM + AM Competitive Entry by Interview FY 2 FY 1 2+6 = 8
Run-through training in Emergency Medicine 2007 CCT in Emergency Medicine +/- sub-specialty/certification FCEM ST 4, ST 5, ST 6 Emergency Medicine MCEM ST 3 EM trauma & musculoskeletal or T&O EM Paediatrics + Paediatric EM ST 6 ST 5 ST 4 ST 3 ST 2 ST 1 ACCS ST 2 1 year Anaesthetic + ICU ST 1 1 year EM + AM Competitive Entry by Interview FY 2 FY 1 2+6 = 8
 Un-coupled EM CCT training 2008 CCT EM +/- Sub-specialist – Independent specialist practitioner CCT route FCEM Post-CCT Article 14 -CESR route ST 4, ST 5, ST 6 30/12 in EM up-to 6/12 relevant other Sub-specialisation: dual accreditation PEM, ICM; Acute Med; Pre-hospital EM HST 3 -yrs Competitive Entry ST 4: Some/All CT competences 2+3+3=8 CT 3 EM Musculoskeletal or T&O MCEM EM Paediatrics ACCS CT 2 1 year Anaesthetics + ICU 6/12 each or 9/3 CT 1 1 year EM + AM 6/12 each Core Training 3 yrs Competitive Entry: CT 1 ACCS (EM) +CT 3 FY 2 FY 1 School of Emergency Medicine Foundation Training
Un-coupled EM CCT training 2008 CCT EM +/- Sub-specialist – Independent specialist practitioner CCT route FCEM Post-CCT Article 14 -CESR route ST 4, ST 5, ST 6 30/12 in EM up-to 6/12 relevant other Sub-specialisation: dual accreditation PEM, ICM; Acute Med; Pre-hospital EM HST 3 -yrs Competitive Entry ST 4: Some/All CT competences 2+3+3=8 CT 3 EM Musculoskeletal or T&O MCEM EM Paediatrics ACCS CT 2 1 year Anaesthetics + ICU 6/12 each or 9/3 CT 1 1 year EM + AM 6/12 each Core Training 3 yrs Competitive Entry: CT 1 ACCS (EM) +CT 3 FY 2 FY 1 School of Emergency Medicine Foundation Training
 ACCS Eo. E without Essex/Beds/Herts 80 Anaesthetics/ICM Emergency Med 48 48 56 62 POSTS Acute Med 70 Other 60 Percentage 50 40 30 20 10 0 2007 2008 2009 2010
ACCS Eo. E without Essex/Beds/Herts 80 Anaesthetics/ICM Emergency Med 48 48 56 62 POSTS Acute Med 70 Other 60 Percentage 50 40 30 20 10 0 2007 2008 2009 2010
 Eo. E: ST 4 Recruitment 2010 School of Emergency Medicine
Eo. E: ST 4 Recruitment 2010 School of Emergency Medicine
 National initiative
National initiative
 Recruitment Initiatives 2012 -17 Regional • • • Expand ACCS from 14 to 43 posts Aim full recruited+ reduce attrition Re-introduce RT option 85+% of STs DRE-EM: 30+ posts Regional activities – – – monthly teaching programs SAS TPD+ Night Safe training program Exam preparation MCEM and FCEM, MCEM A ARCPs, Workshops and Faculty Days School manager, website, promotional material
Recruitment Initiatives 2012 -17 Regional • • • Expand ACCS from 14 to 43 posts Aim full recruited+ reduce attrition Re-introduce RT option 85+% of STs DRE-EM: 30+ posts Regional activities – – – monthly teaching programs SAS TPD+ Night Safe training program Exam preparation MCEM and FCEM, MCEM A ARCPs, Workshops and Faculty Days School manager, website, promotional material
 Good training practice-Local level? • • Well staffed EDs in all grades Balanced Rotas, Training environment, Wp. BAs Consultant 08 -24, MGs 24/7, clinical supervision Good weekly teaching programs Attendance at regional days and SL Regular feedback and support for progression Faculty STRs: timely, fair, reflecting ST abilities Support for slow learners
Good training practice-Local level? • • Well staffed EDs in all grades Balanced Rotas, Training environment, Wp. BAs Consultant 08 -24, MGs 24/7, clinical supervision Good weekly teaching programs Attendance at regional days and SL Regular feedback and support for progression Faculty STRs: timely, fair, reflecting ST abilities Support for slow learners
 Australian EM training
Australian EM training
 What Next? • ‘Addenbrookes’ model: Common frontdoor with Acute medicine 2006 • Multi-professional workforce – ENPs, ACPs, PAs, Physios, SW, MH, Pharmacists, Discharge planners • Expansion of EM and AM- ACCS • Co-location OOH Primary care • Work-Life balance: EM/AM attractive
What Next? • ‘Addenbrookes’ model: Common frontdoor with Acute medicine 2006 • Multi-professional workforce – ENPs, ACPs, PAs, Physios, SW, MH, Pharmacists, Discharge planners • Expansion of EM and AM- ACCS • Co-location OOH Primary care • Work-Life balance: EM/AM attractive
 EM Training 50 yrs Perspective • • EM development driven by its patients All times Casualty ---A&E 1960 s CSA at BMA: new specialty 100 Consultant 1970 s Lewin Report –SR training programmes 1980 s ‘Calman’ Reforms and MMC changes 1990 s-00 s NHS modernisation and re-organisation 2000 The future in your hands
EM Training 50 yrs Perspective • • EM development driven by its patients All times Casualty ---A&E 1960 s CSA at BMA: new specialty 100 Consultant 1970 s Lewin Report –SR training programmes 1980 s ‘Calman’ Reforms and MMC changes 1990 s-00 s NHS modernisation and re-organisation 2000 The future in your hands
 My advice to a young FY 2 doctor asking about a career in Emergency Medicine… • “Ithaka” by CP Cavafy • As you set out for Ithaka hope the voyage is a long one, full of adventure, full of discovery. Laistrygonians and Cyclops, angry Poseidon—don’t be afraid of them: you’ll never find things like that on your way….
My advice to a young FY 2 doctor asking about a career in Emergency Medicine… • “Ithaka” by CP Cavafy • As you set out for Ithaka hope the voyage is a long one, full of adventure, full of discovery. Laistrygonians and Cyclops, angry Poseidon—don’t be afraid of them: you’ll never find things like that on your way….