

169f41444183b862fcc553229aa17ea2.ppt
- Количество слайдов: 63
 Fractures of the Femoral Neck and Intertrochanteric Fractures Knut Strömsöe, MD Ph. D, Orthopaedic Department, Aker University Hospital, Oslo, Norway
Fractures of the Femoral Neck and Intertrochanteric Fractures Knut Strömsöe, MD Ph. D, Orthopaedic Department, Aker University Hospital, Oslo, Norway
 Classification of fractures in the proximal femur
Classification of fractures in the proximal femur
 of fractures in the proximal femur") The Comprehensive AO/ASIF Classification (Müller et al. 1990) of fractures in the proximal femur
The Comprehensive AO/ASIF Classification (Müller et al. 1990) of fractures in the proximal femur
 The comprehensive classification of neck fractures of the proximal femur
The comprehensive classification of neck fractures of the proximal femur
 (based on the angle the fracture line with") Pauwel’s classification of neck fractures (1965) (based on the angle the fracture line with the resultant of forces (R))
Pauwel’s classification of neck fractures (1965) (based on the angle the fracture line with the resultant of forces (R))
 Garden’s classification (based on the relationship of the medial trabeculae in the head and pelvis)
Garden’s classification (based on the relationship of the medial trabeculae in the head and pelvis)
 Reported annual incidence of hip fractures per 100 000 of population (Parker and Pryor 1993) • • Sweden Canada Finland UK USA Malayasia Israel Korea 165 103 91 86 80 70 59 34
Reported annual incidence of hip fractures per 100 000 of population (Parker and Pryor 1993) • • Sweden Canada Finland UK USA Malayasia Israel Korea 165 103 91 86 80 70 59 34
 Number of hip fractures in Norway 1979 -1999: population 4 000 • 1979: 6 800 • 1989: 9 900 • 1999: 11800 (290 per 100 000)
Number of hip fractures in Norway 1979 -1999: population 4 000 • 1979: 6 800 • 1989: 9 900 • 1999: 11800 (290 per 100 000)
 We have to define our problem A g i n g 1900 1930 1960 1997 2 2000 2020
We have to define our problem A g i n g 1900 1930 1960 1997 2 2000 2020
 Osteoporosis Int; 2: 285 -289 • 6.") Cooper C, Campion G, Melton LJ (1992) Osteoporosis Int; 2: 285 -289 • 6. 25 million is an estimated number of hip fractures world wide by 2050 • Increasing world population and increasing life expectancy seems to be the most important reason for this increase
Cooper C, Campion G, Melton LJ (1992) Osteoporosis Int; 2: 285 -289 • 6. 25 million is an estimated number of hip fractures world wide by 2050 • Increasing world population and increasing life expectancy seems to be the most important reason for this increase
 Why do we experience an increase the number of fractures? • Falling frequency increases with age • Porosity of bone increases with age Cooper C, Campion G, Melton LJ (1992) Osteoporosis Int; 2: 285 -289
Why do we experience an increase the number of fractures? • Falling frequency increases with age • Porosity of bone increases with age Cooper C, Campion G, Melton LJ (1992) Osteoporosis Int; 2: 285 -289
 Determinants of fracture risk -Neuromuscular function -Environmental hazards -Time spent at risk Type of fall Protective responses Energy absorption Risk of fall Force of impact Risk of fracture Geometry of bone Bone mineral mass Quality of bone Strength of bone
Determinants of fracture risk -Neuromuscular function -Environmental hazards -Time spent at risk Type of fall Protective responses Energy absorption Risk of fall Force of impact Risk of fracture Geometry of bone Bone mineral mass Quality of bone Strength of bone
 Choice of Treatment policy
Choice of Treatment policy
 Fracture related pattern of femoral neck fractures representing risk for osteofixation failure, non-union and avascular necrosis • Grade of dislocation (Garden 1972, Thorngren 1991) • Size of head fragment (Benterud et al. Acta Orth Scand 1994) • Posterior comminution (Benterud et al. 1997) • Osteoporosis (Bentley 1972, Riska 1969, Anderson 1969, Thorngren 1995)
Fracture related pattern of femoral neck fractures representing risk for osteofixation failure, non-union and avascular necrosis • Grade of dislocation (Garden 1972, Thorngren 1991) • Size of head fragment (Benterud et al. Acta Orth Scand 1994) • Posterior comminution (Benterud et al. 1997) • Osteoporosis (Bentley 1972, Riska 1969, Anderson 1969, Thorngren 1995)
 Fracture related pattern of femoral neck fractures leading to a “treatment policy”. . • Impacted fractures are reported to have less incidence of non-unions (Bentley G, JBJS; 50 B: 551, 1968, Raymakers, 1993) • Impacted fractures develop less segmental collapse in avascular necrosis of the head ? Crawford reported 12 % of avascular necrosis in 50 impacted fractures out of 339 femoral neck fractures with an overall incidence of avascular necrosis in 37% (Crawford H, JBJS; 47 A: 830, 1965)
Fracture related pattern of femoral neck fractures leading to a “treatment policy”. . • Impacted fractures are reported to have less incidence of non-unions (Bentley G, JBJS; 50 B: 551, 1968, Raymakers, 1993) • Impacted fractures develop less segmental collapse in avascular necrosis of the head ? Crawford reported 12 % of avascular necrosis in 50 impacted fractures out of 339 femoral neck fractures with an overall incidence of avascular necrosis in 37% (Crawford H, JBJS; 47 A: 830, 1965)
 arthroplasty?") Preservation of the femoral head or hemi (total) arthroplasty?
Preservation of the femoral head or hemi (total) arthroplasty?
, from Bergen, worked as a Professor in Oslo. He nailed a") Julius Nicolaysen (18311909), from Bergen, worked as a Professor in Oslo. He nailed a medial femoral neck fracture in 1893, 2 years before Wilhelm Konrad Røntgen discovered the Xray
Julius Nicolaysen (18311909), from Bergen, worked as a Professor in Oslo. He nailed a medial femoral neck fracture in 1893, 2 years before Wilhelm Konrad Røntgen discovered the Xray
 Femoral neck fractures in the young or “young geriatric” patient have different aspects as to the older patient. . • Osteoporosis is frequent not the main problem • Fracture pattern is often different as to the older patient • Prosthetic replacement as a primary treatment alternative has to be chosen with greater care than in the older patient
Femoral neck fractures in the young or “young geriatric” patient have different aspects as to the older patient. . • Osteoporosis is frequent not the main problem • Fracture pattern is often different as to the older patient • Prosthetic replacement as a primary treatment alternative has to be chosen with greater care than in the older patient
 in the") Transcervical and subcapital femoral neck fracture (31 B and 31 -C 3) in the “young geriatric” patient • Hip replacement (hemi or total arthroplasty) represents an internal amputation with all its implications • Preservation of the joint (as in all joint fractures) should be what we aim at in the treatment
Transcervical and subcapital femoral neck fracture (31 B and 31 -C 3) in the “young geriatric” patient • Hip replacement (hemi or total arthroplasty) represents an internal amputation with all its implications • Preservation of the joint (as in all joint fractures) should be what we aim at in the treatment
 Secondary failures like secondary osteofixation failure as well as segmental collapse may be handled by secondary arthroplasty • “Primary and secondary Charmley-Hastings hemiarthroplasty in displaced femoral neck fractures and their sequelae” Benterud JG, Kok WL, Alho A. In: Ann Chir Gynaecol 1996; 85(1): 72 -6
Secondary failures like secondary osteofixation failure as well as segmental collapse may be handled by secondary arthroplasty • “Primary and secondary Charmley-Hastings hemiarthroplasty in displaced femoral neck fractures and their sequelae” Benterud JG, Kok WL, Alho A. In: Ann Chir Gynaecol 1996; 85(1): 72 -6
 ?") What do we do with the impacted femoral neck fracture (31 -B 2) ? Functionally treated: No. of Patients 59 73 Raaymakers 1993 Age 15 -69 Instable 2 = 3% 70 -94 16 = 22 %
What do we do with the impacted femoral neck fracture (31 -B 2) ? Functionally treated: No. of Patients 59 73 Raaymakers 1993 Age 15 -69 Instable 2 = 3% 70 -94 16 = 22 %
 ?") What do we do with the impacted femoral neck fracture (31 -B 2) ? In the literature we find: Instability: After early mobilisation without weightbearing: 8 -19% After immediate full weight bearing: 32 -65 %
What do we do with the impacted femoral neck fracture (31 -B 2) ? In the literature we find: Instability: After early mobilisation without weightbearing: 8 -19% After immediate full weight bearing: 32 -65 %
 ?") What do we do with the impacted femoral neck fracture (31 -B 2) ? Mortality in impacted femoral neck fractures: Operative treatment Conservative treatment (Raaymakers 1993) > 10 % 1. 8 - 3. 3. %
What do we do with the impacted femoral neck fracture (31 -B 2) ? Mortality in impacted femoral neck fractures: Operative treatment Conservative treatment (Raaymakers 1993) > 10 % 1. 8 - 3. 3. %
 ?") What do we do with the impacted femoral neck fracture (31 -B 2) ? “It is impossible at the time the patient presents himself to predict which fractures will undergo desimpaction” (Bentley, Crawford, Judet, Asser, Hansen, Famos, Jeannaret) Retroversion is not an important reason for higher instability (Raaymakers 1993)
What do we do with the impacted femoral neck fracture (31 -B 2) ? “It is impossible at the time the patient presents himself to predict which fractures will undergo desimpaction” (Bentley, Crawford, Judet, Asser, Hansen, Famos, Jeannaret) Retroversion is not an important reason for higher instability (Raaymakers 1993)
 ?") What do we do with the impacted femoral neck fracture (31 -B 2) ? Conclusion may be as follows: Age less than 70: Internal fixation in situ Age more than 70: Conservative treatment. If secondary dislocation or AVN: Arhroplasty
What do we do with the impacted femoral neck fracture (31 -B 2) ? Conclusion may be as follows: Age less than 70: Internal fixation in situ Age more than 70: Conservative treatment. If secondary dislocation or AVN: Arhroplasty
 In dislocated femoral neck fractures. . Timing of Surgery • As preservation of the femoral head is the main goal of our treatment surgery should be performed as soon as possible and latest within 6 hours • The value of decompression of the intracapsular haematoma still is unknown
In dislocated femoral neck fractures. . Timing of Surgery • As preservation of the femoral head is the main goal of our treatment surgery should be performed as soon as possible and latest within 6 hours • The value of decompression of the intracapsular haematoma still is unknown
 In dislocated femoral neck fractures. . Timing of Surgery. If not immediate ? • The value of immobilisation in traction is questionable in concern of development of avascular head necrosis • Positioning of the hip in the most comfortable position to the patient probably also is the position where the intracapsular pressure is at lowest
In dislocated femoral neck fractures. . Timing of Surgery. If not immediate ? • The value of immobilisation in traction is questionable in concern of development of avascular head necrosis • Positioning of the hip in the most comfortable position to the patient probably also is the position where the intracapsular pressure is at lowest
 Is the viability of the femoral head predictable? Preoperative • By fracture classification? • By scintigraphy? • MRI Intraoperative • Intraoperative by bleeding? • Intraoperative by measuring of electric potential with temporary implanted platine electrodes and gas insuflation (H 2 O 2)?
Is the viability of the femoral head predictable? Preoperative • By fracture classification? • By scintigraphy? • MRI Intraoperative • Intraoperative by bleeding? • Intraoperative by measuring of electric potential with temporary implanted platine electrodes and gas insuflation (H 2 O 2)?
 In femoral neck fractures. . Is the viability of the femoral head predictable? MRI
In femoral neck fractures. . Is the viability of the femoral head predictable? MRI
 Reduction technique in intracapsular fractures of the femoral neck • Loosen the fracture by “unpack” it • After having obtained the reduction “pack the fracture” and then fix it Mark Flynn injury 1973
Reduction technique in intracapsular fractures of the femoral neck • Loosen the fracture by “unpack” it • After having obtained the reduction “pack the fracture” and then fix it Mark Flynn injury 1973
") Impacted fracture Non displaced fracture Impacted fracture Displaced fracture Reduction manoeuvre (Leadbetter)
Impacted fracture Non displaced fracture Impacted fracture Displaced fracture Reduction manoeuvre (Leadbetter)
 Intracapsular fractures of the femoral neck • Internal rotation of the foot should result in the femoral head, neck and shaft all appearing in a straight line with no residual anglulation at the fracture site ventral dorsal
Intracapsular fractures of the femoral neck • Internal rotation of the foot should result in the femoral head, neck and shaft all appearing in a straight line with no residual anglulation at the fracture site ventral dorsal
 Choice of Implant
Choice of Implant
 Choice of Implant • Cannulated bone screws • Non cannulated bone screws • Nails with hooks (Hansen nails) 0 Angle blade plate • 130 • Sliding Screw Plate Systems (DHS, HCS)
Choice of Implant • Cannulated bone screws • Non cannulated bone screws • Nails with hooks (Hansen nails) 0 Angle blade plate • 130 • Sliding Screw Plate Systems (DHS, HCS)
 Implant demands. . • The implant shall provide stability - prevent dislocation in varus - prevent dislocation in retroversion - prevent rotational micromovements • Allow axial sintering along the implant without penetrating into the joint • In case of delayed union and non union migration into the joint/pelvis should not be possible
Implant demands. . • The implant shall provide stability - prevent dislocation in varus - prevent dislocation in retroversion - prevent rotational micromovements • Allow axial sintering along the implant without penetrating into the joint • In case of delayed union and non union migration into the joint/pelvis should not be possible
 Choice of Implant: Sliding Screw Plate System
Choice of Implant: Sliding Screw Plate System
 Choice of Implant Benterud JG, Husby T, Nordsletten L, Alho A: “Fixation of displaced femoral neck fractures with a sliding screw plate and a cancellous screw or two Olmed screws. A prospective study of 225 elderly patients with a 3 -year follow up”. Ann Chir Gynaecol 1997; 86 (4) 338 -42
Choice of Implant Benterud JG, Husby T, Nordsletten L, Alho A: “Fixation of displaced femoral neck fractures with a sliding screw plate and a cancellous screw or two Olmed screws. A prospective study of 225 elderly patients with a 3 -year follow up”. Ann Chir Gynaecol 1997; 86 (4) 338 -42
 338 -42 Conclusions. Both treatment") Choice of Implant Ann Chir Gynaecol 1997; 86 (4) 338 -42 Conclusions. Both treatment methods resulted in high rate of osteofixation failures (18. 5 % in the SSP group and 19. 5 % in the Olmed group) and non-unions (6. 2 % and 8. 5% respectively)
Choice of Implant Ann Chir Gynaecol 1997; 86 (4) 338 -42 Conclusions. Both treatment methods resulted in high rate of osteofixation failures (18. 5 % in the SSP group and 19. 5 % in the Olmed group) and non-unions (6. 2 % and 8. 5% respectively)
 Choice of Implant • In 31 - B 2 fractures of the “young geriatric” patient a 4 hole DHS with an antirotational screw, however, is the implant of choice. The fixation on the tensile side of the femur and gliding cylinder for the screw provides stability over time
Choice of Implant • In 31 - B 2 fractures of the “young geriatric” patient a 4 hole DHS with an antirotational screw, however, is the implant of choice. The fixation on the tensile side of the femur and gliding cylinder for the screw provides stability over time
 Choice of Implant Angle blade plate and cancellous screw
Choice of Implant Angle blade plate and cancellous screw
 Femoral neck fractures: If screws: Two or three screws? Position of the screws? Dimensions of the screws? Three screw fixation technique in fixation of cervical fractures of the proximal femur
Femoral neck fractures: If screws: Two or three screws? Position of the screws? Dimensions of the screws? Three screw fixation technique in fixation of cervical fractures of the proximal femur
 Choice of Implant Screws with head and washer preventing axial migration in instability Screws without head and equal diameter of thread and shank
Choice of Implant Screws with head and washer preventing axial migration in instability Screws without head and equal diameter of thread and shank
 Fate of the medial neck fracture after ORIF • Early osteofixation failure in 8 -16 % • Non-union in 8 -10% • AVN in 6 -10 % • This makes an overall failure rate of 20 -30% • but- in the first year after a medial neck fracture 25 % of the patient are dead to unrelated fracture desease
Fate of the medial neck fracture after ORIF • Early osteofixation failure in 8 -16 % • Non-union in 8 -10% • AVN in 6 -10 % • This makes an overall failure rate of 20 -30% • but- in the first year after a medial neck fracture 25 % of the patient are dead to unrelated fracture desease
") Classification of trochanteric fractures (31 -A 1 -3)
Classification of trochanteric fractures (31 -A 1 -3)
 Bone mass related to age in cancellous bone and cortical bone Bone mass Trochcanteric area Neck of the femur 50 years 100 years Age
Bone mass related to age in cancellous bone and cortical bone Bone mass Trochcanteric area Neck of the femur 50 years 100 years Age
 Fractures in the proximal Femur at Aker Hospital, Oslo, Norway 1999 Diagnose Cervical Frx No Median age male female 282 84 (29 -104) 53 229 Pertrochanteric Frx 186 88 (54 -102) 75 111 Subtrochanteric Frx 86 ( 39 -95) 20 17 148 357 37 505
Fractures in the proximal Femur at Aker Hospital, Oslo, Norway 1999 Diagnose Cervical Frx No Median age male female 282 84 (29 -104) 53 229 Pertrochanteric Frx 186 88 (54 -102) 75 111 Subtrochanteric Frx 86 ( 39 -95) 20 17 148 357 37 505
 Biomechanichs of the proximal femur
Biomechanichs of the proximal femur
 Biomechanichs of the proximal femur
Biomechanichs of the proximal femur
 Biomechanichs of the proximal femur
Biomechanichs of the proximal femur
 Fracture pattern reflects biomechanichs of the proximal femur in different stages by falling • Falling activates tensile forces of the muscles • Falling induces rotation of the femur on the fixed leg • Forces act on the trochanter by direct contact at the end of the fall
Fracture pattern reflects biomechanichs of the proximal femur in different stages by falling • Falling activates tensile forces of the muscles • Falling induces rotation of the femur on the fixed leg • Forces act on the trochanter by direct contact at the end of the fall
 In unstable trochanteric fractures in the elderly the implant chosen have to: • respect the instability of the fracture • allow fracture impaction during motion without fixation failure • secure retention of the fracture in acceptable position during healing • build a biomechanical construct with the bone allowing early weight bearing
In unstable trochanteric fractures in the elderly the implant chosen have to: • respect the instability of the fracture • allow fracture impaction during motion without fixation failure • secure retention of the fracture in acceptable position during healing • build a biomechanical construct with the bone allowing early weight bearing
 31 -A 3. 3 Fracture. DHS and TSP • sliding screw -plate system allowing the fracture sintering • plate on the tensile site neutralising tension forces • Trochanteric Supporting Plate preventing femoral shaft medialisation • Additional antirotational screw Week 0 Week 8
31 -A 3. 3 Fracture. DHS and TSP • sliding screw -plate system allowing the fracture sintering • plate on the tensile site neutralising tension forces • Trochanteric Supporting Plate preventing femoral shaft medialisation • Additional antirotational screw Week 0 Week 8
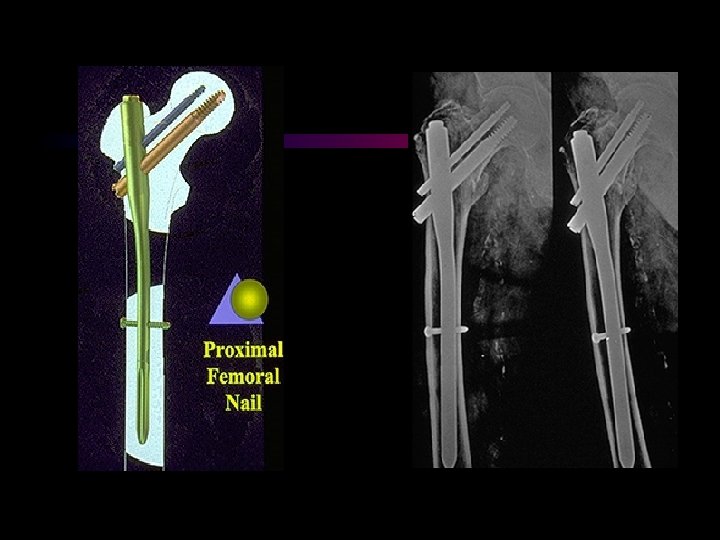
 31 -A 3. 3 Fracture. , The -nail • sliding screw-nail • nail in the centre of the femoral axis • reduction of the lever arm • no neutralisation on the tensile side • sintering in varus with “cutting through”
31 -A 3. 3 Fracture. , The -nail • sliding screw-nail • nail in the centre of the femoral axis • reduction of the lever arm • no neutralisation on the tensile side • sintering in varus with “cutting through”
 31 -A 3. 3 Fracture. The -nail Day 126 Day 160
31 -A 3. 3 Fracture. The -nail Day 126 Day 160
 In unstable trochanteric fractures in the elderly the implant chosen have to: • respect the instability of the fracture • allow fracture impaction during motion without fixation failure • secure retention of the fracture in acceptable position during healing • build a biomechanical construct with the bone allowing early weight bearing
In unstable trochanteric fractures in the elderly the implant chosen have to: • respect the instability of the fracture • allow fracture impaction during motion without fixation failure • secure retention of the fracture in acceptable position during healing • build a biomechanical construct with the bone allowing early weight bearing
 Fractures at the tip of the short - nail 51 days
Fractures at the tip of the short - nail 51 days
 Fractures at the tip of the nail • Aune et al. Acta Orthop Scand 1994; 65 (2): 127 -30: HCS vs. Gamma nail 378 patients: 5. 6 % • Madsen et al: J Orthop Trauma 1998 Vol. 12. No 4 50 patients 2. 9% • Osnes et al. Norw. proceedings 1998: 379 patients 5. 3%
Fractures at the tip of the nail • Aune et al. Acta Orthop Scand 1994; 65 (2): 127 -30: HCS vs. Gamma nail 378 patients: 5. 6 % • Madsen et al: J Orthop Trauma 1998 Vol. 12. No 4 50 patients 2. 9% • Osnes et al. Norw. proceedings 1998: 379 patients 5. 3%
 Stress measurements at the end of the nail. A comparative study between the -nail and the PFN. E. Euler. LMU München 1999 A photoelastic loading study Stress by cyclic loading with 700 N up to 7 times as high in the Gamma nail as in the PFN DHS + TSP
Stress measurements at the end of the nail. A comparative study between the -nail and the PFN. E. Euler. LMU München 1999 A photoelastic loading study Stress by cyclic loading with 700 N up to 7 times as high in the Gamma nail as in the PFN DHS + TSP
 The Medoff sliding plate • A sliding screw plate system allowing sintering along the neck axis as well as along the femoral axis
The Medoff sliding plate • A sliding screw plate system allowing sintering along the neck axis as well as along the femoral axis
 The Medoff sliding plate used in a 31 -A 3. 2 fracture with reversed fracture line
The Medoff sliding plate used in a 31 -A 3. 2 fracture with reversed fracture line
 "A great responsibility rests on the surgeon who introduces a new method of treatment. The desire to have a new idea published is so great the originator is often led astray, and the method is broadcast before it has been proved worthwhile and before the technique has been perfected. " Smith-Peterson, Cave & Vangorder Archives of Surgery 1931
"A great responsibility rests on the surgeon who introduces a new method of treatment. The desire to have a new idea published is so great the originator is often led astray, and the method is broadcast before it has been proved worthwhile and before the technique has been perfected. " Smith-Peterson, Cave & Vangorder Archives of Surgery 1931
 Thank you for your attention
Thank you for your attention