

1609242c0e56a414d0a241e23020bd0b.ppt
- Количество слайдов: 33
 Financial Implications of HIV/AIDS in South Africa – the role of the Business Sector Findings from aids 2031 costing & the efforts of the National AIDS Spending Assessment 7 Apr 2011 Teresa Guthrie, CEGAA Teresa Guthrie, Robert Hecht, Yogan Pillay , Mark Blecher, Kelsey Case
Financial Implications of HIV/AIDS in South Africa – the role of the Business Sector Findings from aids 2031 costing & the efforts of the National AIDS Spending Assessment 7 Apr 2011 Teresa Guthrie, CEGAA Teresa Guthrie, Robert Hecht, Yogan Pillay , Mark Blecher, Kelsey Case
 Overview of the Cost Estimates The aids 2031 South African costing project was carried out during 2009 -2010, sponsored and guided by a national Steering Committee composed of senior South Africa officials and other leading national figures. It was part of a larger international project led by R 4 D which included the estimation of global costs. It aimed to estimate the long-term costs of various response scenarios till 2031. 2
Overview of the Cost Estimates The aids 2031 South African costing project was carried out during 2009 -2010, sponsored and guided by a national Steering Committee composed of senior South Africa officials and other leading national figures. It was part of a larger international project led by R 4 D which included the estimation of global costs. It aimed to estimate the long-term costs of various response scenarios till 2031. 2
 Methodology • Developed epi baseline & 3 scenarios to 2031 – SPECTRUM parameterised to ASSA outputs to 2016 • Collected, reviewed and verified existing costing studies (unit costs) – limited from private sector • Obtained current coverage rates for every intervention • Received input from the project Steering Committee on current coverage and target rates • Agreed on program scale up scenarios with Steering Committee 3
Methodology • Developed epi baseline & 3 scenarios to 2031 – SPECTRUM parameterised to ASSA outputs to 2016 • Collected, reviewed and verified existing costing studies (unit costs) – limited from private sector • Obtained current coverage rates for every intervention • Received input from the project Steering Committee on current coverage and target rates • Agreed on program scale up scenarios with Steering Committee 3
 Cost and Epi Projections – for each scenario • Epidemiological impact assessed") Methodology (continued) Cost and Epi Projections – for each scenario • Epidemiological impact assessed (incidence, mortality, need for treatment, numbers on ART) using Spectrum with Goals • Costs estimated using Resource Needs Model (Futures) § Resource requirements by program area and intervention § For ART & PMTCT incorporated BU-HERO estimates (Meyer Rath, 09) – note that the ART costs have been further adjusted based on the new Tender prices, which will reduce the cost estimates presented here. 4
Methodology (continued) Cost and Epi Projections – for each scenario • Epidemiological impact assessed (incidence, mortality, need for treatment, numbers on ART) using Spectrum with Goals • Costs estimated using Resource Needs Model (Futures) § Resource requirements by program area and intervention § For ART & PMTCT incorporated BU-HERO estimates (Meyer Rath, 09) – note that the ART costs have been further adjusted based on the new Tender prices, which will reduce the cost estimates presented here. 4
 The South African Scenarios 1. Narrow NSP by 2011 2. Expanded NSP by 2021 3. Hard Choices by 2015 Baseline (maintaining current coverage as comparator) 5
The South African Scenarios 1. Narrow NSP by 2011 2. Expanded NSP by 2021 3. Hard Choices by 2015 Baseline (maintaining current coverage as comparator) 5
 Scenario 1 – Narrow NSP Political will to achieve universal access is strong Rapid scaling-up of prevention & treatment • Achieving key NSP targets by 2011 • ART – old WHO regime and 200 CD 4 criteria • PMTCT single dose till 2009, replaced by dual therapy • Early paediatric ART from 2009 • No male circumcision 6
Scenario 1 – Narrow NSP Political will to achieve universal access is strong Rapid scaling-up of prevention & treatment • Achieving key NSP targets by 2011 • ART – old WHO regime and 200 CD 4 criteria • PMTCT single dose till 2009, replaced by dual therapy • Early paediatric ART from 2009 • No male circumcision 6
 Scenario 2 – Expanded NSP Achievement of all NSP & extra targets by 2021 • ART – new regime & CD 4 350 eligibility from 2010, 90% reached by 2015/6 • MC introduced 2010, reaching 90% by 2021 • Expanded workplace programmes, education and behaviour change • Mobilization and higher coverage for CSW & MSM • Expanded efforts for youth-out-of-school • Programs to reduce violence against women • Expanded mitigation interventions 7
Scenario 2 – Expanded NSP Achievement of all NSP & extra targets by 2021 • ART – new regime & CD 4 350 eligibility from 2010, 90% reached by 2015/6 • MC introduced 2010, reaching 90% by 2021 • Expanded workplace programmes, education and behaviour change • Mobilization and higher coverage for CSW & MSM • Expanded efforts for youth-out-of-school • Programs to reduce violence against women • Expanded mitigation interventions 7
 Scenario 3 – Hard Choices Resources are limited, focus on scaling up to high levels the most effective prevention interventions; some other prevention and social programs reduced; targets achieved by 2015: • same ART effort as under Narrow NSP • Increased coverage for Youth in school, condoms, male circumcision, SW & MSMs, STI treatment • Maintaining current coverage for VCT & FCG • Reduction below NSP targets for: mass media, youthout of-school, workplace, HBC, palliative care, food parcels, uniforms • Mitigation efforts significantly reduced 8
Scenario 3 – Hard Choices Resources are limited, focus on scaling up to high levels the most effective prevention interventions; some other prevention and social programs reduced; targets achieved by 2015: • same ART effort as under Narrow NSP • Increased coverage for Youth in school, condoms, male circumcision, SW & MSMs, STI treatment • Maintaining current coverage for VCT & FCG • Reduction below NSP targets for: mass media, youthout of-school, workplace, HBC, palliative care, food parcels, uniforms • Mitigation efforts significantly reduced 8
 Estimated Epidemiological Impact 9
Estimated Epidemiological Impact 9
 10
10
 HIV Prevalence (2000– 2031) 12") Adult (15+yrs) HIV Prevalence (2000– 2031) 12
Adult (15+yrs) HIV Prevalence (2000– 2031) 12
 13
13
 14") Infant HIV-related Deaths (1993 – 2031) 14
Infant HIV-related Deaths (1993 – 2031) 14
 Key points from the Epi-projections 1. Only the expanded NSP will halve the new infections, as per the NSP goal, but only by 2020. 2. Compared to Baseline, the expanded NSP will avert nearly 6, 000 infections in total by 2031, where as continuing with the current NSP will only avert 3, 000 – half! 3. With increasing treatment coverage, HIV prevalence is unlikely to reduce below 10%, best case scenario. 4. Numbers on treatment will continue to grow, up to 3 million by 2018, but thereafter will start to decrease with the expanded NSP & the expanded prevention efforts. 5. PMTCT will significantly reduce infant mortality, in all scenarios since same coverage. 16
Key points from the Epi-projections 1. Only the expanded NSP will halve the new infections, as per the NSP goal, but only by 2020. 2. Compared to Baseline, the expanded NSP will avert nearly 6, 000 infections in total by 2031, where as continuing with the current NSP will only avert 3, 000 – half! 3. With increasing treatment coverage, HIV prevalence is unlikely to reduce below 10%, best case scenario. 4. Numbers on treatment will continue to grow, up to 3 million by 2018, but thereafter will start to decrease with the expanded NSP & the expanded prevention efforts. 5. PMTCT will significantly reduce infant mortality, in all scenarios since same coverage. 16
 Estimated Resource Requirements 17
Estimated Resource Requirements 17
 NB. These estimations include all") Total HIV/AIDS Costs by Scenario (2009 -2031, ZAR Billions) NB. These estimations include all sectors and all sources of funding DRAFT-do not copy or disseminate 18
Total HIV/AIDS Costs by Scenario (2009 -2031, ZAR Billions) NB. These estimations include all sectors and all sources of funding DRAFT-do not copy or disseminate 18
 20") Expanded NSP – Total Resources Required and their Distribution (ZAR billions) 20
Expanded NSP – Total Resources Required and their Distribution (ZAR billions) 20
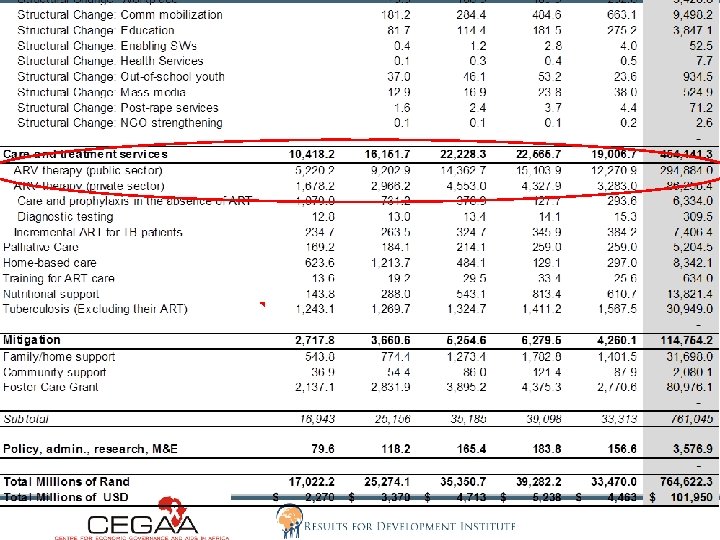
 DRAFT-do not copy or disseminate 21") Expanded NSP – Programme Disaggregation (ZAR billions) DRAFT-do not copy or disseminate 21
Expanded NSP – Programme Disaggregation (ZAR billions) DRAFT-do not copy or disseminate 21
 Expanded NSP delivery
Expanded NSP delivery
 Cost Implications 1. With Expanded NSP costs will double from 2010 to 2021 (but will be significantly reduced with new tender prices, should allow for all on at 350 CD 4 – greater prevention effects) 2. But thereafter they start to decrease significantly. Treatment taking 60% by 2020, but thereafter reducing. 3. Largest proportion will be DOH responsibility for the delivery of public ART – therefore important to increase the role of businesses in provision of ART and PMTCT. 4. Workplace programmes are important for other prevention interventions & Private sector important. 5. The role of NGOs could be expanded.
Cost Implications 1. With Expanded NSP costs will double from 2010 to 2021 (but will be significantly reduced with new tender prices, should allow for all on at 350 CD 4 – greater prevention effects) 2. But thereafter they start to decrease significantly. Treatment taking 60% by 2020, but thereafter reducing. 3. Largest proportion will be DOH responsibility for the delivery of public ART – therefore important to increase the role of businesses in provision of ART and PMTCT. 4. Workplace programmes are important for other prevention interventions & Private sector important. 5. The role of NGOs could be expanded.
 Sustainable Funding Sources? 25
Sustainable Funding Sources? 25
 Sources of Financing for HIV/AIDS in SA • • • No SA NASA yet to ascertain current spending trends of all sectors (public, external & private). No comprehensive database of external sources (some from Burlington (2009). No database of business sector CSI activities (some from Trilogue) Budgetary allocations show national spending, conditional grants to provinces & some provincial voted allocations – limited disaggregation. OOPE – unknown. Development partners appear uneasy to share their longer-term commitments to HIV/AIDS in SA? DPs also struggle to provide year-specific expenditures by province. Business sector is not willing to share their expenditure for the NASA process. Therefore impossible to measure the projected financing gap. 26
Sources of Financing for HIV/AIDS in SA • • • No SA NASA yet to ascertain current spending trends of all sectors (public, external & private). No comprehensive database of external sources (some from Burlington (2009). No database of business sector CSI activities (some from Trilogue) Budgetary allocations show national spending, conditional grants to provinces & some provincial voted allocations – limited disaggregation. OOPE – unknown. Development partners appear uneasy to share their longer-term commitments to HIV/AIDS in SA? DPs also struggle to provide year-specific expenditures by province. Business sector is not willing to share their expenditure for the NASA process. Therefore impossible to measure the projected financing gap. 26
 27") SA Public HIV/AIDS Budget Allocations (2006/07 -2012/13) 27
SA Public HIV/AIDS Budget Allocations (2006/07 -2012/13) 27
 28") Rough Questimate of Total Resource Gap (for all actors, not only public) 28
Rough Questimate of Total Resource Gap (for all actors, not only public) 28
 29") SA DOH Budget Allocations for HIV/AIDS (ZAR millions) 29
SA DOH Budget Allocations for HIV/AIDS (ZAR millions) 29
 Rough Guestimate of public ART shortfall, assuming 90% coverage by 2015 30
Rough Guestimate of public ART shortfall, assuming 90% coverage by 2015 30
 31") Importance of the National AIDS Spending Assessment (NASA) 31
Importance of the National AIDS Spending Assessment (NASA) 31
 Objectives of NASA in South Africa For the years 2007/08, 2008/09 & 2009/10, to identify in each province: All the sources (public, external and private) of financing for HIV/AIDS and TB The providers of the HIV/AIDS and TB services The activities services delivered – and their alignment with the PSP priorities The beneficiaries of the services In order to make recommendations for the improved targeting of funds and efficiency of spending, according to the provincial priorities. 32 DRAFT - DO NOT DISSEMINATE.
Objectives of NASA in South Africa For the years 2007/08, 2008/09 & 2009/10, to identify in each province: All the sources (public, external and private) of financing for HIV/AIDS and TB The providers of the HIV/AIDS and TB services The activities services delivered – and their alignment with the PSP priorities The beneficiaries of the services In order to make recommendations for the improved targeting of funds and efficiency of spending, according to the provincial priorities. 32 DRAFT - DO NOT DISSEMINATE.
 Methodology Aimed to include data from all sources, from all agents and from sampled service providers. All DOE, DSD, DOH expenditure by activity and service provider – from BAS records. Wellness programme spending – included all departments but challenge of coding of HIV-related in BAS records. All NGOs receiving DOH/ DSD/ EU/ PEPFAR grants – sampled others (but nothing received). Districts & Municipalities – most included Donors – Most - EU, GF, UN agencies (NB PEPFAR limitations excl) – pending other donors Private - Businesses - limited response. Medical aid estimates incld. Limited research activities 90% public, 80% external, 80% NGOs & almost no business • • • 33
Methodology Aimed to include data from all sources, from all agents and from sampled service providers. All DOE, DSD, DOH expenditure by activity and service provider – from BAS records. Wellness programme spending – included all departments but challenge of coding of HIV-related in BAS records. All NGOs receiving DOH/ DSD/ EU/ PEPFAR grants – sampled others (but nothing received). Districts & Municipalities – most included Donors – Most - EU, GF, UN agencies (NB PEPFAR limitations excl) – pending other donors Private - Businesses - limited response. Medical aid estimates incld. Limited research activities 90% public, 80% external, 80% NGOs & almost no business • • • 33
 Business sector HIV activities in SA MISSING……. ? ? 34
Business sector HIV activities in SA MISSING……. ? ? 34
 Estimating & Securing Resource Requirements 1. 2. Ø Ø Using estimates of the future costs of an expanded NSP Comparing current spending per intervention More detailed and accurate financing gaps can be calculated Sustainable resources mobilised This requires all partners to: • participate more actively in the achievement of the Expanded NSP • be transparent about their current and future funding activities What are the HIV services currently being provided / funded by business? How could these be expanded? What does government need to do to encourage business sector involvement? 35
Estimating & Securing Resource Requirements 1. 2. Ø Ø Using estimates of the future costs of an expanded NSP Comparing current spending per intervention More detailed and accurate financing gaps can be calculated Sustainable resources mobilised This requires all partners to: • participate more actively in the achievement of the Expanded NSP • be transparent about their current and future funding activities What are the HIV services currently being provided / funded by business? How could these be expanded? What does government need to do to encourage business sector involvement? 35
 Acknowledgements WEBSITE: WWW. CEGAA. ORG SANAC, PACs, HASTs, etc UNAIDS Mark Blecher, National Treasury Drs Pillay & Mbengashe (NDOH) aids 2031 Steering Committee Gesine Meyer-Rath & Lawrence Long, BU/HERO Kelsey Case, Imperial College London John, Lori & Steve, Futures Institute Leigh Johnson, UCT Susan Cleary, UCT Steve Cohen, SDC All the Do. H departments that provided data The teams at CEGAA and Results for Development Institute 36
Acknowledgements WEBSITE: WWW. CEGAA. ORG SANAC, PACs, HASTs, etc UNAIDS Mark Blecher, National Treasury Drs Pillay & Mbengashe (NDOH) aids 2031 Steering Committee Gesine Meyer-Rath & Lawrence Long, BU/HERO Kelsey Case, Imperial College London John, Lori & Steve, Futures Institute Leigh Johnson, UCT Susan Cleary, UCT Steve Cohen, SDC All the Do. H departments that provided data The teams at CEGAA and Results for Development Institute 36